Witkop CJ, Gundlach KK, Streed WJ, Sauk JJ Globodontia in the otodental syndrome. Oral Surg Oral Med Oral Pathol. 1976; 41:(4)472-483
Bloch-Zupan A, Goodman JR. Otodental syndrome. Orphanet J Rare Dis. 2006; 1
Gregory-Evans CY, Moosajee M, Hodges MD SNP genome scanning localises oto-dental syndrome to chromosome 11q13 and microdeletions at this locus implicate FGF3 in dental and inner-ear disease and FADD in ocular coloboma. Hum Mol Genet. 2007; 16:(20)2482-2493
Sedano HO, Moreira LC, de Souza RA, Moleri AB. Otodental syndrome: a case report and genetic considerations. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:(3)312-317
Cook RA, Cox JR, Jorgenson RJ. Otodental dysplasia: a five year study. Ear Hear. 1981; 2:(2)90-94
Lee ML, Levin LS, Kopstein E. Autosomal recessive sensorineural hearing impairment, dizziness, and hypodontia. Arch Otolaryngol. 1978; 104:(5)292-293
Gorlin RJ, Cohen MM, Levin LS. Syndromes of the Head and Neck, 3rd edn. New York: Oxford University Press; 1990
Alsmald O, Meyer BF, Alkuraya F Syndromic congenital sensorineural deafness, microtia and microdontia resulting from a novel homoallelic mutation in fibroblast growth factor 3 (FGF3). Eur J Hum Genet. 2009; 17:(1)14-21
Stewart DJ, Kinirons MJ. Globodontia. A rarely reported dental anomaly. Br Dent J. 1982; 152:(8)287-288
Chen RJ, Chen HR, Lin LM, Lin CC, Jorgenson RJ. “Otodental” dysplasia. Oral Surg Oral Med Oral Pathol. 1988; 66:(3)353-358
Santos-Pinto L, Oviedo MP, Santos-Pinto A, Iost HI, Seale NS, Reddy AK. Otodental syndrome: three familial case reports. Pediatr Dent. 1998; 20:(3)208-211
Vieira H, Gregory-Evans K, Lim N, Brookes JL, Brueton LA, Gregory-Evans CY. First genomic localisation of oculo-oto-dental syndrome with linkage to chromosome 20q13.1. Invest Opthalmol Vis Sci. 2002; 43:(8)2540-2545
Gorlin RJ. Otodental syndrome, oculo-facio-cardio-dental (OFCD) syndrome, and lobodontia: dental disorders of interest to the pediatric radiologist. Pediatr Radiol. 1998; 28:(10)802-804
Globodontia in the otodental syndrome: a rare defect of tooth morphology occurring with hearing loss in an eight-year-old Sinead Enright A Karen Humphrys Gillian Rea Jacqueline A James Dental Update 2024 42:10, 707-709.
Authors
SineadEnright
BDentSci, MFDS RCSI, MPaedDent RCPSG
Salaried Dental Services, Bradford District Care Trust, Westbourne Green Community Health Centre, 50 Heaton Road, Bradford, BD8 8RA
Otodental syndrome is a hereditary disorder comprising globodontia and sensorineural hearing loss. Globodontia is characterized by distinctively bulbous, enlarged crowns of molar and primary canine teeth. Anomalies including taurodontism and hypodontia also occur. We report on the dental treatment and multidisciplinary management of an eight-year-old girl with this rare condition. Referral to Clinical Genetics and Oral Pathology was instrumental in establishing a diagnosis of otodental syndrome for this young patient and her mother, who had similar dental defects.
CPD/Clinical Relevance: To increase awareness among practitioners of this rare dental disorder and highlight the need for multidisciplinary management of such cases.
Article
Globodontia is a gross morphologic dental anomaly characterized by ‘globe’-shaped teeth.1 The condition affects the size, shape and number of teeth with the most distinctive feature being bulbous, enlarged crowns of primary canine, primary molar and permanent molar teeth. Taurodontism, hypodontia, delayed eruption, malocclusion and dysmorphic facial characteristics have also been noted. The features of globodontia are summarized in Table 1.
Globodontia is a pathognomonic feature of otodental syndrome,2,3 a disorder of ectodermal origin first described by Levin et al in 1975.4 Synonymous terms include otodental dysplasia, familial otodentodysplasia and globodontia-deafness syndrome. In this rare, autosomal dominant condition, globodontia occurs with hearing loss.5 Nine families with otodental syndrome have been documented in the literature, including one kindred in which ocular coloboma segregates with the disease (oculo-oto-dental syndrome).2 Single nucleotide polymorphism (SNP) genome scanning of three affected families localized otodental syndrome to chromosome 11q13.3 Haplotype analysis revealed overlapping hemizygous microdeletions and subsequently haploinsufficiency of FGF3 was implicated as the likely cause of otodental syndrome.
Hearing impairment in otodental syndrome is sensorineural in nature and most pronounced in the high frequency range.2,4,6 Hearing deficit appears to plateau by the fourth decade.6 The combination of hearing loss and dental anomalies is seen in over 200 genetic syndromes7 and the sensorineural type can occur with missing permanent anterior teeth8 or teeth with dens invaginatus and unusual crown shapes.9 A condition which may have a similar pathogenesis to otodental syndrome is sensorineural deafness, microtia and microdontia associated with a homozygous FGF3 mutation.10
Case report
An eight-year-old girl was referred to the School of Dentistry, Belfast regarding ‘enamel hypoplasia’. She had no complaints on presentation and was unconcerned about the appearance of her teeth, but she was anxious about dental extractions. Her medical and developmental history revealed that she was born at full term with a difficult birth and postnatal period and had a low birth weight. Hearing loss was detected in infancy and subsequently hearing aids were used. However, there was a language and comprehension delay related to the impairment. Illnesses in early childhood included recurrent ear infections, leading to adenoidectomy and vent placement, and chickenpox at four years of age. She had strabismus, for which she wore glasses. Family history indicated that her mother and great uncle had similar dental defects and the mother had a cholinesterase deficiency.
Examination revealed the following findings:
Extra-oral
Normal facial appearance and facial proportions;
Small haemangioma in the midline of the upper lip.
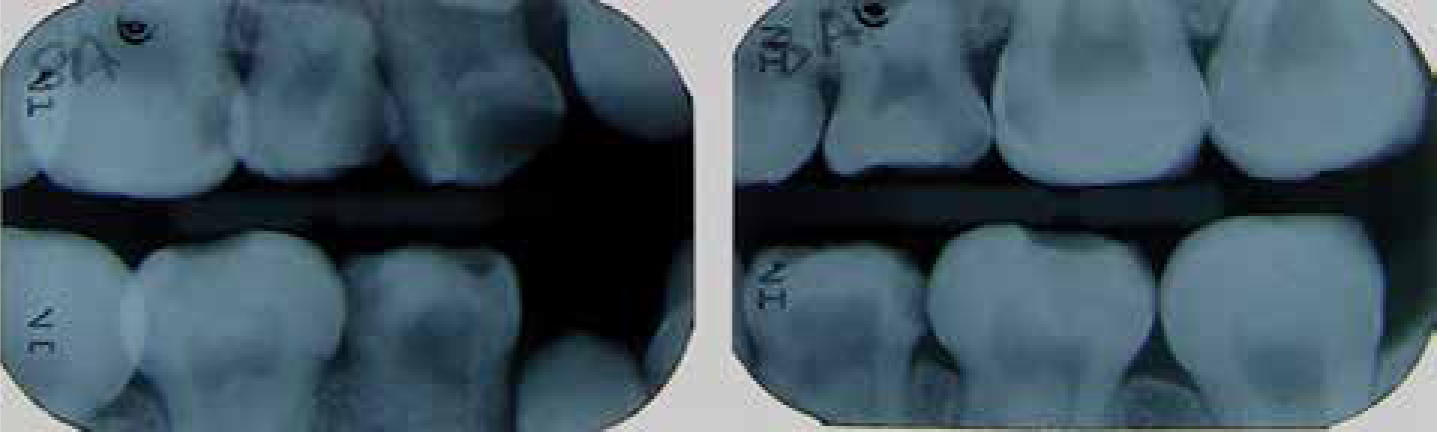
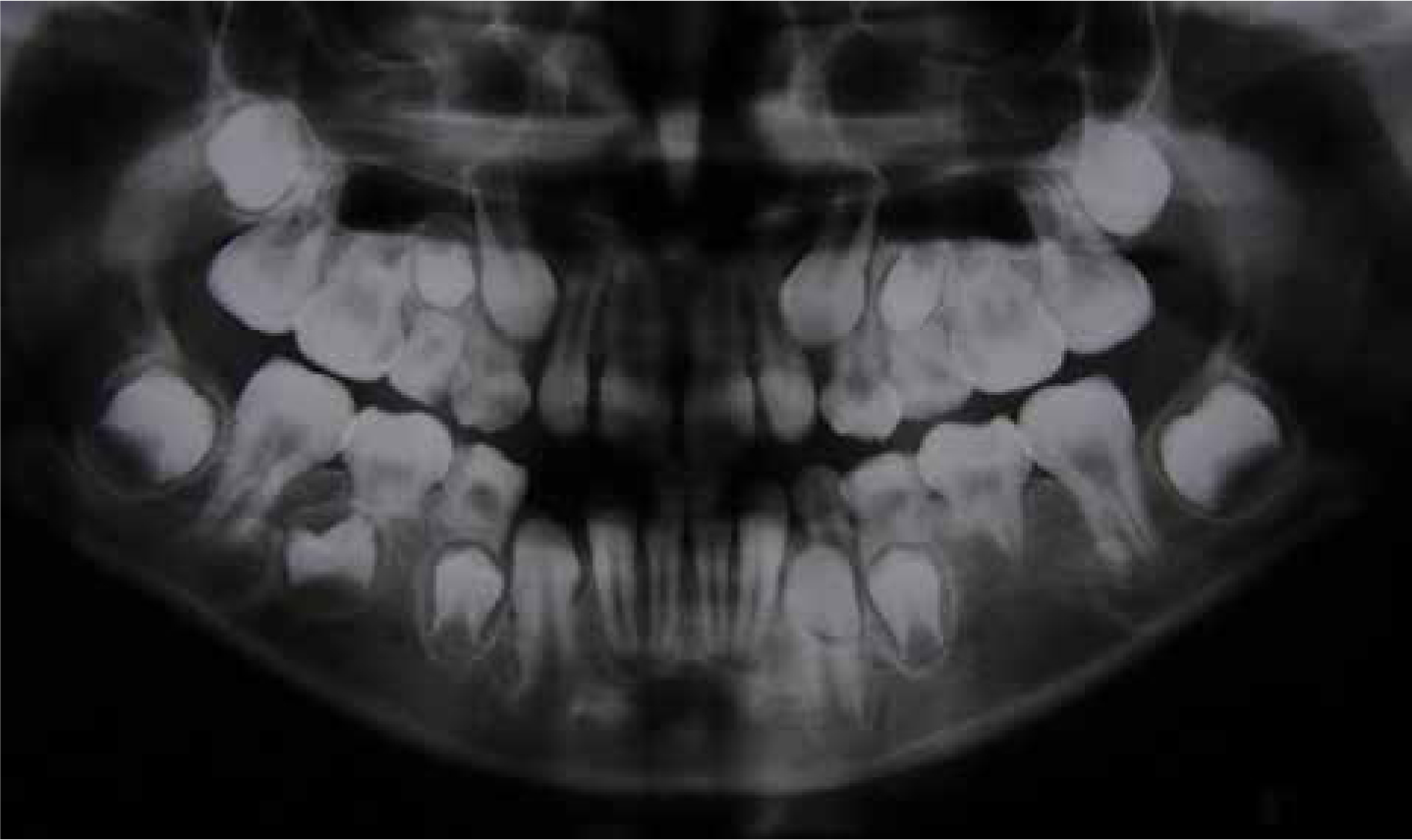
Figure 5. Bitewing radiographs showing malformed teeth with caries in primary molars and URC.Figure 6. Dental panoramic tomograph of child with otodental syndrome.
Single small eccentrically placed cusp on primary molar;
Abnormal root morphology;
Large pulp chamber;
Histologically normal structure of enamel and dentine.
Figure 7. Ground section of extracted primary tooth with globodontia.Figure 8. Extracted primary tooth with globodontia.
An orthodontic opinion was sought and extractions were recommended, including URE/ULE to allow mesial drift of UR6/UL6 and normalize the space required for prosthetic premolar teeth in the future.
Dental treatment included preventive dietary advice, oral hygiene instruction and topical fluoride application. Acclimatization, with consideration for age, dental anxiety and the need for clear communication with visual input was provided. Restorations were placed using a variety of plastic dental materials, such as resin-modified glass ionomer on ULC, hybrid and flowable composite on LRE/LLE, and an opaque but aesthetic composite to mask the enamel opacity in UR1 whilst minimizing the bulk of restorative material. As treatment progressed, the patient's plaque control improved and she was more relaxed and interested at her dental visits. However, general anaesthesia was required for extraction of URE, URD, URC/ULD, ULE; LRD/LLD.
A referral was made to clinical genetics and extracted teeth were sent to the oral pathology department. Through dental examination of the patient's mother and review of an article on her case,11 we could confirm that she had similar dental defects to those of the child.
Figure 9. Upper arch following extractions.Figure 10. Lower arch following extractions.Figure 11. Anterior teeth following treatment.
Diagnosis
Two of the extracted primary molar teeth were examined by oral pathology who established that our patient had globodontia. Assessment by a clinical geneticist confirmed the diagnosis of otodental syndrome in the patient and her mother.
Detailed ophthalmic examination of the patient (aged 10 years) and mother (aged 43 years) found that neither had evidence of colobomata or other ocular abnormalities. Audiology investigations at that stage confirmed the long-standing severe bilateral sensorineural hearing loss of the child. Audiology assessment of the mother revealed normal hearing thresholds bilaterally.
Discussion
This case highlights a rare autosomal dominant condition with characteristic dental dysmorphology, including globe-shaped posterior teeth, malformed roots and hypodontia. Although the majority of the literature on otodental syndrome indicates that incisor teeth and permanent canines are unaffected, microdontia of the lateral incisors11 and primary anterior teeth has been reported previously,12 leading us to believe that the unusual morphology of permanent incisor teeth in this patient is a result of the disorder. We also attribute the hypomineralized and deficient enamel on occlusal surfaces of lower second primary molars to the underlying developmental dental anomaly.
Variable expression (variation in the type and severity of clinical features between individuals with the same genetic alteration, even within the same family) and penetrance (proportion of individuals with a particular mutation who exhibit features of that disorder) are recognized in otodental syndrome.5 As the onset of hearing problems in the disorder varies4,6,13 and ocular defects in oculo-oto-dental syndrome may be mild,14 audiology and ophthalmology investigations were indicated for our patient and her mother. The findings in this case demonstrate variable expressivity and are reflective of other reports in which some individuals with otodental syndrome exhibited only dental anomalies or hearing impairment.1,2,4,5,6,11,12,13
Globodontia was recognized in the mother of the child we present almost 30 years ago in a paper written by Stewart and Kinirons.11 Although one author described that case report as being ‘doubtful’,15 a review of otodental syndrome in 2006 recognized that she did, indeed, have the condition.2 As a result of the recent referral to clinical genetics, a diagnosis of otodental syndrome has been made for her, and the family have finally become aware of the link between the dental and hearing problems.
Mutation analysis in our family is outstanding but the underlying molecular defect is suspected to be a deletion of FGF3, as reported in three other families with the condition.3 Genetic testing is currently only available on a research basis but this would allow earlier confirmation of diagnosis, particularly in those without a family history or those without all of the phenotypic features.
Conclusion
This case report informs dental practitioners about a rare developmental dental defect associated with hearing loss. It increases awareness of the need to take a detailed medical, dental and family history in patients with oral anomalies. The benefits of multidisciplinary management in cases of dental dysmorphology are demonstrated by the involvement of the dental, pathology and genetics teams in providing a concrete diagnosis of otodental syndrome for this patient and her mother. Referral of the young girl from her general dental practitioner to the paediatric department of the dental school facilitated joint treatment planning with consideration of her future orthodontic and restorative needs and provision of dental care in a child-centred manner.