Porter RWJ, Poyser NJ, Briggs PF. A life threatening event from poorly managed dental pain − a case report. Br Dent J. 2007; 202:203-206
Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 1: aetiology and diagnosis. Br Dent J. 2010; 208:459-463
Matthews RW, Peak JD, Scully C. The efficacy of management of acute dental pain. Br Dent J. 1994; 176:413-416
Carrotte P. Endodontics: Part 3 Treatment of endodontic emergencies. Br Dent J. 2004; 197:299-305
Meechan JG. Why does local anaesthesia not work everytime?. Dent Update. 2005; 32:(2)66-72
Meechan JG. How to overcome failed local anaesthesia. Br Dent J. 1999; 186:(1)15-20
Meechan JG. Articaine and lignocaine. Evid Based Dent. 2011; 12:(1)21-22
Srinivasan N, Kavitha M, Loganathan CS, Padmini G. Comparison of anesthetic efficacy of 4% articaine and 2% lidocaine for maxillary buccal infiltration in patients with irreversible pulpitis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107:133-136
Kanaa MD, Whitworth JW, Corbett IP, Meechan JG. Articaine buccal infiltration enhances the effectiveness of lidocaine inferior alveolar nerve block. Int Endod J. 2009; 42:(3)238-246
Kanaa MD, Whitworth JW, Meechan JG. A comparison of the efficacy of 4% articaine with 1:100,000 epinephrine and 2% lidocaine with 1:80,000 epinephrine in achieving pulpal anesthesia in maxillary teeth with irreversible pulpitis. J Endod. 2012; 38:(3)279-282
Kuriyama T, Absi EG, Williams DW, Lewis MA. An outcome audit of the treatment of acute dentoalveolar infection: impact of penicillin resistance. Br Dent J. 2005; 198:759-763
Ellison SJ. An outcome audit of three day antimicrobial prescribing for the acute dentoalveolar abscess. Br Dent J. 2011; 211:591-594
Pain is one of the major reasons that lead patients to seek dental care. For the majority of patients, the pain is of odontogenic origin, as a consequence of dental disease. The timely diagnosis and management of dental pain is an essential component of dental care, and this article reminds readers of the common presenting symptoms of simple dental pain, diagnoses and pragmatic management.
Clinical Relevance: Pain of odontogenic origin is common, and distressing. However, the pathology is consistent, as are the symptoms, and an understanding of this underpins the careful history-taking that will lead the clinician to the diagnosis.
Article
Dental or odontogenic pain is common. In the Adult Dental Health Survey 2009, 9% of patients reported pain at the time of examination, and 8% reported pain frequently in the preceding 12 months and, for some, pain is the primary reason for attendance.1 As with all patients, a thorough history of symptoms should be taken from the patient, along with the medical and social history. The responses may then be interpreted in light of the clinical examination. As with all histories, a systematic approach helps to avoid missing important detail, and elicits the key factors in the history.
Pain of odontogenic origin might be divided into three categories:
That directly related to pulpal pathology;
That related to soft tissue pathology; and
That related to trauma.
Each condition produces characteristic and consistent pathological changes, for example appendicitis always follows the same process so, as a consequence, any condition will present with a range of symptoms and signs that are specific to that condition. Whilst there may be overlap, or a combination of symptoms or multiple conditions, the basic premise holds firm for all conditions. This concept was outlined by Osler in the early 1900s with his advice to colleagues and summarized as ‘listen to the patient – he is telling you the diagnosis’.2 This advice still holds true over a century later, and is based on the principle that symptoms reflect pathology. The corollary from this is that, without a diagnosis, treatment should not be instituted.
Common key symptoms of dental (odontogenic) pain
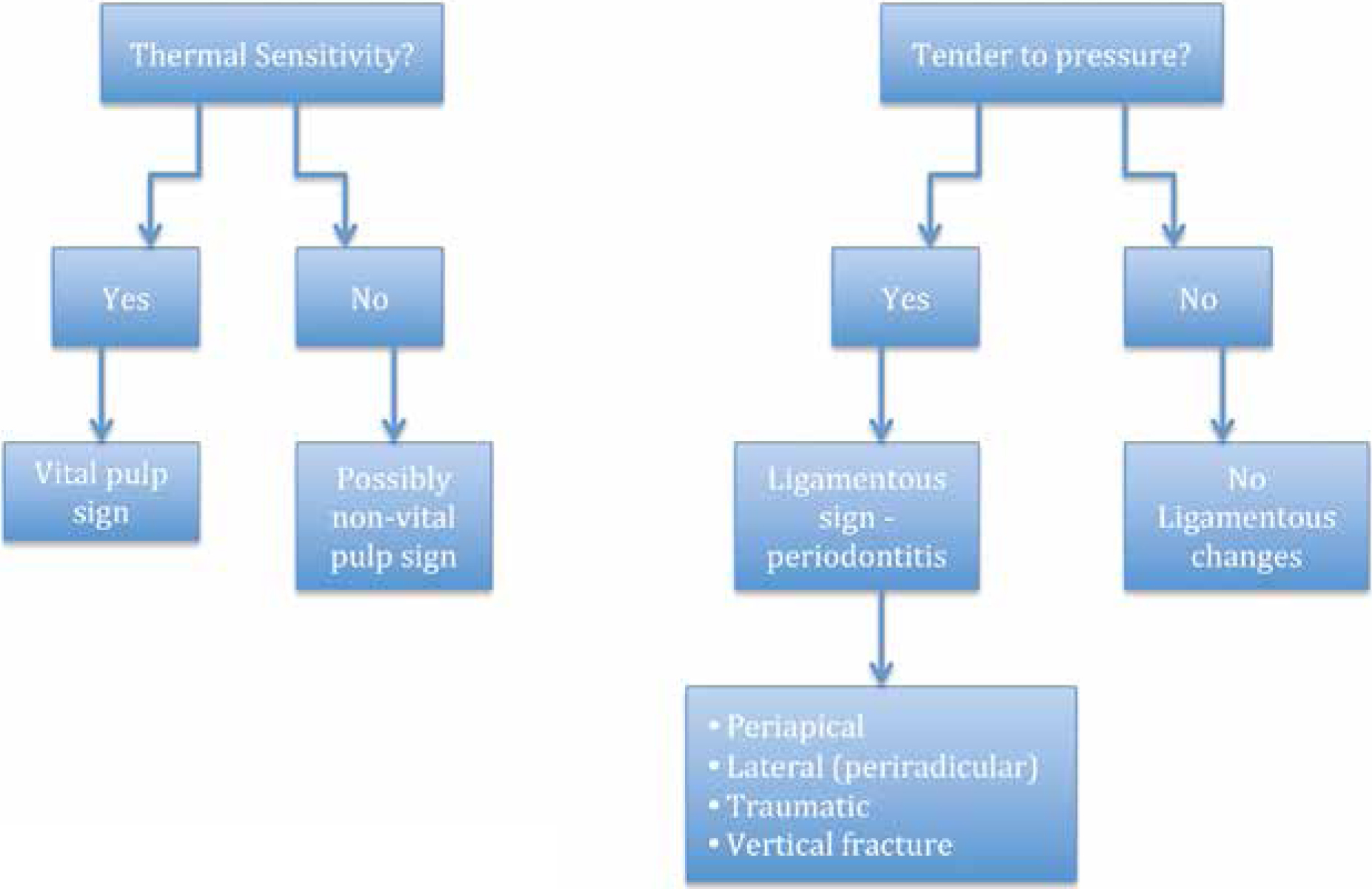
If Osler's advice is followed, then the most important part of any examination is the history, to identify the symptoms associated with the condition. For pain of odontogenic origin, there are two broad symptom groups: thermal sensitivity, and tenderness to pressure (Figure 1).
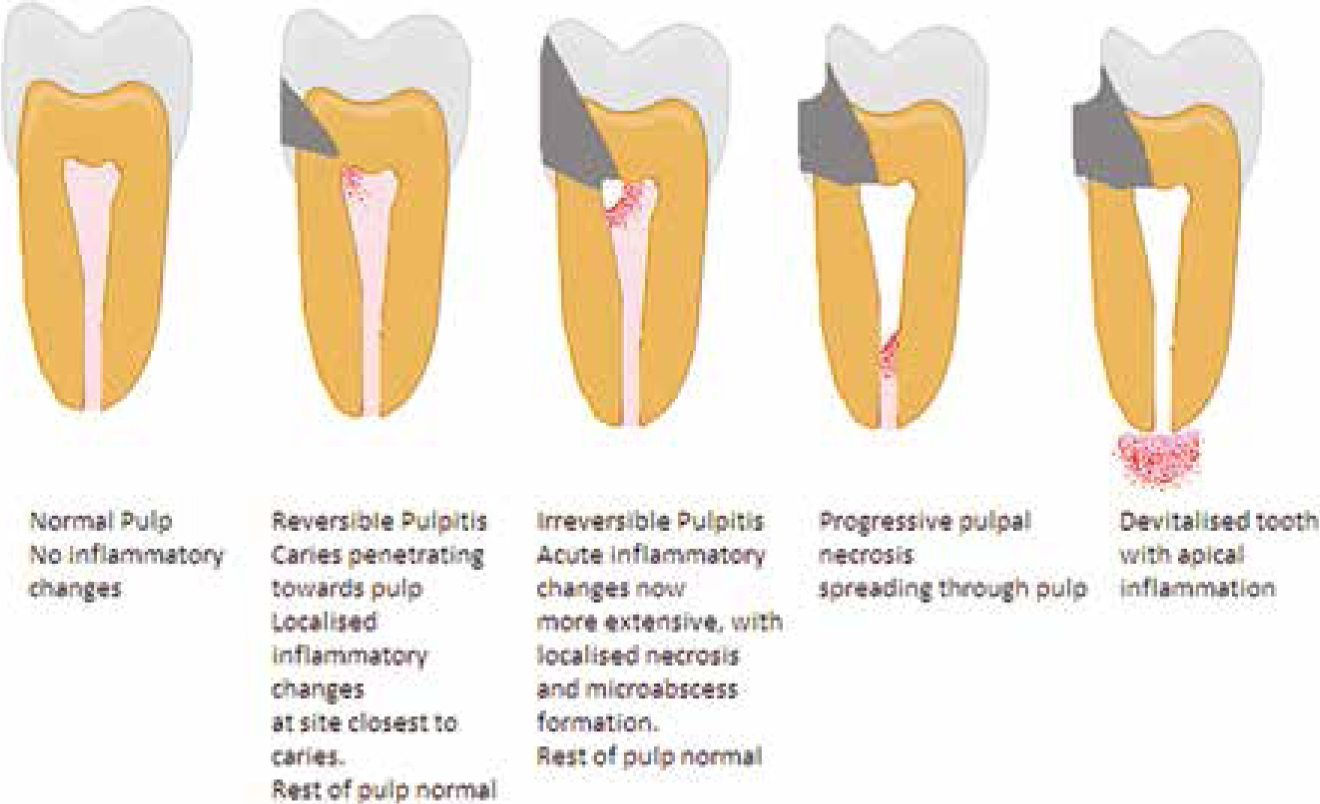
Symptoms related to pulpal pathology will typically show changes in response to normal stimuli (Figure 2). A patient reporting responses to thermal or osmotic stimulus indicates a response from the pulp.3 Inflammatory changes in the pulp, or pulpitis, lead to increasingly significant responses to thermal or osmotic stimulus, as distinct from the more normal and brief response seen with dentine sensitivity. In early stages, this may be reversible, but as the pathology becomes more advanced the process becomes irreversible, and eventually there is uncoupling of the response from the stimulus – or the evolution of spontaneous pain. When pulpitis is irreversible, typically patients report spontaneous, often continuous, pain, often significantly increased with stimulus, although occasionally cold may actually offer brief relief from the pain of a very painful irreversible pulpitis.4 Localization may be difficult. Sleep disturbance is also considered an aspect of irreversible pulpitis, but this is non-specific, as sleep may also be disturbed by a range of other conditions, examples being acute urinary retention to a fractured femur. Rather it is a descriptor of the significance of the pain the patient is suffering, and thus of the extent to which the pathology has progressed.
Figure 2. Dental pulp pathology and its progress.
Whilst such pulpal changes are typically the result of carious destruction of coronal tissues, it is important to remember that a recently placed, large restoration may be an effective pulpal irritant, leading to temporary pulpitis and attendant pain with hypersensitivity. It is also important to appreciate that this may be irreversible.
Tenderness to pressure
Patients may report that the nature of their pain is non-responsive to thermal or osmotic stimuli, but that the tooth can be easily localized, and is tender to pressure – typically on biting, and they frequently report a steady throbbing sensation, which may also disturb sleep. This symptom group relates to inflammatory changes and oedema within the periodontal ligament, typically apical, although lateral (peri-radicular) ligamentous inflammation will produce almost identical symptoms, but may be distinguished by vitality in some cases, along with assessment of the periodontal health. The key here is the understanding that tenderness to pressure indicates a ligamentous issue. Finger pressure, rather than tapping with a mirror, may be a more accurate assessment of this symptom. Ligamentous symptoms also follow trauma – either intra-oral, such as a new high restoration or bruxing or, alternatively, external from a blow. Assessment and exclusion of recent trauma should form part of the history and examination.
Cracked cusp
It is, however, important to distinguish ligamentous involvement from those symptoms of a cracked cusp, which is also tender to pressure. However, here the response is brief, lasting only whilst the stimulus exists, and typically on either application or release of pressure.5 It is unlikely that a response will be initiated by finger pressure alone, unless the cusp has actually fractured, and is only retained in place by the gingival cuff, which will produce exquisite pain on touching the cusp, which is obviously mobile. In most cases, the tooth is vital, and may eventually develop symptoms of pulpitis. For such teeth the use of cotton wool rolls or a ‘tooth sleuth’ in occlusion, or transillumination,5 may help to pinpoint the cusp in question. This can be followed by removal of old restorations to explore the cavity base to identify the fracture, which may require magnification to identify (Figure 3).
Figure 3. Cracked distopalatal cusp identified in upper molar following exploration.
The discomfort from ‘Cracked tooth syndrome’ may be inconsistent, with pain-free periods, and biting on the offending tooth not always causing pain, making the diagnosis very difficult. The tooth may be heavily filled with cracked cusps or, alternatively, but less frequently, a middle-aged otherwise unrestored tooth.
Tooth surface loss
The patient may be a bruxist with attrition or have severe dental erosion or abrasion that may lead to sensitivity and increase the risk of pulpal exposure, and eventual devitalization.
Soft tissue pain
Pain from the soft tissues presents with variable qualities, typically soreness, burning, or sharp pain, related directly to the area of ulceration, inflammation or trauma. Important aspects of mucosal pain relate to the areas involved – generalized or specific – and reflect the nature of the pathology; a chronic atrophic candidiasis will present with generalized soreness, whereas a traumatic ulcer or pericoronitis will be pinpointed, and with some there may be associated signs, such as foetor oris with acute necrotizing ulcerative gingivitis (ANUG).
Neuropathic dental pain
It is important to remember that, if a patient has had persistent symptoms of dental pain, with or without multiple dental restorative interventions, the clinician can simply confirm an inflammatory component of the pain by asking the patient if the pain responds to anti-inflammatory medications (aspirin, ibuprofen or paracetamol). If there is an infective component, the dental pain will also subside with antibiotics. If the patient confirms that the dental ‘toothache’ type pain persists even with anti-inflammatory analgesics, then it is prudent to consider the possibility of neuropathic pain. Referral to a pain specialist or his/her GMP may be preferable to persisting with dental interventions in trying to manage the pain early on. Whilst unusual, this ‘trap’ may draw the well-meaning practitioner into repeated ineffective treatments. Patients with neuropathic pain will often be late middle-aged and may be experiencing other forms of neuropathic pain, including fibromyalgia, headaches, back pain and joint pain.
Examination
A thorough examination of all the tissues with a systematic approach is required. Although, in many cases, the diagnosis is clear, in some it is not, and irreversible pulpitis can be extremely difficult to localize. A patient with a heavily restored dentition may present with a number of potential sites for symptoms of pulpitis, and careful vitality testing is required to help confirm the diagnosis (see below).
Likewise, in some cases of pulpitis, it may be impossible for the patient even to localize to the upper or lower arch, and the use of local anaesthesia as a diagnostic aid should not be underestimated. Local anaesthesia is also the most effective method of delivering pain relief for patients who are suffering severe dental pain, and the timely administration of a good anaesthetic for pain control only allows relaxation of the patient. Severe pain often leads to changes in patient behaviour, such as increased aggression, or reduced communication, and the abolition of the pain suffered will allow the patient to respond more normally, and have the ability to discuss and consider treatment options in a more normal way, and co-operate with treatment. Long-acting anaesthetics offer potentially significant advantages for pain control.
Inflammation and swelling of the soft tissues is a key finding during examination. In the majority of cases, this will occur close to the source of the infection, ie the tooth. The overlying mucosa may show inflammation, and also becomes tender to finger pressure. Changes closer to the gingival margin suggests an origin on the lateral aspect of the ligament, whereas changes appearing in the sulcus suggests an apical origin (Figure 4). Inflammation related to pericoronitis tends to present with localized pain, but may present with more significant swelling, discharge or ulceration (Figure 5).
Figure 4. Swelling in buccal sulcus, originating from apical infection. Note: periodontal origin will appear in the gingival tissues.Figure 5. Severe ulceration associated with pericoronitis.
Vitality testing
Vitality testing relies on providing a stimulus to the pulp to observe the response to the stimulus. Three aspects exist:
Application of cold, such as ethyl chloride;
Application of heat, such as warmed greenstick; and
The use of electronic testers.
Vitality testing is often considered unreliable, particularly with electronic pulp testers and in the presence of crowns (despite the fact that many crowns contain a core of metal which is an effective conductor), but this misses the point: it is in the contextual interpretation that vitality testing provides information to facilitate diagnosis. Control testing should be used to help provide context, and a tooth that clearly produces a hypersensitive response is much easier to distinguish as the likely source of symptoms than others that are showing little response in a group of heavily restored teeth.
A problem that often leads to confusion with vitality testing is when mixed symptoms present – teeth that show obvious tenderness to pressure, but also respond to vitality testing, particularly cold. This combination of features typically appears in a multi-rooted tooth, and is likely to represent a situation where pulp necrosis is progressive, but not complete, where one or more root(s) retains vitality, whilst the other(s) become necrotic, and develop signs of apical inflammatory changes. This may also represent a simple stimulus of the inflamed ligament by the pressure of application of the vitality testing process.
Radiographs
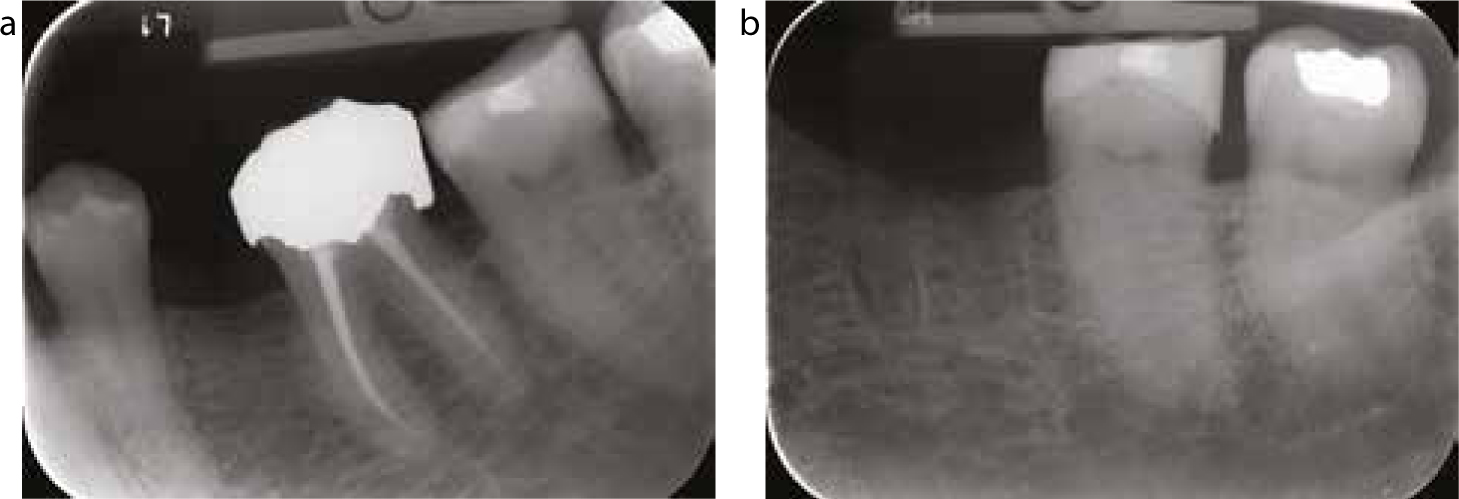
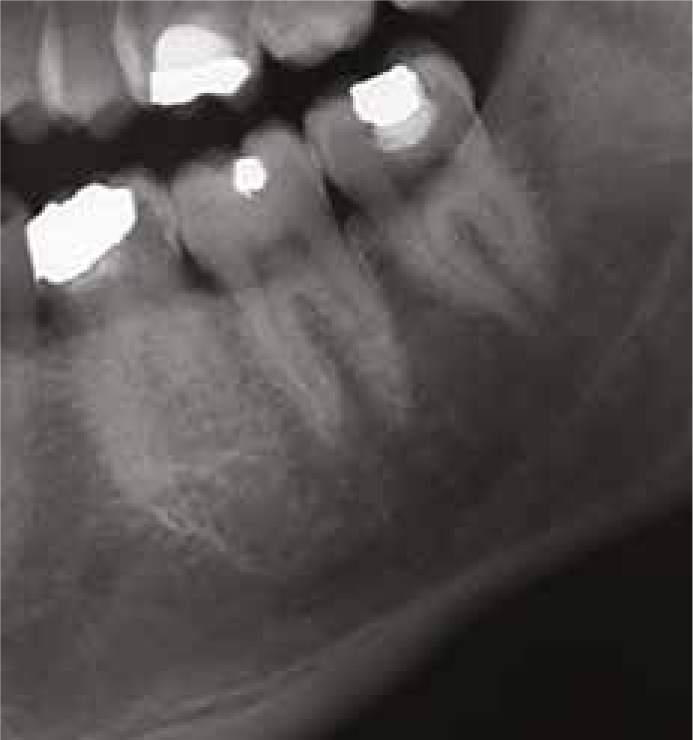
Radiographs provide invaluable information but, with the exception of approximal caries, are rarely diagnostic in their own right. As with vitality testing, this information should be used in context; for example, pulpal sclerosis may be indicative of a pulp that is showing progressive irreversible changes, and may support the diagnosis of a pulpitis in the tooth. Figures 6 a and b demonstrate these changes in a lower second molar over a seven month period. Radiographs offer essential information to allow treatment planning following diagnosis.
Figure 6.
(a, b) Radiographs 7 months apart demonstrating progressive sclerosis of pulp in lower second molar consistent with a pulpitis.
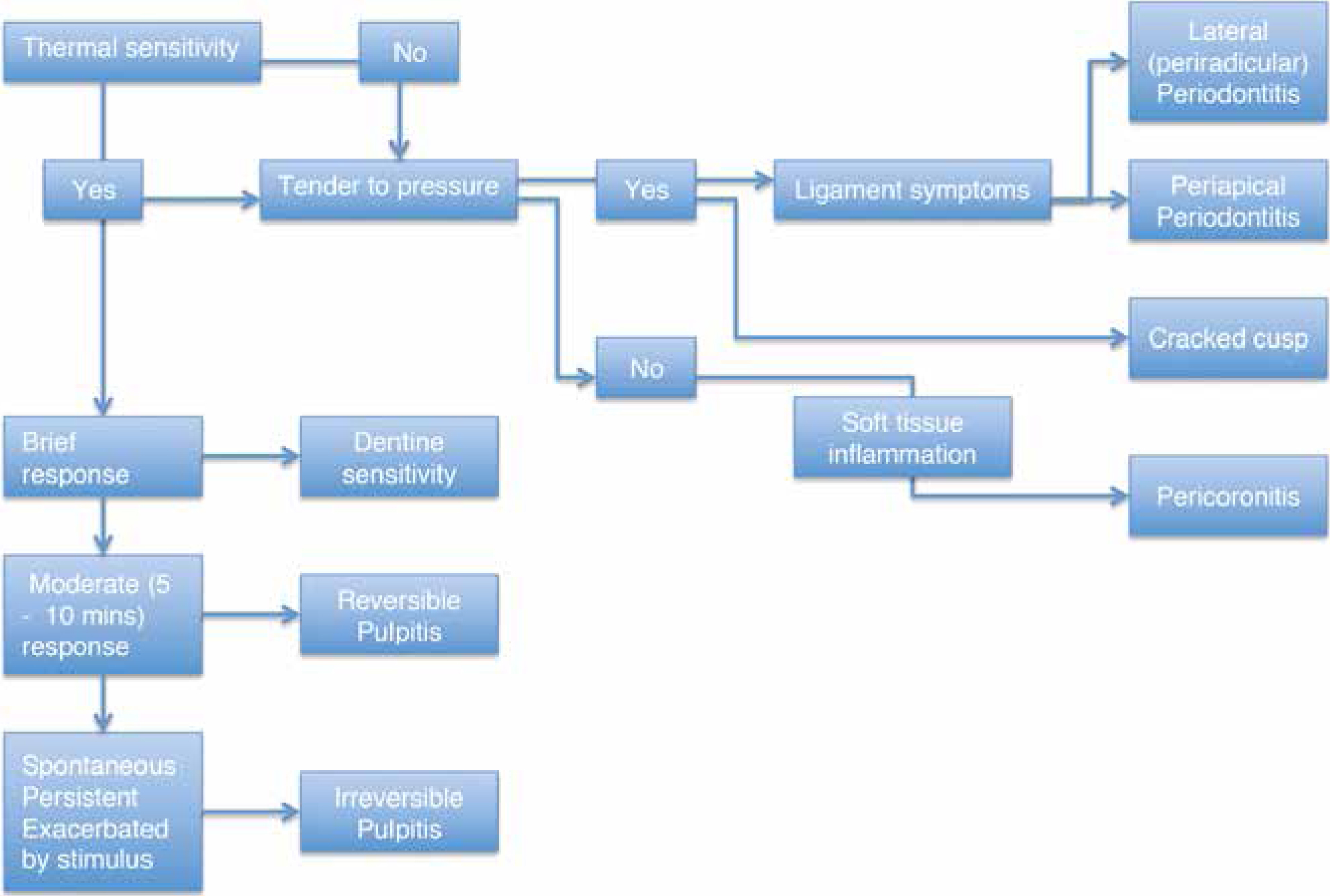
Figure 7. Summary of diagnostic flow in acute odontogenic pain.
Treatment of pain
The key issue is the diagnosis of the patient's symptoms. Once this is made, treatment may be planned, and this follows a logical process (Figure 8):
Figure 8. Treatment decision tree.
Is the tooth in question restorable or not?
Is endodontic treatment necessary and possible?
If the tooth is unrestorable (by virtue of caries or periodontal destruction), or the patient does not wish to retain the tooth, then the decision is straightforward, and extraction is indicated.
For those restorable teeth, initial treatment should be directed to pain relief. This will require a dressing to the tooth, with removal of caries as appropriate. Reversible pulpitis may be treated with a simple calcium hydroxide (Ca(OH)2) and zinc oxide/eugenol (ZnOE) dressing, or an appropriate restorative such as a glass ionomer cement to seal the cavity. Calcium hydroxide has the advantages of being bacteriocidal, and encourages remineralization activity within pulpal tissue, whilst ZnOE, although an older material, still has the advantage of being sedative to the pulp. An irreversible pulpitis, however, requires definitive intervention, and pulpectomy is the only appropriate treatment for pain control. The root canals may then be dressed with Ca(OH)2 or antibiotic/steroid (Ledermix) paste, and a good coronal seal placed to prevent contamination of the canal. The key factor in pain control is effective removal of the inflamed tissue of the pulp.
For periapical periodontitis, decompression of the periapical area is essential to reduce pain. Opening and debriding of the root canals followed by a dressing of Ca(OH)2 will decompress the apical tissues6,7 and decontaminate the root canals, allowing resolution of symptoms by removal of the source of the contamination of the periodontal ligament. However, problems arise when the tooth is already root-filled; for such cases it may be possible to remove the old root filling to allow access to the whole canal for dressing.
For those cases presenting with an acute periodontal episode (lateral or peri-radicular periodontitis), where the tooth is likely to survive, curettage of the pocket and root surface debridement under local anaesthesia will typically produce rapid resolution.
Hot pulp
The phenomenon of the ‘hot pulp’ appears intermittently. This occurs when an irreversible pulpitis becomes very difficult to anaesthetize, and appears resistant to conventional local anaesthesia. Meechan has described a number of management approaches for failed anaesthesia.8,9 pH changes in areas of inflammation are often blamed for resistance to local anaesthetics,9 inhibiting dissociation of the anaesthetic molecule, yet in this situation there is no inflammation in the periapical tissues that might inhibit anaesthetic activity and lead to the failure of analgesia. It is likely that this reflects hyperalgesia of the nerves to the pulp, which are hence unstable, and initiate an action potential at a lower threshold.
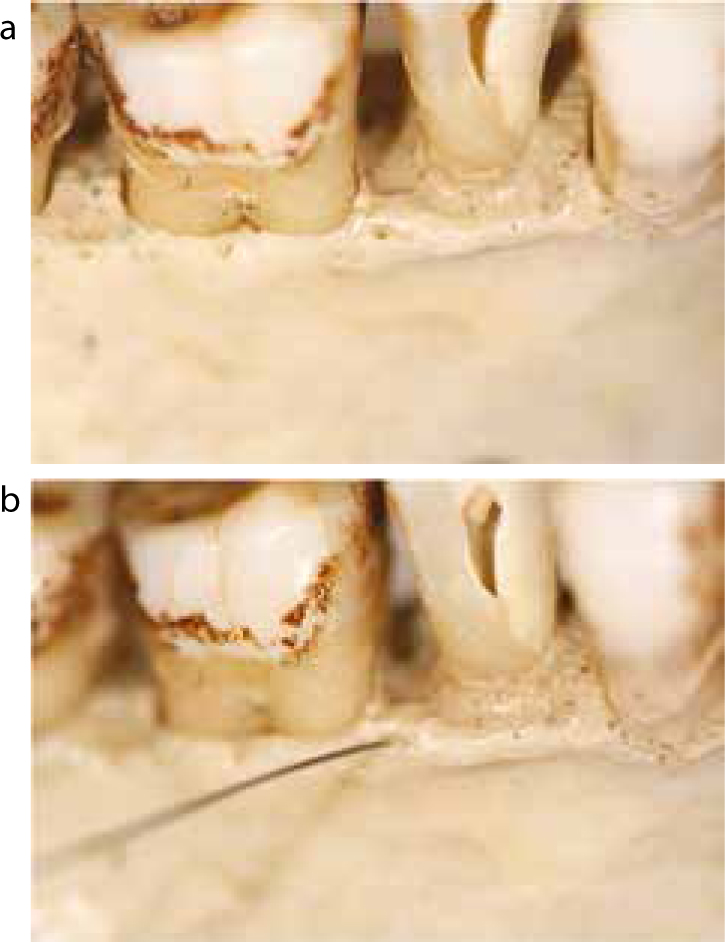
This is a challenging clinical problem, and can only be overcome by increasing the dose of anaesthetic in the area,9 with increased accuracy of the placement of the anaesthetic solution. In most cases, this means applying the solution as close to the pulp as possible, and intra-ligamentary or intra-osseous approaches are most effective for this. In a number of patients, careful probing will allow identification of a small bony canaliculus in the alveolar crestal bone, where it is possible to insert a fine (30/31g) needle, and instil the anaesthetic solution directly into the cancellous bone (Figures 9 a and b). Patients should be warned of a brief sensation of palpitations as some anaesthetic solution will escape into the general vascular circulation. This also means that duration of anaesthesia will be limited, and is often no more than 20–30 minutes.
Figure 9.
(a, b) Small interdental canaliculi allow access to cancellous bone for anaesthesia.
In some cases, intra-pulpal injection of solution is possible, and is usually highly effective, although briefly painful; in this approach it is usually best to insert the needle as far as possible down the root canal, rather than just attempting to infiltrate the coronal pulp. Articaine 4% may be helpful in these difficult cases,10,11,12 although this may be inconsistent,13 and may also be used as an infiltration palatal to an upper tooth, and buccal to a lower molar, to supplement conventional approaches.12
An increased dose of anaesthetic is typically required to achieve anaesthesia in these cases. Infiltrations or blocks typically require repeating, to achieve field anaesthesia, and it is often necessary to administer 0.75–1 ml in the periodontal/intraosseous interface area to achieve anaesthesia.
Teeth that are likely to produce difficulties leading to a hot pulp are difficult to identify, but sometimes a history of an irreversible pulpitis, in combination with the radiographic signs of moderate sclerosis of the pulp, can suggest the potential for difficulties (Figure 10).
Figure 10. ‘Hot pulp’ sometimes indicated by sclerotic pulp – as in this lower first molar.
Swelling
Significant facial or intra-oral swelling indicates abscess formation, or a cellulitis. Drainage is the primary method of management of swelling, and localization of pus allows for drainage, leading to rapid resolution of symptoms. Anaesthesia for this is always challenging, but block anaesthetics can be very helpful in providing pain relief during incision and drainage, and avoid the need to inject into an infected site. The key to this is often the timing of the incision, and a short delay to allow localization of pus is sometimes necessary. Systemic antibiotic therapy may be necessary to control systemic and local spread to surrounding tissues, but should not be used to substitute for active therapeutic intervention, as the evidence is clear that active intervention provides the best outcome,14,15 and simple antibiotic prescribing alone is inappropriate. Indicators for the use of antibiotics include:
Pyrexia (oral temperature >37°C);
Lymphadenopathy;
Severe local swelling (including closure of the eye);
Dysphagia; and
Rigors.
A spreading cellulitis is of concern and, when involving multiple fascial spaces, can become a surgical emergency. Ludwig's Angina is a classic example of this, and this should be treated vigorously. Referral to a maxillofacial department for management is mandatory.
Extraction
For cases where extraction is indicated, the decision must be influenced by the complexity of extraction, and an assessment of this must be made. Extractions may be complex, and may require specialist input. In such cases, dressing of the tooth is still appropriate to stabilize the pathology, and provide symptom control, whilst other arrangements are made. Thus a key aspect of any management strategy for acute dental pain will be to undertake initial control of acute pain, whilst arranging further definitive treatment to be completed later. In many cases, this will require drainage, and dressing of the tooth to control the symptoms.
Unfortunately, extractions do not always proceed simply, and teeth and roots do fracture during removal. Indeed, sometimes teeth appear extremely resistant to conventional extraction. If possible, immediate surgical removal is ideal, however, the operator should make the assessment of the required surgical process. Simple attempts to elevate fractured roots, in an environment where access to an application point does not exist, traumatizes tissues, and leads to significantly increased post-operative pain (Figure 11). Bone removal is mandatory to allow access to an application point for an elevator. If removal is not possible, then again the tooth or roots should be treated to control pain. A vital pulp should be removed and the root canals dressed, and non-vital teeth should be opened for drainage, whilst referral is made to an appropriate specialist. A simple rule of thumb that practitioners may like to consider is that most routine extractions should take no more than 10 minutes. If the extraction is not progressing, the process should stop, and be reassessed to identify the problems and formulate strategies for their management.
Figure 11. Fracture during extraction – access to roots requires surgical intervention.
Pericoronitis and acute ulcerative necrotizing gingivitis (ANUG)
Pericoronitis may be extremely painful, and produce severe tissue destruction (Figure 5). The implicated organisms are typically anaerobes. However, as with other conditions, the primary aspects of the management of pericoronitis looks at the treatment of local factors, such as the removal of traumatizing opposing cusps or tooth, irrigation of the area with chlorhexidine, disruption of the bacterial ecology with ultrasonic scaling, and even hydrogen peroxide as a mouthwash. In the more severe cases, with signs justifying its prescription, metronidazole would be the antibiotic of choice. In some cases, extraction of the tooth may be necessary once the acute phase has passed.
ANUG may also be exquisitely painful, with generalized pain and necrosis of gingival tissues, classically, with loss of interdental papillae as a consequence of anaerobic bacterial infection. Early intervention to control tissue destruction is essential, and metronidazole 200 mg orally three times a day, for three days, is indicated as part of the management regimen, in combination with local interventions such as scaling, chlorhexidine or hydrogen peroxide mouthwashes, and oral hygiene procedures.
Summary
Odontogenic pain is common, and a frequent reason for presentation. Most cases give clear histories that guide the clinician towards the diagnosis, with the primary discriminator being thermal sensitivity indicating a pulpal issue, or tenderness to pressure indicating ligamentous issues. Pain control is the primary need in management of the patient, and relies upon simple techniques of intervention to bring about relief of symptoms, that typically resolve rapidly.