Yengopal V, Harnekar S, Patel N, Siegfried N. Dental fillings for the treatment of caries in the primary dentition. Cochrane Database Syst Revs. 2009; 15
Filstrup SL, Briskie D, da Fonseca M, Lawrence L, Wandera A, Inglehart MR. Early childhood caries and quality of life: child and parent perspectives. Pediatr Dent. 2003; 25:431-440
Guideline on Restorative Dentistry. Clinical Guidelines Reference Manual. 2014; 36:(6)230-241
Kindelan SA, Day P, Nichol R, Willmott N, Fayle SA. UK National Clinical Guidelines in Paediatric Dentistry: stainless steel preformed crowns for primary molars. Int J Paediatr Dent. 2008; 18:20-28
Innes N, Evans D.Dundee: University of Dundee; 2009
Kodaira H, Ohno K, Fukase N, Kuroda M, Adachi S, Kikuchi M, Asada Y. Release and systemic accumulation of heavy metals from preformed crowns used in restoration of primary teeth. J Oral Sci. 2013; 55:(2)161-165
Randall R. Preformed metal crowns for primary and permanent molar teeth: review of the literature. Pediatr Dent. 2002; 24:(5)489-500
Noble J, Ahing SI, Karaaiskos NE, Wiltshire WA. Nickel allergy and orthodontics, a review and report of two cases. Br Dent J. 2008; 204:(6)297-300
Burke FJT, McHugh S, Shaw L, Hosey MT, Macpherson L, Delargy S, Dopheide B. UK dentists' attitudes and behaviour towards Atraumatic Restorative Treatment for primary teeth. Br Dent J. 2005; 199:365-369
Threlfall AG, Pilkington L, Milsom KM, Blinkhorn AS, Tickle M. General dental practitioners' views on the use of stainless steel crowns to restore primary molars. Br Dent J. 2008; 199:(7)453-455
Wong FS, Day SJ. An investigation of factors influencing the longevity of restorations in primary molars. J Int Assoc Dent Child. 1990; 20:(1)11-16
Roberts J, Attari N, Sherriff M. The survival of resin modified glass ionomer and stainless steel crown restorations in primary molars, placed in a specialist paediatric dental practice. Br Dent J. 2005; 198:(7)427-431
Innes N, Ricketts D, Evans D. Preformed metal crowns for decayed primary molar teeth. Cochrane Database Syst Revs. 2007; 1
Qvist V, Johannessen L, Bruun M. Progression of approximal caries in relation to iatrogenic preparation damage. J Dent Res. 1992; 71:(7)1370-1373
Page LA, Boyd DH, Davidson SE, McKay SK, Thompson WM, Innes NP. Acceptability of the Hall Technique to parents and children. N Z Dent J. 2014; 110:(1)12-17
Bell S, Morgan A, Marshman Z, Rodd H. Child and parental acceptance of preformed metal crowns. Eur Arch Paediatr Dent. 2010; 11:(5)218-224
Academic Clinical Fellow in Paediatric Dentistry, Unit of Oral Health and Development, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield, S10 2TA, UK.
This article details the clinical techniques for conventional preformed metal crown placement. It aims to increase the readers' awareness of the clinical advantages of preformed metal crowns and the indications for their use. The second part will discuss the Hall Technique.
CPD/Clinical Relevance: This two-part article aims to guide the reader through the conventional and alternative techniques available for placement of a preformed metal crown whilst providing an update of the evidence for each.
Article
This two-part article will be looking at preformed metal crowns (PMCs), also known as stainless steel crowns (SSCs), which have been in use since the 1950s. They are prefabricated crown forms that can be adapted to individual primary molars as a definitive restoration. In this first part, the indications, evidence and the conventional technique will be described. The second paper will discuss the new and innovative technique for placing these crowns known as the ‘Hall Technique’, together with aesthetic crowns.
Primary teeth in young children are vital to their development as they:1
Are natural space maintainers for permanent teeth;
Help with speech and eating;
Help to provide self-confidence and a good oral health quality of life.
However, the most important reason to restore the primary dentition is the management of caries in children, which can otherwise progress to pain, infection/sepsis and hospital admissions.2
PMCs are widely accepted by paediatric dentists, including the American Association of Paediatric Dentistry (AAPD) and the British Society of Paediatric Dentistry (BSPD) as the restoration of choice for primary molars.3,4
The prognosis is poor due to irreversible pulpal involvement;
The tooth is close to exfoliation (with more than half the roots resorbed);
In a patient with a known nickel allergy or sensitivity;
Patient is pre-cooperative;
Parent or child is unhappy with the aesthetics.
Although PMC is the preferred term, these crowns were traditionally called stainless steel crowns. This is a misnomer, as they are actually nickel chromium. The constituents of 3M ESPE (Seefeld, Germany) preformed metal crowns, the market leader, are as follows:6,7
65–74% iron;
17–19% chromium;
9–3% nickel.
Nickel is one of the constituents and therefore nickel allergy is one of the contra-indications to the use of PMCs. It is suggested that 11% of young female adults and 2% of young male adults are nickel sensitive.8 From the orthodontic literature, it is estimated that only 0.1–0.2% of patients show a harmful response to nickel. This is because it is thought that much greater concentrations of nickel are required intra-orally than on the skin to elicit a reaction. Further, it has been shown that only small amounts of the metal constituents leach from PMCs.6
Evidence supporting the use of PMCs
A questionnaire study of a random sample of general dental practitioners (GDPs) drawn from the Midlands of England and Scotland reported 6% potentially using PMCs to restore primary teeth.9 An interview study the same year of GDPs in the North West of England reported again only 6% placing PMCs.10 In this study, the commonest reasons cited for the low uptake included cost, time consuming to fit and patient co-operation issues. Appearance and parental acceptance were also cited as a concern.
The longevity of preformed metal crowns is their key advantage over multi-surface restorations. One retrospective study conducted in NHS general practice found the 5-year survival rate of conventional technique preformed metal crowns to be 100%; over twice that of the multi-surface amalgams, though the small number of only 18 PMCs sampled is a valid criticism of this study.11 This issue was rectified in a five-year retrospective study, conducted in a private specialist paediatric practice, that found only 2.1% of preformed metal crowns required replacement, compared to 14.7% of Black's Class II amalgams over a 10-year period. A second prospective study conducted in the same specialist practice found very similar survival rates between PMCs and intra-coronal restorations, but the mean follow-up was only just over two years.12
These observational studies have a number of drawbacks and confounders, including a lack of standardization on use of local anaesthetic, variable use of rubber dam and, most importantly, the PMC tended to be selected for larger carious lesions.
This longevity and the consequent reduction in the need for replacement can have significant implications in terms of time- and cost-effectiveness, along with patient and parent satisfaction.
None of these studies is a randomized controlled trial. A Cochrane review on PMCs found that there were no studies that met the inclusion criteria and therefore no relevant data were available for analysis.13 Therefore, no conclusions could be made as to whether PMCs were more successful than alternatives for restoring primary molar teeth. However, ‘it is important that the absence of evidence for PMCs is not misinterpreted as evidence for their lack of efficacy’, especially as the ‘evidence[s] that have been produced … have strength in that the clinical outcomes are consistently in favour of PMCs’.13
Conventional PMC technique
The conventional crown technique requires a good degree of patient co-operation. This is necessary firstly to allow the administration of local anaesthetic.
Step 1 Explanation
Show the crown to the child and his/her carer and describe the procedure (Figure 1).
Figure 1. Show the crown to the patient and carer.
Step 2 Anaesthesia
Local anaesthetic is best provided following application of topical anaesthetic.
Step 3 Tooth preparation
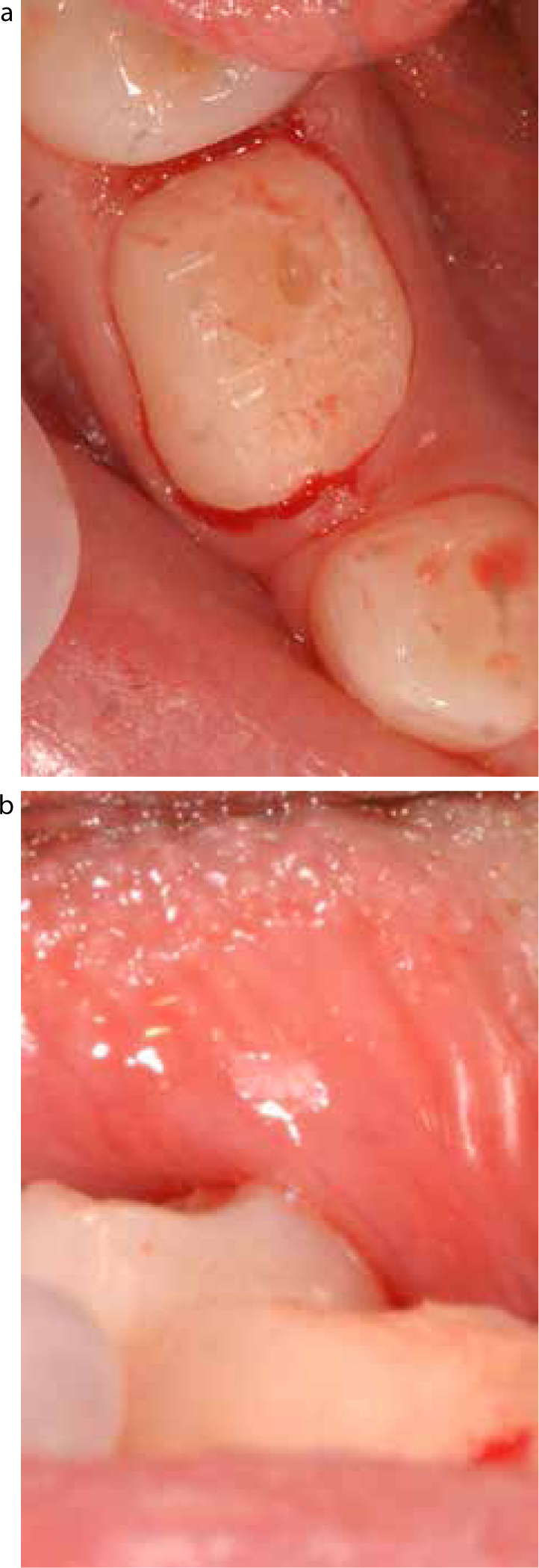
Figure 2 shows a tooth prior to preparation. The tooth is reduced occlusally by 1.5 mm, using a diamond fissure bur. This reduction should take into account the extent of tooth surface loss already present, as further reduction in a tooth already displaying signs of significant erosion or attrition could compromise the pulp further.
Figure 2. A primary tooth with caries prior to tooth preparation.
Approximal reduction is the most technically-challenging aspect of the conventional technique. A visible space should be created with a fine-pointed diamond bur, ensuring that only the enamel of the tooth to be crowned is reduced (Figure 3). The adjacent tooth should not be contacted by the bur, unless, of course, it is to be extracted or crowned in the same treatment session. Even the slightest iatrogenic damage approximally has been shown to increase risk of development of a carious lesion at that site.14 This is clearly highly likely in an existing cariogenic environment.
Figure 3. Approximal reduction of the primary tooth, taking care to avoid iatrogenic damage of adjacent teeth.
Buccal and lingual reduction is not normally required. However, it is frequently necessary to remove the buccal prominence on first primary molars, particularly in the lower arch.
Any remaining caries is then removed (Figures 4a and b). The final preparation should be free of ledges, steps or shoulders, with smooth and rounded edges to facilitate placement of the crown.
Figure 4.
(a) Occlusal view following reduction and caries removal. (b) Buccal view of primary tooth following preparation, showing reduction in height.
Step 4 Crown selection and adaptation
There are two main techniques employed by dentists to select the appropriate choice of crown. The first involves measuring the mesio-distal space with either dividers or a periodontal probe. The second utilizes trial and error, a process which becomes easier with experience.
The crown which adequately restores the space with a snug fit to the tooth should be selected. Occasionally, adjustment may be required in the form of crimping or trimming the crown. The former tends to be required when the tooth requires a crown between two sizes. Crimping of the larger crown to engage interproximally and beneath any bulbosities can often solve the problem (Figures 5a and b). Alternatively, manual adjustment of the crown form can be undertaken simply by squeezing the crown slightly between finger and thumb (Figure 6). Trimming followed by polishing with a stone may be necessary in cases where there is extensive tooth surface loss occlusally, which has reduced the crown height. Trimming should be avoided whenever possible, as this reduces retention and, even with stoning, it can be hard to remove rough sharp edges. Moreover, trimmers should be used as opposed to scissors, as the latter can produce distortion.
Figure 5.
(a) Crimping the crown with size 114 crimping pliers. (b) Crimping the crown with size 112 crimping pliers.Figure 6. Manual adjustment of crown form with finger and thumb.
Step 5 Cementation
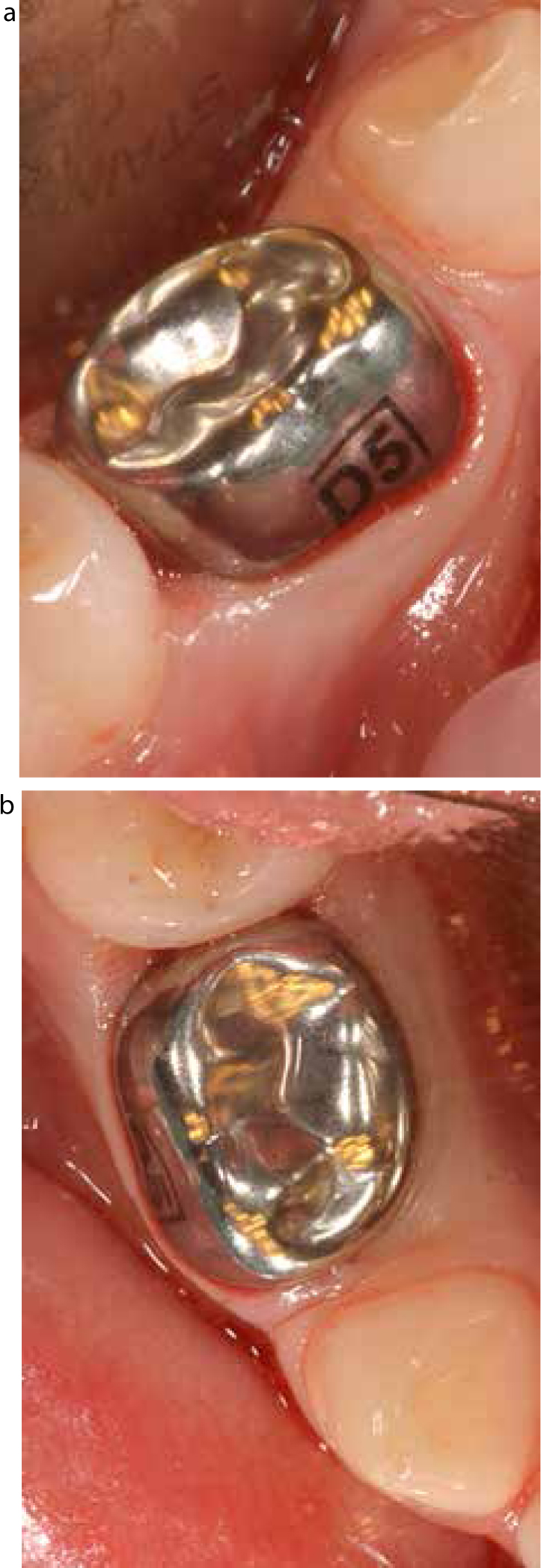
The prepared tooth should then be washed and dried. The crown chosen is generously filled with the luting material and fully seated (Figure 7). Whilst resin-modified glass ionomer cement is reported to have superior bonding properties as a luting agent for PMCs, conventional glass ionomer cements are widely used.7,15 Excess cement should be removed with damp gauze and an instrument; knotted floss passed interproximally may be helpful (Figure 8a and b).
Figure 7. PMC filled with luting cement.Figure 8.
(a) Buccal view of fully seated PMC – note the blanching of the gingivae. (b) Occlusal view of fully seated PMC with excess cement removed.
Consideration must be given to airway protection during both try-in and cementation. This can be done by sitting the patient upright, using a sheet of gauze as a physical barrier or using tape to hold the crown.
Acceptability
Durability, plasticity and malleability are some of the key properties of preformed metal crowns that contribute to their clinical success and ease of use. These properties hail from the metallic components that in turn produce the silver-coloured appearance. Clearly, one would expect aesthetics to be a potential issue for parents and children alike. This issue was noted by Page and colleagues, who sought opinions from both children and their parents on the appearance of their PMC(s).16 Whilst the children interviewed gave generally positive or neutral feedback, a few parents were concerned that their child's PMC would be viewed by adult peers as an indicator of dental neglect. Bell et al's questionnaire study looked at the views of children and their parents, on conventional PMCs and those placed by the Hall Technique in more depth.17 Only 8% of children did not find having the crown placed ‘okay’, and approximately 16% seemed to have concerns about its appearance, particularly other people commenting on it. A small number of parent's (5%) reported strong concerns about the appearance.
For this reason, it is important that parents and children can view a crown, or a photo of a crown, in situ prior to placement and are aware of on which tooth it is planned to be placed.
PMC removal
Rarely, instances may arise where PMC removal is indicated. Reasons for this include:
Trapping of an erupting first permanent molar on the distal surface of a PMC;
Perforation of the PMC occlusal surface due to wear (which is too extensive to be repaired by use of glass-ionomer cement);
Child or parent unhappy with appearance despite discussions prior to placement.
Removal is relatively simple and does not require anaesthesia because the luting cement insulates and protects the tooth.
The technique for crown removal involves:
Cutting into the crown in the middle of the occlusal surface using a fissure diamond bur. At this point, there is a large layer of cement present protecting the tooth from the bur so iatrogenic damage is extremely unlikely (Figure 9);
Move the bur two-thirds of the way towards the lingual surface;
Next extend the cut buccally along the occlusal surface and down the buccal aspect with a pointed diamond bur until the crown has been split. It is at the gingival margin where the crown is closely adapted that iatrogenic damage is more likely to occur. Fortunately, visibility is usually excellent and this can be avoided;
Once the crown is split in this way it can be unpeeled and removed in one piece with an excavator (Figure 10);
The remaining cement is then easily removed.
Figure 9. Layer of luting cement protecting the tooth from iatrogenic damage during removal of a PMC from a first permanent molar.Figure 10. When the PMC is split it can be peeled away from the tooth.
Tooth-coloured crowns
As discussed, aesthetics is an issue with PMCs. In the past it has been suggested that, following placement, a window could be cut in the buccal surface of the crown to improve its aesthetics. This compromises the PMC integrity and has a limited improvement on aesthetics. Therefore, anterior and posterior tooth-coloured crowns have been developed. These are usually veneered, although all-ceramic crowns such as zirconium are also available. Owing to the thickness of these aesthetic crowns, a more extensive tooth preparation is required. In primary teeth this is significant due to the enamel/dentine/pulp ratio. There is also an issue with the loss of the veneer over time, although these crowns are improving in quality with advancements in manufacturing techniques.
Conclusion
The use of PMCs has been shown to be a successful restorative option, accepted by patients and their carers. The technique of conventional PMC placement is, in the authors' opinion, relatively simple and certainly much simpler to carry out than intra-coronal restorations in primary teeth.
The second of these papers will discuss the Hall Technique, which does not involve tooth preparation. Some practitioners will have a preference for either the conventional or Hall technique. For those who adopt the latter, it is essential to understand the conventional technique for instances when the Hall Technique is not possible. These occasions include, amongst others, the presence of a ledge or significant space loss, preventing a crown from seating without preparation.