Angle EHPhiladelphia: White Dental Manufacturing Company; 1907
Postlethwaite K The range and effectiveness of safety headgear products. Eur J Orthod. 1989; 11:228-234
Samuels R, O'Neill J, Bhavra G, Hills D, Thomas P, Hug H A clinical evaluation of a locking orthodontic facebow. Am J Orthod Dentofacial Orthop. 2000; 117:344-350
Graber LW Chin cup therapy for mandibular prognathism. Am J Orthod. 1977; 72:23-41
Baek S-H, Kim K-W, Choi J-Y New treatment modality for maxillary hypoplasia in cleft patients. Angle Orthod. 2010; 80:783-791
Delaire J Maxillary development revisited: relevance to the orthopaedic treatment of Class III malocclusions. Eur J Orthod. 1997; 19:289-311
Brandão M, Pinho HS, Urias D Clinical and quantitative assessment of headgear compliance: a pilot study. Am J Orthod Dentofacial Orthop. 2006; 129:239-244
Cureton SL, Regennitter FJ, Yancey JM The role of the headgear calendar in headgear compliance. Am J Orthod Dentofacial Orthop. 1993; 104:387-394
Kuroda S, Yamada K, Deguchi T, Kyung H-M, Takano-Yamamoto T Class II malocclusion treated with miniscrew anchorage: comparison with traditional orthodontic mechanics outcomes. Am J Orthod Dentofacial Orthop. 2009; 135:302-309
Bowden DE Theoretical considerations of headgear therapy: a literature review. 2. Clinical response and usage. Br J Orthod. 1978; 5:173-181
Taner TU, Yukay F, Pehlivanoglu M, Çakırer B A comparative analysis of maxillary tooth movement produced by cervical headgear and pend-X appliance. Angle Orthod. 2003; 73:686-691
Tanne K, Matsubara S, Sakuda M Stress distributions in the maxillary complex from orthopedic headgear forces. Angle Orthod. 1993; 63:111-118
Tortop T, Yüksel S Treatment and posttreatment changes with combined headgear therapy. Angle Orthod. 2007; 77:857-863
Atherton G, Glenny A-M, O'Brien K Development and use of a taxonomy to carry out a systematic review of the literature on methods described to effect distal movement of maxillary molars. J Orthod. 2002; 29:211-216
Firouz M, Zernik J, Nanda R Dental and orthopedic effects of high-pull headgear in treatment of Class II, division 1 malocclusion. Am J Orthod Dentofacial Orthop. 1992; 102:197-205
Melsen B, Dalstra M Distal molar movement with Kloehn headgear: is it stable?. Am J Orthod Dentofacial Orthop. 2003; 123:374-378
Proffit WR, Fields HW, Sarver DM, 4th edn. St Louis: Elsevier Health Sciences; 2006
Leonardi M, Armi P, Franchi L, Baccetti T Two interceptive approaches to palatally displaced canines: a prospective longitudinal study. Angle Orthod. 2004; 74:581-586
Parkin N, Furness S, Shah A, Thind B, Marshman Z, Glenroy G Extraction of primary (baby) teeth for unerupted palatally displaced permanent canine teeth in children. Cochrane Database Syst Rev. 2012; 12
Kurol J, Bjerklin K Treatment of children with ectopic eruption of the maxillary first permanent molar by cervical traction. Am J Orthod. 1984; 86:483-492
Perez CA, de Alba JA, Caputo AA, Chaconas SJ Canine retraction with J hook headgear. Am J Orthod. 1980; 78:538-547
Holmes A, Nashed R, O'Keeffe C The correction of dental centre line discrepancies using an edgewise appliance. J Orthod. 1989; 16:271-276
Hershey HG, Houghton C, Burstone CJ Unilateral face-bows: a theoretical and laboratory analysis. Am J Orthod. 1981; 79:229-249
Brosh T, Portal S, Sarne O, Vardimon AD Unequal outer and inner bow configurations: comparing 2 asymmetric headgear systems. Am J Orthod Dentofacial Orthop. 2005; 128:68-75
Jacobson A A key to the understanding of extraoral forces. Am J Orthod. 1979; 75:361-386
Martina R, Viglione G, Teti R Experimental force determination in asymmetric face-bows. Eur J Orthod. 1988; 10:72-75
Keeling SD, Wheeler TT, King GJ, Garvan CW, Cohen DA, Cabassa S Anteroposterior skeletal and dental changes after early Class II treatment with bionators and headgear. Am J Orthod Dentofacial Orthop. 1998; 113:40-50
Tulloch JFC, Phillips C, Koch G, Proffit WR The effect of early intervention on skeletal pattern in Class II malocclusion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 1997; 111:391-400
Tulloch J, Phillips C, Proffit WR Benefit of early Class II treatment: progress report of a two-phase randomized clinical trial. Am J Orthod Dentofacial Orthop. 1998; 113:62-74
Mandall N, DiBiase A, Littlewood S, Nute S, Stivaros N, McDowall R Is early Class III protraction facemask treatment effective? A multicentre, randomized, controlled trial: 15-month follow-up. J Orthod. 2010; 37:149-161
Mandall N, Cousley R, DiBiase A, Dyer F, Littlewood S, Mattick R Is early Class III protraction facemask treatment effective? A multicentre, randomized, controlled trial: 3-year follow-up. J Orthod. 2012; 39:176-185
Masucci C, Franchi L, Defraia E, Mucedero M, Cozza P, Baccetti T Stability of rapid maxillary expansion and facemask therapy: a long-term controlled study. Am J Orthod Dentofacial Orthop. 2011; 140:493-500
Watkinson S, Harrison J, Furness S, Worthington H Treatment for prominent lower front teeth in children. Cochrane Database Syst Rev. 2013; 9
Parkin NA, McKeown HF, Sandler PJ Comparison of 2 modifications of the Twin-block appliance in matched Class II samples. Am J Orthod Dentofacial Orthop. 2001; 119:572-577
Lentini-Oliveira D, Carvalho F, Qingsong YE, Junjie L, Saconato H, Machado M Orthodontic and orthopaedic treatment for anterior open bite in children. Cochrane Database Syst Rev. 2007; 2
Bowden DE Theoretical considerations of headgear therapy: a literature review. 2. Clinical response and usage. Br J Orthod. 1978; 5:173-181
Poulton DR The influence of extraoral traction. Am J Orthod. 1967; 53:8-18
Barton JJ High-pull headgear versus cervical traction: a cephalometric comparison. Am J Orthod. 1972; 62:517-529
Wieslander L, Tandläkare L The effect of orthodontic treatment on the concurrent development of the craniofacial complex. Am J Orthod. 1963; 49:15-27
Turner P Extra-oral traction. Dent Update. 1991; 18:197-203
Baccetti T, McGill JS, Franchi L, McNamara JA, Tollaro I Skeletal effects of early treatment of Class III malocclusion with maxillary expansion and face-mask therapy. Am J Orthod Dentofacial Orthop. 1998; 113:333-343
Ngan P, Hägg U, Yiu C, Merwin D, Wei SH Soft tissue and dentoskeletal profile changes associated with maxillary expansion and protraction headgear treatment. Am J Orthod Dentofacial Orthop. 1996; 109:38-49
Deguchi T, Kuroda T, Minoshima Y, Graber TM Craniofacial features of patients with Class III abnormalities: growth-related changes and effects of short-term and long-term chincup therapy. Am J Orthod Dentofacial Orthop. 2002; 121:84-92
Abdelnaby YL, Nassar EA Chin cup effects using two different force magnitudes in the management of Class III malocclusions. Angle Orthod. 2010; 80:957-962
Yoshida N, Jost-Brinkmann P-G, Yamada Y Initial tooth movement under extraoral force and considerations for controlled molar movement. Angle Orthod. 1995; 65:199-208
Deguchi T, Murakami T, Kuroda S, Yabuuchi T, Kamioka H, Takano-Yamamoto T Comparison of the intrusion effects on the maxillary incisors between implant anchorage and J-hook headgear. Am J Orthod Dentofacial Orthop. 2008; 133:654-660
Samuels RH, Willner F, Knox J, Jones ML A national survey of orthodontic facebow injuries in the UK and Eire. Br J Orthod. 1996; 23:11-20
Holland GN, Wallace DA, Mondino BJ, Cole SH, Ryan SJ Severe ocular injuries from headgear. Am J Orthod. 1986; 89
British Orthodontics Society.
Kerosuo HM, Dahl JE Adverse patient reactions during orthodontic treatment with fixed appliances. Am J Orthod Dentofacial Orthop. 2007; 132:789-795
Travess H, Roberts-Harry D, Sandy J Orthodontics. Part 6: Risks in orthodontic treatment. Br J Orthod. 2004; 196:71-77
Rahilly G, Price N Current products and practice nickel allergy and orthodontics. J Orthod. 2003; 30:171-174
Extra-oral appliances are used in orthodontics to apply forces to the jaws, dentition or both and the popularity of these appliances is cyclical. Although the use of retraction headgear for the management of Class II malocclusion has declined over the last 20 years with the refinement of non-compliance approaches, including temporary anchorage devices, headgear still has a useful role in orthodontics. The use of protraction headgear has increased as more evidence of its effectiveness for the treatment of Class III malocclusion has become available. This paper describes the mechanics and contemporary uses of headgear in orthodontics for primary care dentists and specialist orthodontists.
CPD/Clinical Relevance: Extra-oral appliances have specific uses in orthodontic biomechanics. Clinicians using retraction headgear and protraction headgear should be familiar with their clinical indications, the potential problems and how these can be avoided.
Article
Extra-oral forces used in orthodontic treatment require the use of headgear. After the introduction of retraction headgear by Norman W Kingsley in the late 1800s, headgear use increased with the popularization of the first generation of fixed appliances and retraction headgear by Edward H Angle. Retraction headgear use reduced dramatically in the 1920s with the introduction of intra-oral elastics as these were believed to provide equivalent forces.1 In the 1940s, the increasing use of cephalometric radiography in orthodontics led to concerns about the adverse effects of intra-oral elastic traction, including proclination of lower incisors and retroclination of upper incisors. As a result, headgear use increased again. Although the use of retraction headgear has declined steadily with the introduction of the non-compliance fixed appliance, distalizing appliances, including the pendulum appliance, lip bumper appliances and temporary anchorage devices (TADs), headgear remains the standard for anchorage reinforcement and maxillary arch distalization. Enthusiasm is increasing for the use of protraction headgear for the treatment of Class III malocclusion and patients affected by hypodontia where space closure may result in a reverse overjet.
There are a variety of clinical uses for headgear, requiring different directions of forces, force levels and wear levels which result in varying effects on the dentition and/or skeletal base relationships.
Components of extra-oral appliance
In this article, the contemporary uses and effectiveness of extra-oral traction appliances are discussed.
There are four main components:
Extra-oral unit;
Force delivery system;
Intermediate/connecting component;
Intra-oral component.
Extra-oral unit
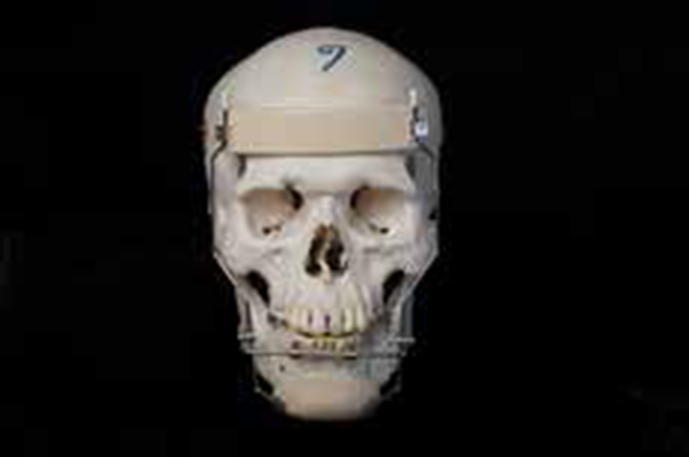
This part of the appliance provides the anchorage for the extra-oral force in a form of headcap (Figure 1), neckpad/strap or chin cup (for retraction headgear) or a facemask (for protraction headgear). Retraction headgear normally includes the delivery force system in the headcap/neckpad/strap.
Figure 1. Headcap for retraction headgear.
Force delivery system
This can involve either a spring-loaded device (Figure 2) or heavy-force, extra-oral elastic. The former is used with retraction headgear and chin cup appliances while the latter is commonly used with protraction facemask appliances.
Figure 2. Force-delivery module (snap-away) for retraction headgear (open and closed).
Intermediate/connecting component
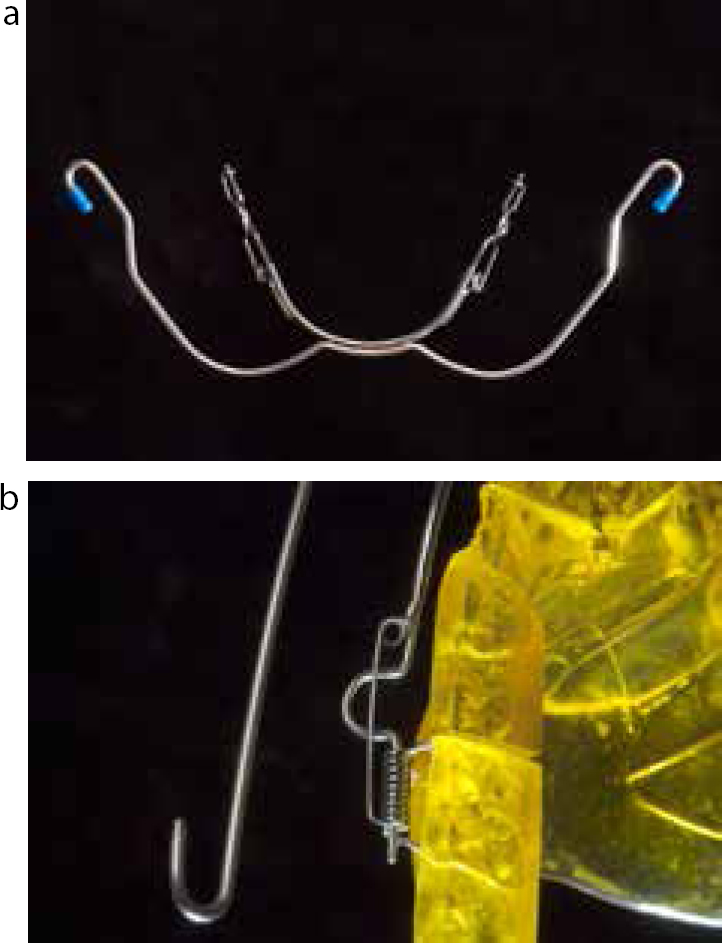
This transmits the force to the teeth and underlying skeleton and connects the extra-oral and intra-oral components. With retraction headgear, the intermediate component is the outer part of the facebow that is welded/soldered to the inner part (inner bow) of the extra-oral component. The inner bow should also incorporate a robust safety mechanism to prevent an accidental disengagement2,3 (Figure 3a, b).
Figure 3. Locking facebow (a) closed (b) attached to clasp of upper removable appliance.
Intra-oral component
Retraction headgear is attached via the headgear facebow to either fixed, removable or functional appliances for either anchorage reinforcement or molar distal movement. With a fixed appliance (Figure 4), the inner bow inserts into molar bands using welded headgear tubes which are either gingivally placed (close to the centre of tooth rotation) or occlusally positioned (for better access during insertion and removal). With removable appliances (Figure 5), the facebow either inserts into tubes soldered to the molar clasps or to coils wound as part of the clasps (Figure 3b). Headgear tubes can also be incorporated into the acrylic of a functional appliance for orthopaedic force delivery. The only headgear appliance that has no intra-oral component is the chin-cup appliance.4 When using a protraction facemask, the intra-oral component is either a fixed or removable appliance with many operators simultaneously treating the patient with slow maxillary expansion (using a quad helix appliance) or rapid maxillary expansion (RME).5,6
Figure 4. Retraction headgear fitted to a fixed appliance.Figure 5. Retraction headgear fitted to a removable appliance.
Uses of extra-oral appliances in clinical orthodontics
The effectiveness of headgear depends entirely on patient compliance in wearing the appliance and it is well-known that patients usually overestimate the time for which headgear is worn.7 As headgear is not worn full-time, the intermittent force delivery is a biomechanical disadvantage, with relapse occurring when the appliance is not worn. Headgear charts, timers and award systems have been proposed to improve compliance and success rates.8 There are different levels of force and duration of use according to the clinical application (Table 1).
Force levels (gram/side)
Duration (hour/per day)
Anchorage
250-300
10
Tooth movement
300-350
12-14
Orthopaedic movement
450-600
14-16
Anchorage reinforcement
Retraction headgear can be used for anchorage reinforcement antero-posteriorly and vertically. Although headgear is considered to be a good method of anchorage reinforcement, TADs have been shown to provide equivalent results with minimal patient co-operation.9 For anchorage reinforcement, force levels of 250–300 g per side are required for a minimum of 10 hours/day, on average.10,11,12,13,14
Molar distalization
Retraction headgear can distalize the molars by up to ½ a molar unit (approximately 5 mm) which can be useful when used for correction of a Class II molar relationship and relief of crowding on a non-extraction basis or reduction of an increased overjet.15,16,17,18 Molar distalization using headgear in conjunction with extraction of the deciduous canine in order to provide space for ectopic permanent maxillary canines has been shown to have a success rate of 80%, in comparison to 50% where the deciduous canine was extracted as an isolated measure.19 However, the Cochrane review by Parkin et al has shown that there is no high-quality evidence to justify the interceptive effect of extraction of primary canines.20 Headgear can also be used to upright impacted upper first molars and to regain lost space after premature loss of primary teeth.21 Force levels of 400–500 g/side used over a period of 12–14 hours/day are necessary for distalization.10 Headgear use can tip and extrude the molars, depending on the magnitude and direction of the applied force as well as the duration of headgear wear.11,12,13
Canine retraction/labial segment movement
J-hook headgear has historically been used to intrude upper anterior teeth, retract maxillary canines individually or, rarely, retract lower canines.22 Force levels of 250–300 g per side are required for a minimum of 10 hours/day, on average.10 Owing to the risk of ocular trauma, and as canine retraction is more easily achieved with sliding mechanics when using contemporary fixed appliances, J-hook headgear is no longer used.
Differential (asymmetric) tooth movement
Asymmetric movement of the molars can be achieved using asymmetrical headgear (AHG).23 There are many designs for AHG but the main principle of action is Castagliano's Theorum, which involves greater movement on one side due to a longer outer bow or heavier force on this side. The variety of designs of AHG include the power-arm facebow, soldered-offset facebow, swivel-offset facebow and spring-attachment facebow.24,25,26 One of the disadvantages of AHG is the tendency to produce a crossbite on the side of the long arm and an increase in difficulty when fitting the appliance.27 Force levels of 250–300 g per side are required for a minimum of 10 hours/day, on average.11,12,13
Growth modification
Class II malocclusion
Theoretically, headgear can alter the skeletal relationship, due to a restriction of maxillary forward and downward growth that allows the mandible to 'catch up' during treatment, when used in growing children aged 12–13 years.28,29 However, most of the skeletal improvement has been shown to be lost 1 year after treatment.28,30
Class III malocclusion
Enthusiasm for the use of protraction facemask for the treatment of cases with a Class III incisor relationship is increasing. Studies have found that the facemask may provide an orthopaedic effect in growing patients, with an improvement in the ANB angle by an average of 2.6 degrees when compared to a control group.31 Unlike the loss of the skeletal improvement with retraction headgear in Class II cases over time, the skeletal results with protraction headgear are generally stable after 3 years of treatment.32 Although investigators have found that relapse can occur up to 8.5 years after treatment,33 a protraction facemask is now the treatment of choice for mild to moderate Class III malocclusions.34
Anterior open bite
High-pull headgear combined with a twin block, monoblock or Dynamax appliance can be used to treat high angle Class II malocclusions.35 However, the evidence for the effect of headgear on the vertical dimension is weak as Oliveira et al found only a limited improvement in anterior open bite when treated with a palatal crib and headgear.36 Force levels of 400–500 g/side used over a period of 12–14 hours/day are recommended for a skeletal effect.10
Headgear types
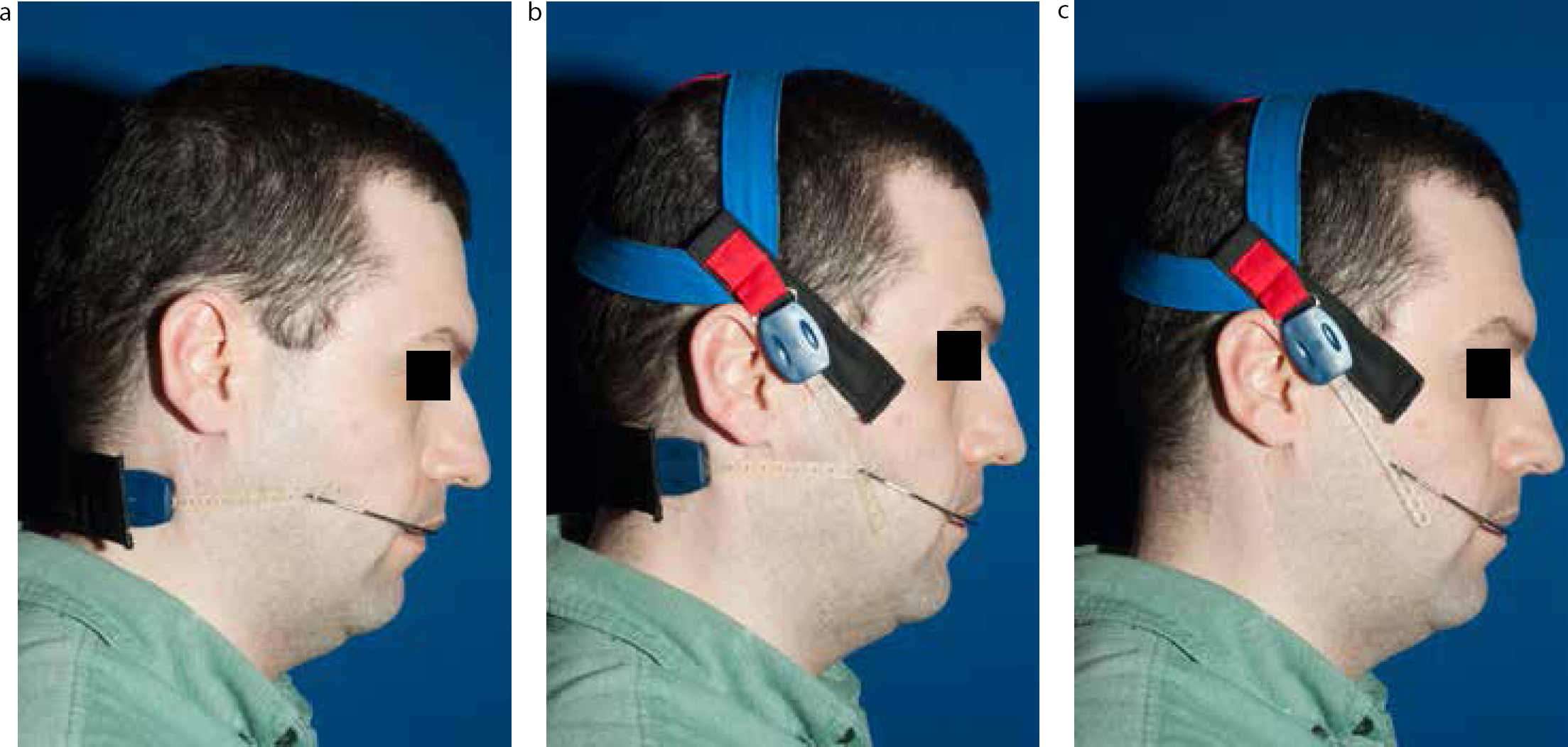
Headgear is categorized according to the antero-posterior direction of pull: if the force is directed distally, then the headgear is called retraction and, where the force is mesially directed, it is called protraction headgear. Retraction headgear is also classified according to the direction of force above, at, or below the occlusal plane: high pull, straight/combination pull and low or cervical pull.
Figure 6.
(a) Low-pull, (b) straight/combination-pull and (c) high-pull headgear.
This type of headgear is frequently referred to as cervical traction and is the most commonly used headgear appliance.37 Cervical traction is used mainly for the correction of low angle Class II malocclusion by restraining the forward growth of the maxilla.38 Cervical traction is believed to have a reciprocal effect on the growth of the mandible as well as extrusion of maxillary molars.39 This latter effect results in a clockwise mandibular rotation, thus cervical headgear is indicated mainly for growing children with a deep overbite.39,40
This is a hybrid of high pull and low pull, theoretically producing a pure distal movement without any extrusion or intrusion of the molars.37 The forces are transmitted to the teeth through a combination of a head cap and a neck strap.23
High-pull headgear produces forces that pass apically through the centre of resistance of the maxillary teeth producing intrusive forces to the molars, which can therefore help the correction of an anterior open bite.39 Occipital headgear has orthopaedic effects on the maxilla by restraining its vertical growth.37 Although wearing high pull headgear can result in compensatory eruption of the mandibular molars, this can be controlled by using a fixed lingual arch.
J-Hook
High pull
This type of headgear exerts an intrusive and distal action on the upper incisors which moves the teeth distally as well as gingivally.37
Straight/combination pull
This is used to retract mandibular or maxillary canines distally. However, the force vector can cause downward tipping of the incisors.37
Low pull
This type of headgear intrudes and retracts the mandibular incisors to camouflage a Class III skeletal base relationship.37 It is worth noting that the use of J-Hook headgear in the UK is obsolete due to safety concerns about potential ocular injuries.
This is also called a facemask or reverse headgear. Facemask therapy is an effective orthopaedic appliance for growing children in order to correct a Class III malocclusion through forward movement of the maxilla.41 The results of treatment are better in the early mixed dentition than in the late mixed dentition.42 In addition to the skeletal changes, reverse headgear can result in dental compensation to assist with the correction of a reverse overjet or Class III malocclusion.14,43
Chin-cup
Chin-cup therapy is used to correct Class III malocclusions in growing patients using forces ranging from 250–600 g per side for at least one year. Some researchers have found that chin-cup therapy has dental effects as well as redirecting, inhibiting or slowing condylar growth.44,45 However, as no forces are applied to the maxilla, cases with maxillary hypoplasia will not have any upregulation of maxillary growth when treated with a chin-cup appliance. As a result, chin-cup therapy is seldom used in the UK.
Fitting and monitoring progress with headgear
Retraction
The first step in fitting the retraction headgear involves selecting the correct facebow size. The inner bow should be 1.13 mm while the outer bow is 1.45 mm for maximum rigidity. The facebow should be set parallel to the occlusal plane with slight expansion. The centre of bow should be slightly away and above the central incisor edge. The inner bow should follow the contour of lip and cheeks but not actively displacing them. Each side of the facebow must be adjusted to fit into the fixed appliance molar bands or removable appliance tubes/colis at one side at a time. If the molars are not severely rotated then toe-in bends should be placed. The length of the outer bow, relationship to the centre of rotation, the direction of pull should be carefully selected and adjusted to minimize distal crown tipping. All these factors are important in determining the force vectors and the net force. In particular, if the outer bow is positioned at the trifurcation point of molars, the result will be distal translocation of the molars.10,46
Protraction
With protraction headgear, the fitting procedure starts with adjusting the cams (Figures 7, 8) using the Allen key until they are 15 degrees below the occlusal plane. The elastics are attached to the intra-oral device and should be heavy enough to apply the required force at 30 degree angulation. It is preferable for the elastics to cross-over to avoid lip irritation.31
Monitoring progress with headgear appliances can be undertaken by asking the patient/parent about compliance, using compliance charts,8 assessing the ability of the patient to insert/remove the appliance, checking for physical signs of wear and tear, identifying positive tooth movement in comparison with pre-treatment study models/cephalometry and detecting molar mobility.
Iatrogenic effects of retraction and protraction headgear and solutions to overcome these
There are many iatrogenic effects of extra-oral appliances. These are detailed in Table 2 with solutions that can be used to manage them.
Iatrogenic effect
Frequency
Management
Pain due to heavy force levels
Common
Non-steroidal painkillers
Increased risk of root resorption
Rare possibility with J-hook headgear
Monitor radiographically using long cone periapical radiographs47 Force levels should be as low as possible over a short duration
Trauma to the face and eye
Rare but serious consequences (ophthalmitis and blindness) due to accidental disengagement or recoiling injuries48,49,50
Prevention through:Demonstration of the safe use of the headgear to the patient and parent Verbal and written instructions50Incorporation of safety mechanisms
Nickel allergyContact dermatitis-type IV (delayed hypersensitivity)
30% of female and 3% of male patients undergoing orthodontic treatment51
Confirmation of the nickel allergy by a dermatologistFurther episodes avoided using nickel-free appliances or a plastic shield for the headgear facebow52,53,54
Latex allergy
Infrequent
Latex-free elastic components
Safety mechanisms for retraction headgear
Many safety mechanisms are available to prevent ocular injuries resulting from retraction headgear. These include:
Safety release mechanisms where the headgear is designed to ‘break-away’ when excessive force is applied (Figure 2).54
Safety facebows such as locking mechanisms (Figure 3) (Nitom Locking Facebow, Ortho Kinetics Corporation, Vista, Calif/GAC International Inc, Central Islip, NY) and recurved reverse entry inner bows.2,3
Additional safety mechanics such as blunt ends and locating elastics.2
The British Orthodontic Society (www.bos.org.uk) recommends at least two main safety mechanics are provided with each headgear appliance, as well as informed, written and verbal instructions being given to the patients/parents. It is vital to inform the patient to ensure the safety mechanisms are in place during use. Patients should be advised to avoid wearing their headgear while playing sports and they should stop the use of the headgear and contact their orthodontist immediately if the headgear becomes detached during sleep. Moreover, the patient must be aware that if any ocular injury associated with the headgear occurs, it must be treated as a medical emergency. Lastly, patients should be instructed to bring their headgear to each appointment and report any problems to their orthodontist.50
Conclusion
Retraction headgear remains a useful appliance in contemporary clinical orthodontics. Protraction headgear has both an orthopaedic and orthodontic effect and is a useful appliance for young patients presenting with a Class III malocclusion.