Thiruvenkatachari B Orthodontic treatment for prominent upper front teeth (Class II malocclusion) in children. Cochrane Database Syst Revs. 2013; 11
Hunt NP. Why should the NHS continue to fund orthodontic treatment in the current financial climate?. Royal College of Surgeons of England: Faculty Dental Journal. 2013; 4:16-19
Nguyen QV A systematic review of the relationship between overjet size and traumatic dental injuries. Eur J Orthod. 1999; 21:503-515
Johal A, Cheung MY, Marcene W. The impact of two different malocclusion traits on quality of life. Br Dent J. 2007; 202
Rusanen J Quality of life in patients with severe malocclusion before treatment. Eur J Orthod. 2010; 32:43-48
de Oliveira CM, Sheiham A. Orthodontic treatment and its impact on oral health-related quality of life in Brazilian adolescents. J Orthod. 2004; 31:20-27
Kenealy P The psychological benefit of orthodontic treatment. Its relevance to dental health education. NY State Dent J. 1991; 57:32-34
Shaw WC, Addy M, Ray C. Dental and social effects of malocclusion and effectiveness of orthodontic treatment: a review. Community Dent Oral Epidemiol. 1980; 8:36-45
Seehra J, Newton JT, Dibiase AT. Interceptive orthodontic treatment in bullied adolescents and its impact on self-esteem and oral-health-related quality of life. Eur J Orthod. 2013; 35:(5)615-621
Proffit WR, Tulloch JF. Preadolescent Class II problems: treat now or wait?. Am J Orthod Dentofacial Orthop. 2002; 121:560-562
O'Brien K Early treatment for Class II Division 1 malocclusion with the Twin-block appliance: a multi-center, randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2009; 135:573-579
Tulloch JF, Proffit WR, Phillips C. Outcomes in a 2-phase randomized clinical trial of early Class II treatment. Am J Orthod Dentofacial Orthop. 2004; 125:657-667
Wortham JR Comparison of arch dimension changes in 1-phase vs 2-phase treatment of Class II malocclusion. Am J Orthod Dentofacial Orthop. 2009; 136:65-74
O'Brien K Effectiveness of early orthodontic treatment with the Twin-block appliance: a multicenter, randomized, controlled trial. Part 1: Dental and skeletal effects. Am J Orthod Dentofacial Orthop. 2003; 124:234-243
McDowall RJ, Waring DT. Class II growth modification: evidence of absence or absence of evidence. Orthod Update. 2010; 3:44-50
Morris DO, Illing HM, Lee RT. A prospective evaluation of Bass, Bionator and Twin Block appliances. Part II − The soft tissues. Eur J Orthod. 1998; 20:663-684
Tumer N, Gultan AS. Comparison of the effects of monoblock and twin-block appliances on the skeletal and dentoalveolar structures. Am J Orthod Dentofacial Orthop. 1999; 116:460-468
O'Brien K Effectiveness of treatment for Class II malocclusion with the Herbst or twin-block appliances: a randomized, controlled trial. Am J Orthod Dentofacial Orthop. 2003; 124:128-137
Lee RT, Kyi CS, Mack GJ. A controlled clinical trial of the effects of the Twin Block and Dynamax appliances on the hard and soft tissues. Eur J Orthod. 2007; 29:272-282
Thiruvenkatachari B Comparison of Twin-block and Dynamax appliances for the treatment of Class II malocclusion in adolescents: a randomized controlled trial. Am J Orthod Dentofacial Orthop. 2010; 138:144 e1-e9
Nelson C, Harkness M, Herbison P. Mandibular changes during functional appliance treatment. Am J Orthod Dentofacial Orthop. 1993; 104:153-161
Courtney M, Harkness M, Herbison P. Maxillary and cranial base changes during treatment with functional appliances. Am J Orthod Dentofacial Orthop. 1996; 109:616-624
Ghafari J Headgear versus function regulator in the early treatment of Class II, division 1 malocclusion: a randomized clinical trial. Am J Orthod Dentofacial Orthop. 1998; 113:51-61
Keeling SD Anteroposterior skeletal and dental changes after early Class II treatment with bionators and headgear. Am J Orthod Dentofacial Orthop. 1998; 113:40-50
Baccetti T, Franchi L, Stahl F. Comparison of 2 comprehensive Class II treatment protocols including the bonded Herbst and headgear appliances: a double-blind study of consecutively treated patients at puberty. Am J Orthod Dentofacial Orthop. 2009; 135:698-699
Nelson B, Hansen K, Hagg U. Class II correction in patients treated with class II elastics and with fixed functional appliances: a comparative study. Am J Orthod Dentofacial Orthop. 2000; 118:142-149
Nelson B A long-term follow-up study of Class II malocclusion correction after treatment with Class II elastics or fixed functional appliances. Am J Orthod Dentofacial Orthop. 2007; 132:499-503
Emami MS, Jamilian A, Showkatbakhsh A. The effect of anterior inclined plane treatment on the dentoskeletal of Class II division 1 patients. J Indian Soc Pedod Prev Dent. 2007; 25:130-132
Class II division 1: an evidence-based review of management and treatment timing in the growing patient Sophy K Barber Katherine E Forde Richard J Spencer Dental Update 2024 42:7, 707-709.
Authors
Sophy KBarber
BDS, MJDF, MSc, MOrth RCS(Ed)
Post-CST Registrar in Orthodontics, Leeds Dental Institute
Class II division 1 malocclusion is common and various methods have been suggested for successful treatment in the growing patient. A number of recent high-quality studies have been undertaken to assess the efficacy of these treatments. We aim to outline the existing best evidence that supports current practice, with a review of the effect of treatment timing on outcome. This will provide a sound evidence-base for General Dental Practitioners for assessing, advising and referring young patients for treatment.
CPD/Clinical Relevance: General Dental Practitioners should understand the management options and optimal time for treating growing patients with a Class II division 1 malocclusion.
Article
Class II division 1 is an incisal classification of malocclusion where the incisal edge of the mandibular incisors lie posterior to the cingulum plateau of the maxillary incisors with normal or proclined maxillary incisors (British Standards Index, 1983). There is always an associated increase in overjet (Figure 1). This malocclusion is common, with an estimated prevalence of 15–20%,1 although there is racial variation, with Class II division 1 more common in Caucasian than Latin American, Middle Eastern and Asian populations, and lowest in Black racial groups.2
Figure 1. Class II division 1 incisal relationship with an increased overjet.
A number of genetic and environmental factors may contribute to a Class II division 1 malocclusion:
Skeletal factors – it is generally agreed that the majority of patients with a Class II malocclusion have some degree of skeletal imbalance with either a retrognathic mandible, protrusive maxilla or, most commonly, a combination (Figure 2);
Figure 2. Class II skeletal profile with retrognathic mandible.
Why treat Class II division 1?
A number of benefits have been associated with orthodontic treatment including a reduction in the susceptibility to caries, periodontal disease and temporomandibular joint dysfunction, whilst also improving speech and masticatory function. However, the supporting evidence is equivocal.3,4 It may be assumed that correction of an increased overjet will potentially reduce the risk of trauma, as it has been shown that individuals with an overjet greater than 3mm are twice as likely to suffer injury to their upper incisors.5 The meta-analysis undertaken in a recent Cochrane review found that ‘early orthodontic treatment for children with prominent upper front teeth is more effective in reducing the incidence of incisal trauma than providing one course of orthodontic treatment when the child is in early adolescence’.2
A number of studies have found that the presence of malocclusion can have a significant impact on an individual's quality of life6,7,8 and result in reduced self-esteem.9,10 Prominent upper incisors may be a target for teasing and bullying and it is now accepted that one reason for undertaking treatment of malocclusion is the psychosocial benefit that it accrues.3,4,11
What methods are there for the treatment of Class II division 1 malocclusion?
Clinical and radiographic examination of intra- and extra-oral hard and soft tissues is essential to establish the correct diagnosis and determine the likely aetiology of the malocclusion. Any habits must be completely stopped before treatment can be undertaken otherwise treatment is likely to be unsuccessful or relapse after completion.12
A number of methods have been advocated for the treatment of Class II division 1 malocclusion and these are dependent on patient age, the underlying aetiology, skeletal pattern and clinician preference. So-called ‘growth modification’ aims to alter growth pattern towards normal in growing patients with an underlying skeletal discrepancy; methods include functional appliance treatment and headgear. If growth modification is not required, orthodontic camouflage may be considered, including fixed appliances alone or in combination with extractions, intermaxillary elastics or temporary anchorage devices (TADs).
For non-growing patients with significant skeletal discrepancy in antero-posterior, vertical or lateral planes of space, and for those who are outside the realms of orthodontic camouflage, a combined surgical-orthodontic approach may be required. This will not be discussed further within this article as we wish to focus on growing patients.
Timing of treatment
Early treatment is defined as treatment provided in the early mixed dentition, usually between the ages of 7–9 years. This has also been called two-phase treatment, whereby a second separate definitive phase of treatment is undertaken when the patient reaches the permanent dentition. Late treatment, or one-phase treatment, is a single course of comprehensive treatment undertaken in the permanent dentition around the age of 12–14 years. Early treatment has been advocated to reduce the risk of incisal trauma, improve psychosocial well-being and reduce bullying (Table 1). It has also been claimed that early treatment can lead to superior outcomes in terms of efficiency, making definitive treatment easier, and efficacy, in that the final result is superior.13 Further assertions have been made for early treatment in terms of improved skeletal pattern, and reduced need for extractions and orthognathic surgery; however, these have been disproved in recent high quality clinical trials.14,15,16
Advantages of Early Treatment
Disadvantages of Early Treatment
Reduce the risk of incisal trauma
Risk of relapse due to failure to retain result and lack of lip competency
Risk of retreatment
Reduce teasing and bullying
Increased overall treatment time
Reduced final occlusal score
Risk of root resorption if maxillary canines not yet erupted
No evidence of long-term psychosocial benefit
One high-quality randomized controlled trial compared early and late treatment of Class II division 1 malocclusion with functional appliances.14 Although differences were found between treated patients and untreated controls after the initial phase, following a second phase of treatment there was no lasting difference in terms of skeletal pattern, extraction pattern or self-esteem. Detrimental effects were seen in those who had undergone early treatment; more appointments, longer total treatment time and associated costs, and a worse final occlusal outcome as indicated by the Peer Assessment Rating (PAR).
Similarly, trials involving early treatment with headgear have found that any early benefit gained in skeletal pattern and occlusion is lost following the second phase of treatment.15,16 Furthermore, Tulloch et al15 found no relationship between skeletal maturity and skeletal response to functional treatment, challenging the suggestion that correlating growth modification treatment to pubertal growth will improve outcome.
The availability of sufficient results from high-quality trials comparing early and late treatment facilitated meta-analysis to be undertaken as part of a Cochrane review.2 Combined findings showed that, at the end of all treatment, no significant differences were found in overjet, skeletal relationship or PAR score between the children who had a course of early treatment, with either headgear or functional appliances, and those who had not received early treatment. The only outcome to be affected by treatment timing was the incidence of new incisal trauma, which was significantly reduced by early treatment with either functional appliance or headgear (odds ratio 0.59 and 0.47, respectively). The Cochrane review concludes ‘the evidence suggests that providing early orthodontic treatment for children with prominent upper front teeth is more effective in reducing the incidence of incisal trauma than providing one course in early adolescence. There appears to be no other advantage for providing early treatment’.
Functional appliances
Functional appliances are a range of fixed and removable appliances that cause their effect by influencing the muscle groups that control position and function of the mandible, transmitting forces to the dentition and basal bone.12 The result is a decrease in overjet and correction of the buccal segment relationship, caused by both skeletal and dental changes. A recent study quantified the changes seen after a first stage of functional treatment.17 Skeletal change was attributed to restraint of maxillary forward and downward growth and increased growth and forwarding positioning of the mandible, contributing to 27% of the overjet reduction and 41% of buccal segment correction. Dental changes included retroclination of maxillary incisors, proclination of mandibular incisors and mesial eruption of mandibular molars. The majority of overjet reduction and buccal segment correction is dental, 73% and 59%, respectively. Soft tissue changes include elimination of lip trap and improved lip competence. It has also been postulated that tongue activity and soft tissue pressures from the lips and cheeks might be altered, enhancing the soft tissue environment.18
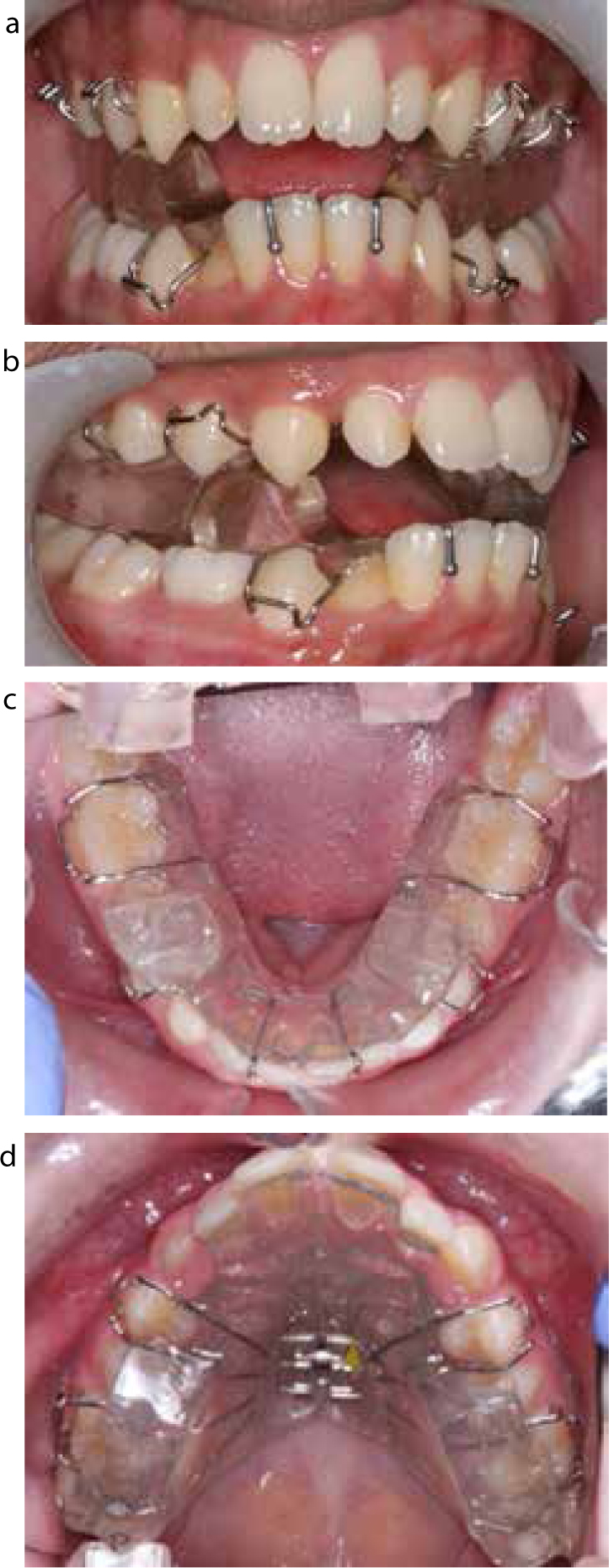
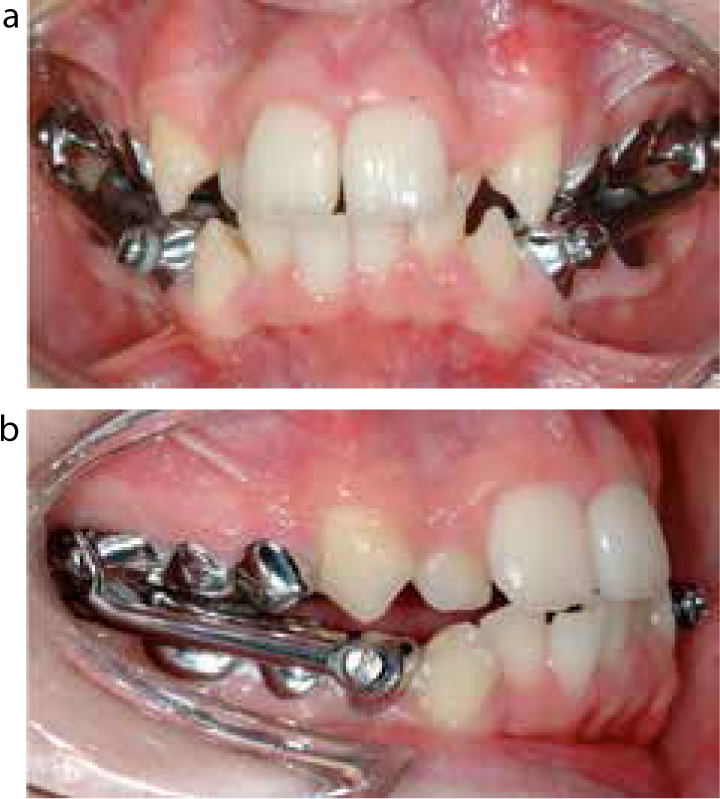
The first reported use of a mandibular positioning device was the ‘Monobloc’ by Dr Robin, in France in 1902, for neonates with under-developed mandibles. This was followed by the first functional device for growth modification, the Andresen Activator, in Norway in 1908. A number of German appliances, such as the Herbst appliance in 1934, the Bionator appliance in the 1950s and the Functional Regulator in 1966 followed on. Table 2 summarizes the various types of functional appliance that are currently in use. The Twin Block, first described by Clark in 1982, consists of two blocks with interlocking 70° bite planes, which cause forward posturing of the mandible (Figure 3). Owing to its high patient acceptance, scope for modification and ease of construction, repair and re-activation, the Twin Block is the most commonly used functional appliance in the UK. The most commonly used fixed-functional appliance is the Herbst appliance, which usually attaches to maxillary first molars and mandibular first premolars via bilateral telescopic arms which posture the mandible forward but allow opening and lateral movements (Figure 4). Other types of fixed-functional appliances, known as Class II correctors, have been described.
2 parts: maxillary and mandibular removable parts that interlock via posterior bite block with inclined bite planes to protrude mandible
Can be used with headgear and sectional upper fixed appliances Midline screw allows expansion Springs can be added to procline the upper labial segment
Good patient acceptance Cheap to make, repair and re-activate Able to eat and speak Wide range of modifications possible
Single block appliance with palatal coverage and an anterior lingual mandibular extension via rigid posts, to protrude the mandible
Can be used with a lower fixed applianceOcclusal coverage can be added to aid differential eruption of teeth
Less bulky and visible thanother appliancesDoes not cause lateral open bitesAllows posterior eruption aiding correction of a deep overbiteIncisor capping may limit lower incisor proclination
Unable to expand the maxillary archMust be removed for eatingDifficult to re-activate
Single block appliance with open palate to alter tongue proprioception and heavy labial and buccal wires to alter soft tissue forcesUpper and lower parts joined by occlusal acrylic that encourages a protrusive bite
Palatal wire can be adjusted for palatal expansion
Simple and sturdyEasy to construct and modifyLack of posterior clasps enables exfoliation of deciduous molars
Difficult to re-activateMust be removed for eating
Bass Dynamax
2 parts: upper removable plate with vertical spring projections that contact steps on the lower fixed lingual arch to protrude the mandible
Can be used with fixed appliance and headgearMaxillary expansion possiblePosterior capping
Enables incremental advancementTorque spring anteriorly allows control of maxillary incisor tipping
Prone to breakages (decementation of molar bands or fatigue of vertical spring projections)Uncomfortable on tongue
Frankel Functional Regulator
Tissue-borne appliance that aims to alter forces on the periosteum through buccal shields and postures the mandible forwards
Appliance design may be altered for correction of Class II/1, II/2 and III malocclusions
Arch expansion is facilitated through buccal shields
Can be difficult to wearDifficult to construct and modifyAcrylic buccal shields are prone to distortion/fracture
Fixed appliance made of bilateral telescopic arms connected from maxillary molar to mandibular canine causing mandibular protrusion
Can be used with fixed appliances
‘Compliance-free’ as fixedGood patient acceptanceMay be used in conjunction with a fixed applianceClinician may re-activate chairside by extending the telescopic arms
High breakage rate (decementation or separation of telescopic arms)Increased cost Increased lower labial segment proclination
Figure 3.
(a–d) Twin Block appliance.Figure 4.
(a, b) The Herbst appliance.Figure 5. Medium Opening Activator (MOA).Figure 6.
(a, b) Bionator.
The Cochrane review of Class II division 1 considered a number of high quality trials that investigated the effect of functional treatment compared to an untreated control. The combined results from the trials confirm that both early and late treatment lead to an improvement in Class II malocclusion.2 At the end of phase one of early treatment, overjet was reduced by 4.17 mm and skeletal relationship improved by 0.89°, while at the end of adolescent treatment the improvements were 5.22 mm and 2.37°, respectively.
The Twin Block appliance has been used in most studies evaluating functional appliance treatment as it is considered to be the ‘gold standard’ against which other appliances should be tested. When compared to other functional appliances, the Twin Block appliance was found to produce a statistically significant reduction in skeletal base discrepancy (ANB = -0.68 degrees; 95% CI -1.32 to -0.04) when compared to other functional appliances, although there was no significant effect from the type of appliance on the final overjet.2 The Twin Block has also been shown to cause clinically significant beneficial changes to the soft tissues.19 However, there are problems associated with the Twin Block including excessive lower incisor proclination,20 a significant failure-to-complete rate of 25%21 and a breakage rate of up to 35%.22 Lower incisor proclination occurs with most functional appliances and this must be considered during treatment planning and monitored throughout treatment. Twin Block appliances can also cause an increase in vertical dimension, which may be desirable in some cases but may not be beneficial in patients with an increased lower anterior face height. In these patients, careful control of the vertical dimension should be planned.
The success rate of the Herbst appliance, often considered to be a ‘compliance-free’ appliance, was found to be much higher than the Twin Block in one study, with a failure-to-complete rate of 12.9%.21 This is approximately half that of the Twin Block so may be considered in patients where compliance is predicted to be difficult. However, the Herbst is considerably more expensive and demonstrated a higher breakage rate so that the benefits of reduced compliance requirements must be balanced against this.
The Bass Dynamax appliance has also shown similar results to the Twin Block for overjet reduction, chin advancement and drop-out rate. However, like the Herbst, the breakage rate was significantly higher than the Twin Block, at 55%.22 Importantly, one high-quality randomized control trial comparing the Bass Dynamax appliance and Twin Block appliance had to be terminated early due to a high number of adverse events and lack of progress in the Dynamax group.23 The Frankel Regulator-2 (FR-2) and Activator appliances have both been shown to cause some improvement in Class II division 1 malocclusion, but with significant increase in lower face height with no change in mandibular length.24,25 In most cases, these changes are likely to be unfavourable.
It can be concluded that most functional appliances are able to produce some improvement in Class II malocclusions and the Twin Block appliance has been shown to produce favourable results most consistently in those who complete treatment. It must be noted that there is a considerable failure rate and wide individual variation in response to the appliances was shown by large standard deviations in the trials.
Headgear
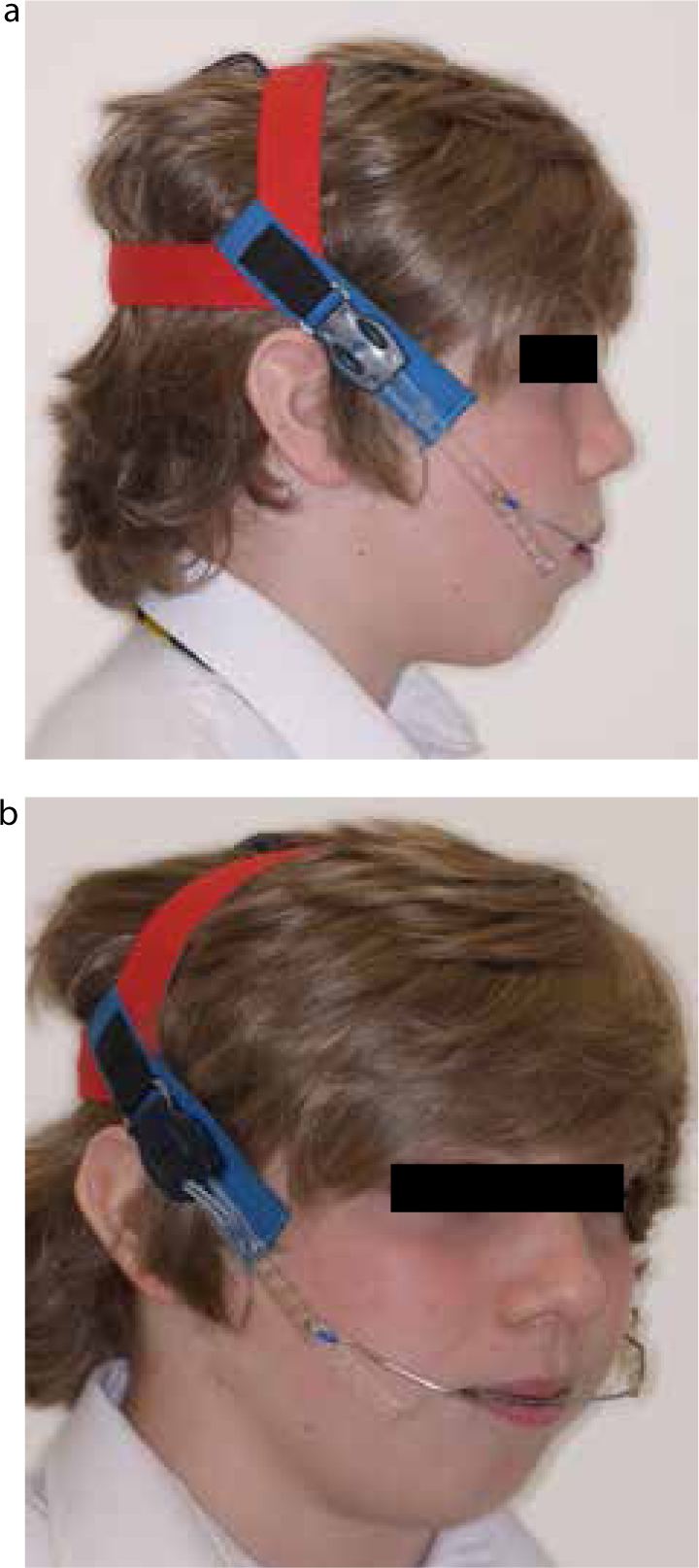
Headgear exerts force to the dentition and basal bones via extra-oral traction attached directly to bands on the teeth or to a maxillary splint or functional appliance (Figure 7). The effects are mainly dento-alveolar with some skeletal effect through restriction of maxillary downward and forward growth.15,26 Several studies found an additional small effect on mandibular growth when headgear is used in conjunction with an anterior bite plane.27
Figure 7.
(a, b) High-pull headgear. The headgear in this image has been used in conjunction with a Twin Block appliance.
The effect of headgear treatment, as early treatment, was compared to one-phase treatment, carried out later, in a study of two trials.15,27 Both found a significant reduction in overjet and improvement in skeletal relationship after headgear treatment. There was no difference in any outcomes that could be attributed to treatment timing, with the exception of risk of trauma where the later treatment group showed twice the risk of incisal trauma.2
A number of prospective trials have compared headgear to alternative methods of Class II correction. Two high quality randomized control trials compared headgear to the Bionator functional appliance and found that both treatment methods were able to correct the malocclusion by dento-alveolar correction of overjet reduction and molar distalization and a small improvement in skeletal base relationship.15,27 The Bionator had greater effect on mandibular growth while the headgear tended to exert most effect on the maxilla and maxillary teeth. Similarly, the Frankel Regulator-2 (FR-2) appliance was shown to have a comparable outcome to headgear, but through different mechanisms. Headgear produced greater molar correction and affected the maxilla only while the FR-2 affected both jaws and caused greater overjet reduction through upper incisor retroclination by the labial bow.26
Comparison between the Herbst appliance and headgear treatment found a high success rate (92.8%) for both in terms of occlusal correction. Both groups showed significantly more mandibular growth and protrusion than the controls, with an improvement in overjet and molar relationship. The Herbst group showed greater change in skeletal bases but also mandibular incisor proclination, while the headgear resulted in greater reduction in overbite and maxillary incisor retroclination.28
The Cochrane review summarizes that ‘no significant differences, with respect to final overjet, ANB, or ANB change, were found between the effects of early treatment with headgear and the functional appliances’.2 However, headgear is highly reliant on good patient compliance, with 12–14 hours a day of wearing required to achieve the effects described.
Fixed appliances
Fixed appliances can be used alone or in combination with extractions or temporary anchorage devices to retract the maxillary teeth to correct a Class II division 1 malocclusion by dental means only. Class II intermaxillary elastics are used to retract the maxillary teeth against the mandibular teeth, with reciprocal mesialization and proclination of the mandibular teeth. Currently, no high quality prospective studies have been undertaken to compare the use of maxillary extractions and Class II elastics to other methods of treating Class II malocclusion.
Extractions
The extraction of two maxillary first premolars and fixed appliance is a commonly used method of treating Class II division 1 patients. However, the decision to extract, or not, to reduce an overjet is contentious, with conflicting evidence in the literature. The main risks associated with extractions and incisor retraction is an increase in naso-labial angle and associated worsening of the facial profile. A specialist opinion is required to ensure that the patient is fully informed of the risks and benefits of extractions.
Class II intermaxillary elastics
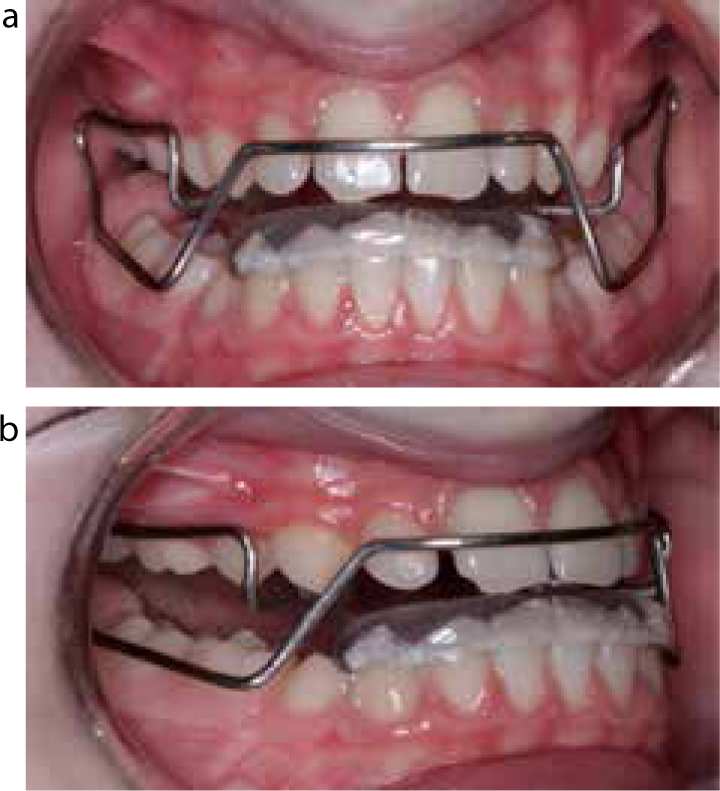
Two retrospective case-matched studies were identified which compare the effect of Class II intermaxillary elastics and fixed appliance (Figure 8) to Herbst appliances.29,30 Both appliances reduced the overjet with no significant difference in the improvements in jaw-base relationship. The fixed appliance system resulted in significantly longer total treatment time, with more relapse in overjet, greater proclination of the incisors and greater lower face height and maxillary prognathism; however, the fixed appliance system that was used in this study has been superseded, so these results may be considered outdated.
Figure 8. Class II intermaxillary elastics.
Temporary Anchorage Devices (TADs)
Temporary anchorage devices, also called mini-screws and mini-implants, provide anchorage reinforcement during labial segment retraction in Class II malocclusions. The screws bind to the alveolar bone mechanically rather than by osseointegration, enabling straightforward removal once treatment is complete. This method minimizes reciprocal tooth movement allowing full utilization of extraction spaces during labial segment retraction and provides anchorage for buccal segment distalization. TADs tend to be used in older patients and currently there are no high quality studies involving growing subjects.
Removable appliances
Upper removable appliances (URAs) are less frequently used since the widespread acceptance of fixed appliances, although URAs with anterior inclined bite plane (AIBP) have been suggested as an aid to antero-posterior correction in Class II patients. Emami and co-workers31 studied the effect of treatment with URA with AIBP in a retrospective study of 25 patients with relatively mild Class II division 1 malocclusion (overjet approximately 5 mm). The appliance was effective in correcting the overjet by proclination of the lower incisors, retroclination of the upper incisors and mandibular protrusion. Although a number of other anecdotal reports are available, insufficient high quality evidence exists to quantify the extent of possible antero-posterior correction with removable appliances.
When should general dental practitioners refer Class II patients?
Timing of referral for Class II division 1 children is extremely important as late referral may limit the treatment options available, particularly attempts at growth modification. On the other hand, recent evidence strongly suggests that there are few advantages to early treatment (undertaken as a first stage of treatment in the early mixed dentition) for Class II division 1 malocclusion and that starting treatment too early may actually reduce success and long-term outcome. It is therefore now recommended that a single phase of treatment is undertaken once the patient is in the late mixed dentition or early permanent dentition. This is the ideal time for orthodontic referral for the majority of Class II growing patients.
The exceptions to this are if there is a significant risk of incisal trauma due to greatly increased overjet, or if the child is being teased or bullied at school. For these patients, early treatment may be indicated and an earlier referral should be made for an orthodontic opinion.2
Conclusions
Most functional appliances cause some improvement in the Class II division 1 malocclusion compared to a control, with similar treatment times. A notable failure-to-complete rate is associated with functional appliances.
Headgear is a successful alternative treatment to functional appliances for the management of Class II malocclusion. Headgear tends to have a small restraining effect on the maxilla, with a large component of correction achieved by dento-alveolar change. Headgear may be a more appropriate choice in patients where diagnosis indicates the origin of the skeletal discrepancy is a protrusive maxilla rather than retrognathic mandible. However, high patient compliance is essential for success.
Currently, there is insufficient high quality evidence to assess whether maxillary premolar extraction, Class II intermaxillary elastics, TADs and removable appliances are effective alternatives to other methods of Class II management in the growing patient.
There appears to be no advantage in early treatment for Class II patients, with the exception of patients who are deemed to be at significant risk of incisal trauma due to greatly increased overjet, or if the child is being teased or bullied at school.