Pecie R, Krejci I, Garcia-Godoy F, Bortolotto T. Non-carious cervical lesions – a clinical concept based on the literature review. Part 1. Prevention. Am J Dent. 2011; 254:49-56
Grippo JO. Abfractions: a new classification of hard tissue lesions of teeth. J Esthet Dent. 1991; 3:14-19
Lee WC, Eakle WS. Possible role of tensile stress in the etiology of cervical erosive lesions of teeth. J Prosthet Dent. 1984; 52:374-380
Lee HC, Lin CL, Wang CH, Cheng CH, Chang CH. Stresses at the cervical lesion of maxillary premolar. A finite element investigation. J Dent. 2002; 30:283-290
Rees JS. The biomechanics of abfractions. Proceedings of the Institution of Mechanical Engineers part H. J Engineering Med. 2006; 220:69-80
Burke FJT, Whitehead SA, McCaughey AD. Contemporary concepts in the pathogenesis of the Class V non-carious lesion. Dent Update. 1995; 22:28-32
Telles D, Pegorado LF, Periera JC. Incidence of noncarious cervical lesions and their relation to the presence of wear facets. J Esthet Restor Dent. 2006; 18:178-183
Silva AG, Martins CC, Zina LG, Moreira AN, Paiva SM, Pordeus IA, Magalhaes CS. The association between occlusal factors and noncarious cervical lesions: a systematic review. J Dent. 2013; 41:9-16
Estafan A, Furnari PC, Goldstein G, Hittelman EL. In vivo correlation of noncarious cervical lesions and occlusal wear. J Prosthet Dent. 2005; 93:221-226
Senna P, Del bel Cury A, Rosing C. Non-carious cervical lesions and occlusion: a systematic review of clinical studies. J Oral Rehabil. 2012; 39:450-462
Bartlett DW, Shah P. A critical review of non-carious cervical (wear) lesions and the role of abfraction, erosion and abrasion. J Dent Res. 2006; 85:306-312
Attar N, Tam LE, McComb D. Flow, strength, stiffness and radiopacity of flowable resin composites. J Can Dent Assoc. 2003; 69:516-521
Stewardson DA, Creanor S, Thornley P, Bigg T, Bromage C, Browne A, Cottam D, Dalby D, Gilmour J, Horton J, Roberts E, Westoby L, Burke T. The survival of class V restorations in general dental practice: part 3. five year survival. Br Dent J. 2012; 212
Heintze SD, Ruffieux C, Rousson V. Clinical performance of cervical restorations – a meta-analysis. Dent Mater. 2010; 26:993-1000
Chee B, Rickman LJ, Satterthwaite JD. Adhesive for the restoration of non-carious cervical lesions: a systematic review. J Dent. 2012; 40:443-452
Peumans M, De Munck J, Mine A, Van Meerbeck B. Clinical effectiveness of contemporary adhesives for the restoration of non-carious cervical lesions. A systematic review. Dent Mater. 2014; 30:2089-1303
Van Dijken JWV, Pallesen U. Long-term dentin retention of etch-and-rinse and self-etch adhesives and a resin-modified glass ionomer cement in non-carious cervical lesions. Dent Mater. 2008; 24:915-922
Van Dijken JWV. A prospective 8-year evaluation of a mild two-step self-etching adhesive and a heavily filled two-step etch- and-rinse system in non-carious cervical lesions. Dent Mater. 2010; 26:940-948
Van Dijken JWV, Sunnegardh-Gronberg K, Lindberg A. Clinical long-term retention of etch and rinse and self-etch adhesive systems in non-carious cervical lesions. A 13 years evaluation. Dent Mater. 2007; 23:1101-1107
Wilder AD, Swift EJ, Heymann HO, Ritter AV, Sturdevant JR, Bayne SC. A 12-year clinical evaluation of a three-step dentine adhesive in noncarious cervical lesions. J Am Dent Assoc. 2009; 140:526-536
Boghosian AA, Drummond JL, Lautenschlager E. Clinical evaluation of a dentin adhesive system: 13 year results. J Dent Res. 2007; 86:(Spec Issue)
Loguercio AD, Reis A, Barbosa AN, Roulet JF. Five year double blind randomized controlled clinical evaluation of a resin-modified glass ionomer and a polyacid-modified resin in non-carious cervical lesions. J Adhes Dent. 2003; 5:323-332
Franco EB, Benettti AR, Ishikiriama SK 5-year clinical performance of resin composite versus resin-modified glass ionomer restorative system in non-carious cervical lesions. Oper Dent. 2006; 31:403-408
Gwinnett AJ, Kanca J. Interfacial morphology of resin composite and shiny erosion layers. Am J Dent. 1992; 5:316-317
Tay FR, Pashley DH. Resin bonding to cervical sclerotic dentine: a review. J Dent. 2004; 32:173-179
Da Costa TEF, Loguercio AD, Reis A. Effect of enamel bevel on the clinical performance of resin composite restorations placed in non-carious cervical lesions. J Esthet Restor Dent. 2013; 25:346-356
Schroeder M, Reis A, Luque-Martinez I, Loguercio AD, Masterson D, Maia LC. Effect of enamel bevel on retention of cervical composite resin restorations: a systematic review and meta-analysis. J Dent. 2015; 43:777-788
Mickenautsch S. How well are current GIC product labels related to current systematic review evidence?. Dent Update. 2011; 38:634-644
Burke FJT. The evidence base for ‘own label’ resin-based dental restoratives. Dent Update. 2013; 40:5-6
A large number of Class V restorations are placed per annum to restore cervical lesions. This paper evaluates the pathogenesis of these lesions, with particular reference to the role of occlusal factors, and reviews the literature in order to provide advice on the material(s) which are most likely to produce optimal longevity of a Class V restoration.
CPD/Clinical Relevance: Resin-modified glass ionomer materials appear to provide optimal survival for a Class V restoration, but a (flowable) composite might produce a better aesthetic result.
Article
The Class V cavity constitutes a considerable burden of treatment for the general dental practitioner, with the most recent available figures in England and Wales indicating that more of these are placed than Class I restorations (circa 1.5million vs 1.4 million in the year 2004–2005),1 although these data do not differentiate between non-carious cervical lesions (NCCL) and restorations placed because of root caries. However, worldwide, the prevalence of NCCL has been estimated to vary from 5–85% of the population,2 while the review by Pecie and colleagues3 found a prevalence ranging from 11–62%. The prevalence and severity also appears to increase with age. Despite this prevalence, these restorations do not appear to attract the attention or imagination of dentists worldwide, given the substantial volume of publications on Class I and II composites and the relative paucity of papers on Class V restorations.
It is therefore the aim of this paper to review the literature on Class V restorations with particular respect to which material performs optimally in these cavities.
Pathogenesis of the Class V lesion
Class V cavities may form:
As a result of caries;
From attack by erosive substances; and/or
By excessive toothbrushing with a hard toothbrush (Figure 1).
Figure 1. Excessive toothbrushing with an abrasive paste was considered to be the cause of these Class V cavities in a patient from China.
Might occlusal factors be involved?
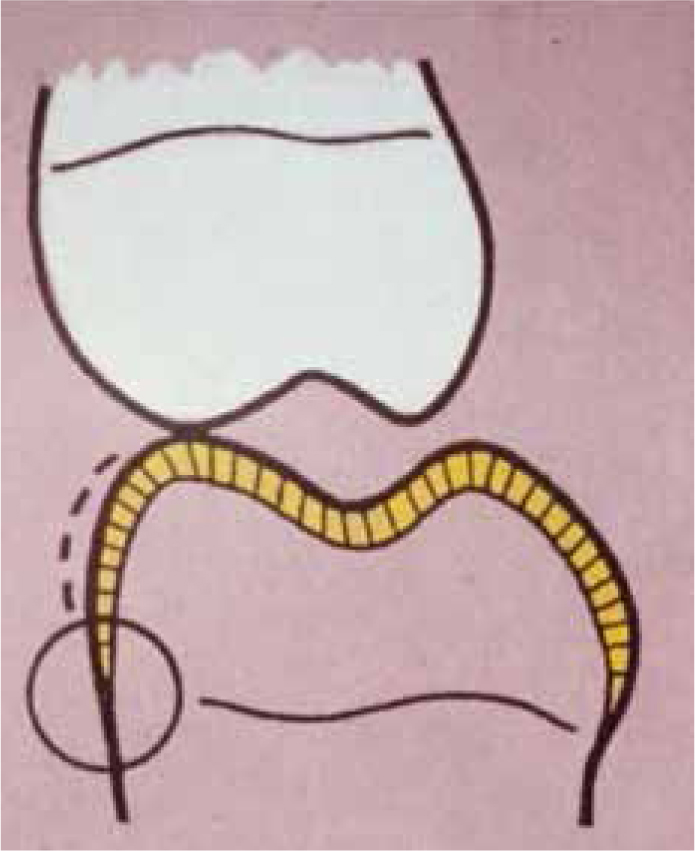
An occlusally related pathogenesis has been proposed, with Grippo4 terming these lesions ‘abfractions’ from the Latin words for ‘breaking away’, in an attempt to explain the development of wedge-shaped lesions (Figure 2). The concept of tensile stresses in the aetiology of NCCL was first put forward by Lee and Eakle in 1984,5 with the theory being extended by Grippo4 in 1991 to include the concept of chemical or electrochemical degradation in the cervical area of affected teeth. Some engineering studies have supported the ‘abfraction theory’ by way of tensile stresses resulting from oblique occlusal forces causing the commencement of a lesion by disruption of bonds between hydroxyapatite crystals in the cervical area of teeth where the enamel is thin.6,7 One paper,8 in 1995, presented an SEM image purporting to demonstrate the initiation of an abfraction lesion by a small enamel fracture. Telles and co-workers9 examined 1,131 teeth in first year dental students, finding 129 NCCL, with 29 of the 40 students having at least one tooth with one lesion. After three years, the incidence of new lesions was 57, with the identification of new lesions associated with the presence of wear facets being statistically significant.
Figure 2. Proposed pathogenesis of the abfraction lesion by initial fracture of enamel prisms in the cervical region of the tooth as a result of occlusal stress (after Lee and Eakle5).
However, support for the ‘abfraction theory’ is generally lacking in systematic reviews:
A recent systematic review by Silva and colleagues10 examined the association between NCCL and occlusal factors, with the results indicating that there was no support for an association between the two and the authors stating that ‘the evidence does not support intervention to alter some occlusal factors for the prevention or control of the progression of NCCL’. However, three of the nine studies eventually included in the review of the 1,082 potentially eligible studies found associations between NCCL and some variables, such as occlusal contact area, right canine guidance, premature contacts in centric relation and working side.
Estafan and co-workers,11 on examining the 299 casts of the teeth of dental students, clearly concluded that ‘non-carious cervical lesions are not related to occlusal wear’.
The result of the systematic review by Senna and colleagues12 concurs with this view, concluding that ‘the role of occlusion in the pathogenesis of non-carious cervical lesions seems undetermined’.
Finally, the critical review of NCCL by Bartlett and Shah13 concluded ‘that there is little evidence, apart from laboratory studies, to indicate that abfraction exists other than as a hypothetical component of cervical wear’. In addition, these authors state that ‘much stronger evidence suggests that cervical wear is a combination of erosion, abrasion and attrition’.
This view, of a multifactorial aetiology for NCCL, is supported by a variety of other authors.14,15,16
In summary, therefore, support for a relationship between occlusal wear and NCCL development may be considered insufficient, in the view of the author, to support preventive intervention/treatment of NCCL lesions by occlusal adjustment.
Reasons to treat a Class V lesion
Sensitivity, the presence of a carious lesion or poor aesthetics may result in a patient's request for treatment of a Class V lesion, but the dental practitioner may also consider restoration of such a lesion under the following circumstances:8
To arrest the progress of the lesion;
To prevent plaque accumulation and the potential onset of caries or periodontal disease;
Because it is unaesthetic;
Where pulpal exposure is likely if the lesion increases in depth;
Because it is interfering with a denture seating, or to improve denture clasp retention.
In addition, the American Academy of Operative Dentistry17 has suggested that, for lesions influenced by acidic dissolution, the reasons for the acid challenge should be assessed and the patient counselled, be it with regard to the consumption of fruit juice or other potentially erosive drinks (some sports drinks and herbal teas being implicated in some research). Furthermore, patients with conditions which result in gastric reflux should be counselled to seek medical attention. In other words, a first treatment goal should be the removal of the aetiological factors.17 It should also be noted that dentine is less resistant to acid attack and wear than enamel so that, when the dentine is exposed, the destruction of tooth substance will accelerate.
An alternative view has been proposed by Pecie and colleagues from the University of Geneva,3 namely that restoration should be postponed in the absence of aesthetic demands, sensitivity or a threat to the integrity of the tooth, given their consideration that the development of the NCCL is a slow process. They suggest preventive therapy, including risk assessment and prevention of development of NCCL by correcting habits and the early detection and management of incipient lesions. For patients presenting with NCCL, they suggest the use of a soft toothbrush and low abrasion fluoridated toothpaste and the avoidance of a toothpaste with a low pH. They also suggest the avoidance of toothbrushing after an acidic challenge and the use of adhesive systems to provide a dentine seal to be an effective strategy.
Properties of materials for Class V restorations
A number of restorative materials may be used for the restoration of Class V carious cavities or non-carious lesions. Fifty years ago, gold inlays were favoured for these cavities, formed by the taking of a wax pattern of the cavity, the investment of the pattern and the forming of the inlay by the lost wax process in a one visit technique (in the way that CAD CAM techniques can do today!). However, these restorations were not aesthetic in everyone's eyes! (Figure 3).
Figure 3. Gold inlays were once a means of restoring Class V cavities. They were also once considered aesthetic!
Today, with the advent of materials such as glass ionomer and its variants, which reliably adhere to tooth substance, the placement of Class V restorations is substantially simplified. Resin composite and its variants, such as flowable composites, are also appropriate, when used in conjunction with a dentine-bonding agent. The use of amalgam in Class V appears to be waning, but there are no data available which indicate the respective numbers of restorations placed in these materials.
Ideal properties of a material for restoration of Class V cavities
Material specific properties for Class V restorations include:
Satisfactory resistance to wear caused by toothbrushing;
Low modulus of elasticity, given that anterior teeth have been considered to flex around their cervical area;
Good aesthetics.
Other properties, although not specific to Class V restorations, which could be considered appropriate include:
Small filler particles for polishability;
Sufficiently stiff consistency to hold shape, yet easily placed into a cavity (although some operators appear to prefer the consistency of a flowable composite);
Self curing/setting or curable to any depth;
Dimensionally stable or low shrinkage/stress;
Fluoride release;
Self-adhesive to enamel and dentine.
Amalgam
Amalgam may be used for Class V restoration, but its use is limited by the fact that it requires the provision of undercuts into the cavity, if these are not present as a result of caries removal, ie it is unlikely to fulfil the ideals of minimally invasive dentistry. It is also unaesthetic.
Glass ionomer
Glass ionomer (GI) and its variants possess the ideal property of adhesion to tooth substance by way of the chemical reaction between the polyacrylic acid constituent of the material and the calcium of the hard dental tissues.18 All glass ionomer materials release fluoride as a result of their acid-base setting reaction but, while this may be considered to be a beneficial property, this fluoride release has little or no effect on cariostasis in vivo.19 Conventional glass ionomers tend to be opaque and thereby unaesthetic (Figure 4), but have the low modulus considered appropriate for restoration of cavities in the cervical region. Resin-modified GIs (RMGIs) were developed by the incorporation of a resin into the glass ionomer matrix: this decreases the solubility of the material, improves its adherence to tooth tissue, improves its fluoride release and results in a material which is more aesthetic and which can be finished and polished immediately following placement, providing potentially reasonable aesthetics (Figure 5).18 For these reasons, RMGIs are therefore the glass ionomer of choice for the restoration of Class V cavities and non-carious cervical lesions.
Figure 4. Class V conventional glass ionomer restoration immediately after placement, the restoration being opaque and of less than ideal aesthetics.Figure 5.
(a) Cervical cavity adjacent to crown at UL3, requiring restoration. (b) Cavity in Figure 5a restored with RMGI.
Resin composite
Resin composite materials, other than those developed for use as self-adhesive resin luting materials,20 do not have any innate bond to tooth structure, so an intermediate dentine/enamel bonding agent must be employed. These are the most aesthetic materials available for use in Class V restorations (Figure 6). Several variants are available, with the less heavily-filled flowable variants being particularly favoured in Class V cavities. Initially, these materials were considered to have a modulus of elasticity close to dentine, but it is now apparent that their modulus is simply closer to that of tooth structure, as opposed to close.21
Figure 6.
(a) Abrasion/erosion cavities in the maxillary central incisor teeth of a patient with toothwear. The incisal edges of the upper anterior teeth have already been restored using a nano-filled composite. (b) Resin composite may be considered to be the material of choice for Class V cavities when aesthetics is the over-riding consideration. Cavities in Figure 6a restored with flowable composite, immediately after placement and finishing.
Flowable composites, which were introduced in 1995, are less heavily filled (45–60%) variants of conventional hybrid resin composite materials. Early materials had low viscosity, high polymerization shrinkage, low wear resistance, but, today, companies have added other components (resins, different filler types and amounts) in an effort to reduce polymerization shrinkage. These materials, which are often available in a wide variety of shades, are presented in syringe format, so are designed to flow into crevices or line angles without creating air voids. The material spreads or flows rather than staying in one place or shape, being ‘puddled’ into position. In this regard, a recently introduced composite, Sonic Fil (Kerr Mfg Co, Orange, CA, USA) may be of value in the restoration of Class V cavities. This uses sonic energy via a specially designed handpiece, in order to reduce the viscosity of the composite when it is being applied to the cavity, with the material becoming more viscous when the sonic energy is stopped.
With flowable composites, there is a delicate balance between polymerization shrinkage and modulus of elasticity. Being less heavily filled, it would be expected that their shrinkage will be greater than more heavily filled conventional composite materials. However, being less heavily filled, flowable composites will have a lower modulus of elasticity, ie increased flexibility, which could be perceived as an advantage, given that teeth are considered to flex, with the cervical region being the fulcrum.
Survival of Class V restorations
The literature was reviewed, by way of a Medline search, in order to determine the optimum material(s) for restoring Class V lesions. Papers included were:
Systematic reviews and meta analyses;
Papers giving details of survival of Class V restorations over 10 years; or
Where large numbers of restorations (> 500) were involved.
Furthermore, it was considered that papers from the ‘real world’ of general dental practice were ideal, given that this is where the majority of treatment, worldwide, is carried out. However, only one paper from this arena was identified, that from Stewardson et al22 (vide infra). The studies identified in the Medline search are summarized below:
Heintze and co-workers23 carried out a literature review and meta-analysis which was published in 2010. Fifty clinical studies involving 40 adhesive systems matched their inclusion criteria. These workers found that, on average, 10% of cervical restorations were lost and 24% exhibited marginal discoloration after three years. However, the variability ranged from 0–50% for retention loss and from 0–74% for marginal discoloration. They detected ‘hardly any’ secondary caries. The results indicated that the adhesive/restorative class had the most significant influence, with 2-step self-etching adhesive systems performing best (an example being Clearfil SE [Kuraray]) and 1-step self-etch adhesive systems performing worst (an example being One Step [Bisco]). Three-step etch and rinse systems, glass ionomers/resin-modified glass ionomers, 2-step etch and rinse systems were ranked in between. These authors also concluded that the dentine and enamel surface should be roughened before placement of the restoration, but that bevelling of the enamel margin did not influence the clinical result.
Chee and colleagues24 carried out a systematic review of the restoration of NCCL, published in 2012, including randomized controlled trials (RCTs), comparing at least two adhesives in NCCLs with >18 months’ follow-up. They concluded that there was wide variation between adhesives in the same category, but added, somewhat disappointingly, that there was insufficient evidence to support one adhesive system or bonding strategy over another.
Peumans and colleagues25 published, in 2014, a systematic review on the clinical effectiveness of adhesives for the restoration of NCCLs, reviewing Medline, Ovid and IADR abstracts. They included RCTs that included at least two adhesives with a follow-up period of >18 months, calculating annual failure rates (AFRs). Their results indicated the lowest mean AFR scores for glass ionomer, followed by two-step self-etch adhesives, three-step etch and rinse systems, while significantly higher AFR scores were recorded for one-step self-etch systems, two-step etch and rinse systems and two-step self-etch systems. They also noted significant differences between adhesives of the same class and that selective enamel etching did not influence the retention rate of self-etch adhesives.
Van Dijken and Pallesen26 reported the results of etch and rinse and self-etch adhesives and a resin-modified glass ionomer at 13 years. Initially, 270 restorations were placed, with 215 being evaluated at 13 years. Fifty-three per cent of restorations were lost over that period, with significantly different failure rates for the different systems. The AFRs were as follows:
Etch and rinse systems
- Syntac Classic (Ivoclar, Lichtenstein) 2.8%
- Optibond (Kerr Mfg Co, Orange, CA, USA) 3.1%
- Permagen (Ultradent, Utah, USA) 13%
- Scotchbond MP (3M ESPE, MN, USA) 4.8%
Self-etch systems
- PSA (Dentsply, Konstanz, Germany) 4.4%
- RMGI, Vitremer (3M ESPE, MN, USA) 2.7%
As reported in other studies, there was wide variation within the same generic type of adhesives, with 78% of Permagen-retained restorations being lost over 13 years, compared with 41% of Optibond-retained restorations. This compared with a loss of 36% of Vitremer RMGI restorations after 13 years.
Van Dijken27 further reported on two adhesive systems (Clearfil SE and PQ1) at 8 years. One ‘experienced operator’ placed 119 restorations at baseline, recalling 112 at 8 years – an excellent recall rate. The cumulative loss rate at 8 years was 26% for Clearfil SE and 39% for PQ1, a significant difference. Furthermore, he did not note any difference between the lesions with sclerotic and non-sclerotic dentine, although the results confirmed better clinical retention in the slightly roughened lesions and higher loss rate in the ‘severe-sclerotic’ lesions. The size of the lesions did not influence bonding effectiveness.
Van Dijken and colleagues 28 have reported a 13-year evaluation of four etch and rinse and three self etch adhesive systems in NCCL, assessing a total of 275 restorations during the observation period. The cumulative loss rate at 13 years was 60%, with significant differences in failure rates for different systems, these varying between 26% and 95%. Clearfil Liner Bond, with an AFR of 2.0% performed best, while Denthesive (Heraeus-Kulzer, Wehrheim, Germany) performed worst with an AFR of 7.3%. No recurrent caries was observed. The authors commented that all systems showed a degradation of the bond.
Wilder and colleagues29 reported, in 2009, on a 12-year clinical evaluation of a three-step etch and rinse adhesive (Optibond Dual-Cure: Kerr) in NCCLs. They restored 100 NCCLs, the results indicating a 93% retention in a group in which the enamel was etched, while in the group where both enamel and dentine were etched, the retention rate was 84%. The authors considered this retention rate to be unmatched in clinical research studies of this type, especially in light of the clinical variables encountered in the study. However, van Dijken and Pallesen26 presented a retention rate of the same bonding system of 60% at 13 years, while Boghosian and colleagues30 found the retention rate of Optibond Dual cure to be 97% at 13 years.
Lastly, from the world of UK general dental practice, Stewardson and colleagues22 have reported the five year survival of Class V restorations at five years. Ten general dental practitioners, from the Birmingham-based practice-based research group BRIDGE, collected an extensive amount of data on each occasion that they placed a Class V restoration, with the choice of material being the practitioners' own decision and with the data then being subjected to statistical analysis using Kaplan-Meier analysis and Cox Regression to test for significant associations between factors such as the practitioner, the patient's age and oral hygiene, method of payment, the tooth, the cavity and the type of restorative material used. At the end of five years, 989 restorations were available for analysis, with a total of 27.8% of restorations having failed and 11.7% being lost to follow-up. Complete loss of the restoration was the predominant mode of failure, comprising 83% of the failures. Increasing age of patient was associated with a shorter time to restoration failure, while other factors involved were:
- Use of a rotary instrument to roughen the dentine surface or provide an undercut was associated with a 40% reduction in risk of failure;
- Moisture contamination resulted in a 29% increase in risk of failure;
- Large cavities increased the risk of failure by 165% compared to small;
- Cavities only in dentine had an increased risk of failure by 39%.
The five-year survival of the different materials is presented in Table 1.
RMGI
79%
Amalgam
75%
Flowable Composite
69%
Composite
68%
Compomer
71%
Conventional Glass Ionomer
51%
When interpreting these results, all materials were associated with a longer time to restoration failure than conventional glass ionomer, with RMGI performing optimally. There was also a significant relationship between whether the Class V cavity was carious or non-carious, with the follow-up comparisons indicating that more of the carious cavities had been filled with amalgam or RMGI or other materials. When the data were further separated, the time to failure of GI restorations was shorter than for other materials, with the log-rank tests indicating that this was only significant for carious cavities, and not for non-carious. There was no association with regard to carious cavities being prepared with a bur, but only 18 were so treated. However, with non-carious cavities, the time to failure for restorations in which the cavity was not prepared with a bur was significantly reduced compared with those which had been prepared. The results of this particular study concur with others of similar duration by Loguercio and co-workers31 and Franco et al,32 both of which demonstrated superior performance of RMGI (when compared with other tooth-coloured restorative materials) in NCCL.
Finally, with regard to the role of occlusal factors in the aetiology and restoration of NCCLs, the study by Stewardson et al22 did not identify an influence of any occlusal factors on time to restoration failure.
Discussion
This paper evaluated the survival rate of a variety of materials used to restore Class V carious and non-carious cavities. The lack of homogeneity among the papers included in the present work makes drawing conclusions difficult, in particular because of the variety of criteria used to place or replace Class V cavities. However, it could be argued that this is what clinical dental practice is all about, with practitioners from differing undergraduate and postgraduate backgrounds providing a wealth of data.
The information presented here may therefore be considered to be robust, with a number of common themes emerging, namely, that RMGI materials provide the best AFRs in a number of studies and reviews and could therefore be recommended as the material of choice, other than in situations where the superior aesthetics of resin composite (flowable or other) is indicated.
Should the surface of the cavity be roughened?
There is evidence from the study by Heintze et al23 that this is a good clinical practice, with the study by Stewardson and colleagues22 supporting this. Van Dijken27 has discussed this, considering that, in contrast to the creation of a smear layer during cavity preparation, the cervical lesion is not normally covered by a smear layer, and that roughening with a round diamond prior to the adhesive restoration will create a smear layer similar to that found in drilled cavities. In his 8-year study,27 there was better clinical retention in the slightly roughened cavities. In addition, the removal of the outer surface of sclerotic dentine by roughening with a diamond has been suggested in order to create a hybrid layer similar to young dentine.33 While removal of a hyper-mineralized sclerotic dentine surface using phosphoric or stronger acids has been discussed, this may be considered to have the potential to result in post-operative sensitivity. Accordingly, removal of the surface layer of sclerotic dentine has also been recommended by Tay and Pashley,34 since clinicians have no way of discerning the actual morphology of the NCCL surface. Finally, the review by Heintze et al23 provides additional information regarding the benefit of roughening the dentine surface, given that they identified that retention and marginal discoloration was significantly less in those restorations whose surface was prepared with a diamond but prior to placement of the adhesive.
Should the margin of the NCCL be bevelled?
The perceived wisdom, in the past, was that it should, insofar that this would increase the surface area of contact between restorative and tooth. However, the review by Heintze et al23 did not identify any clinical improvement when the coronal enamel was bevelled. This is confirmed by the work of Da Costa and colleagues35 and a very recent systematic review/meta-analysis by Schroeder et al.36
Which dentine adhesive provides optimum retention for resin composite restorations in NCCLs?
The review by Heintze et al23 identified the 2-step self-etching adhesive systems as performing better than the 3-step etch and rinse systems, followed by the glass ionomer cements and RMGIs, with the worst performance in the 1-step self-etching group. In their 13 year evaluation, Van Dijken and Pallesen26 commented that all the systems that they tested showed a continuous degradation of bond, but with an RMGI performing optimally and a 3-bottle dentine bonding system (Optibond) performing best in that group of materials while, in a separate study, Van Dijken and collagues28 identified Clearfil Liner Bond as performing optimally. In the systematic review by Peumans and colleagues,25 their results indicated the lowest mean AFR scores for glass ionomer, followed by two-step self-etch adhesives, three-step etch and rinse systems, and significantly higher AFR scores were recorded for one-step self-etch systems.
The heterogeneity of the data makes it difficult to present one resin-based bonding agent as being superior in a variety of studies, with Chee et al24 identifying variation among adhesives with the same bonding strategy – is this due to variations in composition and/or manufacturer, perhaps? However, it appears that 2-step self-etching adhesive systems, such as Clearfil SE, have been found to perform optimally, followed by the 3-step etch and rinse materials, with the variants of Clearfil (Clearfil SE and Clearfil LinerBond) being mentioned as performing well in several studies, as well as the 3-bottle versions of Optibond. However, the field of dentine bonding is fast moving, with the latest variants, the Universal Bonding agents, appearing to hold promise. However, it might not be a coincidence that many of these new materials contain the monomer 10-MDP, which is a constituent of the Clearfil group of bonding agents.
Finally, placement of Class V restorations may be facilitated when less viscous materials, such as flowable composites, are replaced by the use of specially designed matrices, an example of which is illustrated in Figure 7. Furthermore, in order to maximize the effectiveness of restorations, as well as choosing the right generic type, as this article has attempted to elucidate, clinicians should use materials which have a good research pedigree, something which so-called ‘own label’ materials do not have.37,38
Figure 7. Kerr Hawe Class V matrices can be useful. The handle is autoclavable, the matrices disposable.
Conclusions
Which material and clinical technique performs best? From this review, it may be concluded that:
RMGI performs optimally and is therefore recommended in clinical situations in which aesthetics is not an overriding factor;
The surface of a NCCL should be roughened prior to placement of the restoration, be it GI-based or resin-based;
There is no need to bevel the coronal aspect of the cavity margin; and
2-step self-etch bonding agents, Clearfil SE being an example, appear to perform optimally, 3-step etch and rinse bonding agents also being well ranked in a number of studies, but with the bond reducing with time.