Porter SR, Hegarty A, Kaliakatsou F, Hodgson TA, Scully C. Recurrent aphthous stomatitis. Clins Dermatol. 2000; 18:569-578
Carew O'Donnell S, Marshman Z, Zaitoun H. ‘Surviving the sting’: the use of solicited diaries in children and young people with oral mucosal disease. Int J Paediatr Dent. 2013; 33:352-358
Scully C. Aphthous ulceration. N Engl J Med. 2006; 335:165-172
Le Doare K, Hullah E, Challacombe S, Menson E. Fifteen-minute consultation: a structured approach to the management of recurrent oral ulceration in a child. Arch Dis Child Educ Pract Ed. 2013; 99:82-86
Kozlak ST, Walsh SJ, Lalla RV. Reduced dietary intake of vitamin B12 and folate in patients with recurrent aphthous stomatitis. J Oral Pathol Med. 2010; 39:420-423
Lopez-Jornet P, Camacho-Alonso F, Martos N. Hematological study of patients with aphthous stomatitis. Int J Dermatol. 2014; 53:159-163
Felix D, Luker J, Scully C. Oral medicine: 1. Ulcers: aphthous and other common ulcers. Dent Update. 2012; 39:(7)513-519
Jurge S, Hegarty AM, Hodgson T. Orofacial manifestations of gastrointestinal disorders. Br J Hosp Med (Lond). 2014; 75:(3)497-501
Scully C, Gorsky M, Lozada-Nur F. The diagnosis and management of recurrent aphthous stomatitis. A consensus approach. J Am Dent Assoc. 2003; 134:(2)200-207
Patel P, Brostoff J, Campbell H, Goel RM, Taylor K, Ray S, Lomer M, Escudier M, Challacombe S, Spencer J, Sanderson J. Clinical evidence for allergy in orofacial granulomatosis in inflammatory bowel disease. Clin Transl Allergy. 2013; 3:(1)
Amir J, Harel L, Smetana Z, Varsano I. The natural history of primary herpes simplex type 1 gingivostomatitis in children. Treatment of herpes simplex gingivostomatitis with aciclovir in children: a randomised double blind placebo controlled study. Br Med J. 1997; 314:(7097)1800-1803
Sakane T, Takeno M, Suzuki N, Inaba G. N Engl J Med. 1999; 341:1284-1291
Shephard M, Hodgson T, Hegarty AM. Vesiculobullous disorders affecting the oral cavity. Br J Hosp Med (Lond). 2014; 75:(9)502-508
Brocklehurst P, Tickle M, Glenny AM, Lewis MA, Pemberton MN, Taylor J, Walsh T, Riley P, Yates JM. Systemic interventions for recurrent aphthous stomatitis (mouth ulcers). Cochrane Database Syst Rev. 2012; (9) https://doi.org/10.1002/14651858.CD005411.pub2
Jurge S, Kuffer R, Scully C, Porter SR. Mucosal diseases series No VI. Recurrent aphthous stomatitis. Oral Dis. 2006; 12:1-21
Ślebioda Z, Szponar E, Kowalska A. Etiopathogenesis of recurrent aphthous stomatitis and the role of immunologic aspects: literature review. Archiv Immunol Therap Experimental. 2014; 62:(3)205-215
Shim YJ, Choi JH, Ahn HJ, Kwon JS. Effect of sodium lauryl sulfate on recurrent aphthous stomatitis: a randomized controlled clinical trial. Oral Dis. 2012; 18:(7)655-660
Addy M, Carpenter R, Roberts WR. Management of recurrent aphthous ulceration – a trial of chlorhexidene gluconate gel. Br Dent J. 1976; 141:118-120
Nolan A, Baillie C, Badminton J, Rudralingham M, Seymour RA. The efficacy of topical hyaluronic acid in the management of recurrent aphthous ulceration. J Oral Pathol Med. 2006; 35:461-465
Preshaw PM, Grainger P, Bradshaw MH, Mohammad AR, Powala CV, Nolan A. Subantimicrobial dose doxycycline in the treatment of recurrent oral aphthous ulceration: a pilot study. J Oral Pathol Med. 2007; 36:(4)236-240
Brown RS, Bottomley WK. Combination immunosuppressant and topical steroid therapy for treatment of recurrent major aphthae: a case report. Oral Surg Oral Med Oral Pathol. 1990; 69:(1)42-44
Mimura MA, Hirota SK, Sugaya NN, Sanches Jr JA, Migliari DA. Systemic treatment in severe cases of recurrent aphthous stomatitis: an open trial. Clinics (Sao Paolo). 2009; 64:(3)193-198
Katz J, Langevitz P, Shemer J, Barak S, Livneh A. Prevention of recurrent aphthous stomatitis with colchicine: an open label trial. J Am Acad Dermatol. 1994; 31:(3)459-461
Revuz J, Guillaume JC, Janier M Crossover study of thalidomide vs placebo in severe recurrent aphthous stomatitis. Arch Dermatol. 1990; 126:(7)923-927
Fleming FJ, Vytopil M, Chaitow J, Jones R, Darras BT, Ryan MM. Thalidomide neuropathy in childhood. Neuromuscular Disord. 2005; 15:172-176
Powell RJ, Gardner-Medwin JM. Guidelines for the clinical use and dispensing of thalidomide. Postgrad Med J. 1994; 70:901-904
Zeldis JB, Williams BA, Thomas SD, Elsayed ME. S.T.E.P.S.: a comprehensive program for controlling and monitoring access to thalidomide. Clin Ther. 1999; 21:(2)319-330
Krisdapong S, Sheiham A, Tsakos G. Impacts of recurrent aphthous stomatitis on quality of life of 12- and 15-year-old Thai children. Qual Life Res. 2012; 21:(1)71-76
Gherunpong S, Tsakos G, Sheiham A. The prevalence and severity of oral impacts on daily performances in Thai primary school children. Health Qual Life Outcomes. 2004; 2
Verbrugge LM. Health Diaries. Med Care. 1980; 18:(1)73-95
Rosethal GE, Shannon SE. The use of patient perceptions in the evaluation of healthcare delivery systems. Med Care. 1997; 35:(11)NS58-NS68
Management of recurrent aphthous stomatitis in children Jodie A Montgomery-Cranny Ann Wallace Helen J Rogers Sophie C Hughes Anne M Hegarty Halla Zaitoun Dental Update 2024 42:6, 707-709.
Authors
Jodie AMontgomery-Cranny
BDS(Hons), BSc(Hons), MBCHB(Hons)
Specialty Registrar in Oral Medicine, Charles Clifford Dental Hospital, Sheffield, S10 2SZ, UK
Academic Clinical Fellow in Paediatric Dentistry, Unit of Oral Health and Development, School of Clinical Dentistry, University of Sheffield, Claremont Crescent, Sheffield, S10 2TA, UK.
Recurrent oral ulceration is common and may present in childhood. Causes of recurrent oral ulceration are numerous and there may be an association with underlying systemic disease. Recurrent aphthous stomatitis (RAS) is the most common underlying diagnosis in children. The discomfort of oral ulcers can impact negatively on quality of life of a child, interfering with eating, speaking and may result in missed school days. The role of the general dental practitioner is to identify patients who can be treated with simple measures in primary dental care and those who require assessment and treatment in secondary care. Management may include topical agents for symptomatic relief, topical corticosteroids and, in severe recalcitrant cases, systemic agents may be necessary.
CPD/Clinical Relevance: Children and young people frequently suffer from recurrent oral ulceration; with recurrent aphthous stomatitis being the most common diagnosis.
Article
In simple terms, an ulcer is a full thickness breach of the epithelium. There are numerous causes of oral ulceration in both adults and children, with recurrent aphthous stomatitis (RAS) being the most common cause; it is reported to affect up to 40% of children.1 The degree of pain and psychological distress caused by ulcers is variable and management should encompass acknowledgement of their impact on quality of life.2
RAS represents a genetic predisposition to oral ulceration. Inheritance is thought to be polygenic with no specific genes or HLA types yet identified.3 Identifying those for whom the possibility of undiagnosed systemic disease needs to be investigated and those who do not respond to simple management strategies is of crucial importance to reduce patient morbidity and maintain high standards of care.3
Diagnosis
A diagnosis of recurrent aphthous stomatitis (RAS) is usually reached following a thorough clinical history (Table 1), together with the physical appearance of the ulcer, if present at the time of examination.4,5 Predisposing factors in children and young people include trauma, stress, hormonal imbalance3 and certain foods and history-taking should assess these factors (Table 1). A family history of RAS is often evident. Typically, aphthous ulcers are round or ovoid in shape with a grey or yellow base and have a varying degree of perilesional erythema.3
Number
How many ulcers do you get at any one time?
Size
How big do they get? eg pin head, grain of rice, 5 pence piece
Site
Where in the oral mucosae do they effect?
Frequency
How often do you get the ulcers?
Duration
How long does each ulcer last for?
Ulcer-free period
How long between ulcer episodes?
Any extra-oral ulcers?
Do you get ulcers elsewhere on the body? eg genitalia, eyes, skin
Pain
Are the ulcers painful – do they effect eating, talking, etc?
Habits
Do you clench or grind your teeth? Are you aware of tongue thrusting?
Any associations
Are the ulcers associated with any particular foodstuffs? Any relation to the menstrual cycle in females? Any stresses such as links with onset of ulcers during school examination periods?
Effect on life/schooling
How do the ulcers affect you? What is their effect on eating and drinking? How much school has been missed due to oral ulcers?
Family history
Do you have any first degree relatives with oral ulceration? Any inflammatory bowel disease (Crohn's disease or ulcerative colitis) or any Coeliac disease in your family? Any other significant illnesses?
Medical history and review of systems
Enquire about any related systemic systems, especially focusing on any gastro-intestinal signs, eg abdominal pain, weight loss, blood or mucus in the stools, altered bowel habit, nocturnal defecation.
Medication history
Enquire about prescribed medication, especially anything tried so far to treat the oral ulceration and anything bought ‘Over The Counter’ (OTC) or abroad as ‘ulcer remedies’. Check compliance and correct usage technique to any medication tried so far.
There are three distinct patterns of RAS (Table 2):3
Lips, cheeks, tongue, pharynx, palate, gingivae, floor of mouth
Scarring
Uncommon
Common
Uncommon
Children affected
75–85%
10–15%
5–10%
Figure 1. Minor aphthous ulcer, left lateral border of the tongue.Figure 2. Minor aphthous ulcers, left upper labial mucosa.Figure 3. Major aphthous ulcer, left lateral border of the tongue.Figure 4. Major aphthous ulcer, right anterior pillar of the fauces.Figure 5. Herpetiform aphthous ulceration affecting lower labial mucosa and attached gingivae.Figure 6. Herpetiform aphthous ulceration affecting the ventral surface of the tongue.
Aetiology of recurrent oral ulceration in children
The various causes of oral ulceration in children are summarized in Table 3.6
Aetiology
Associated Features
Relevant Investigations
Infection
Viruses: Hand foot and mouth, Coxsackie virus, Herpes simplex, Herpes zoster, Cytomegalovirus, Epstein Barr, HIVBacteria: Tuberculosis, Syphilis
Systemic features such as fever, lethargy, weight loss, prodrome
Full blood countSwab +/- biopsyViral serology if indicated
Full blood countFolateIron/ferritinVitamin B12All to be arranged in primary care
Most common
Recurrent aphthous stomatitis is the most common and is a diagnosis of exclusion.3 Haematinic deficiencies, such as low vitamin B12, folate or ferritin and anaemia have been linked with worsening of aphthous ulceration.7,8 Traumatic ulcers are also common in children, may be recurrent and often present similarly to aphthous ulcers (Figure 7).9
Figure 7. Traumatic ulceration left lateral border of tongue related to sharp lower incisal edges.
Systemic conditions
Coeliac disease and inflammatory bowel disease, ie Crohn's disease and ulcerative colitis may be associated with aphthous-like ulcers10 and may present with various nutritional deficiencies secondary to malabsorption.11 Similar ulcers may be seen in orofacial granulomatosis, a granulomatous inflammation of the orofacial tissues, sometimes triggered by dietary exposure to cinnamon and benzoates.12 Behçet's disease, cyclic neutropenia and rare syndromes, such as MAGIC (mouth and genital ulcers with inflamed cartilage) and PFAPA (periodic fever, aphthous stomatitis, pharyngitis and cervical adenitis) are also characterized by recurrent aphthous ulcers.1
Infections
Common childhood viral illnesses (Table 3) can present as a single episode of multiple oral ulcers.9 These are self-limiting illnesses, expected to be managed in primary care without a need to refer for specialist opinion. Recovery is normally within 7–10 days.13,14
Mucocutaneous disease
Mucocutaneous conditions (Table 3), such as mucous membrane or bullous pemphigoid, pemphigus vulgaris, linear IgA disease and erythema multiforme, generally require referral to secondary or tertiary care, with occasional inpatient management required.4,15,16
Investigations
Each case should be judged individually and investigations carefully selected to confirm or refute the diagnosis as appropriate. Undertaking full blood count and haematinics is standard practice when assessing patients with suspected RAS and these can be arranged in primary care by the patient's general medical practitioner. Other investigations, such as serology for Coeliac disease or inflammatory markers (Table 4) are best arranged following referral to secondary or tertiary care.
Investigation
Healthcare Setting
Information Obtained
FBC
Primary care – general medical practice
A full blood count will give much information about whether the patient is anaemic or is suffering a clinical or subclinical infection as well as give clues as to potential haematological causes for oral ulceration
Haematinics
Primary care – general medical practice
Deficiencies in B12, folate and ferritin may cause worsening of oral ulceration
Management of RAS can be difficult and, as yet, there are no consensus guidelines on the best therapy option, as highlighted in a recent Cochrane review of systemic agents in RAS.17 There are a number of possible pharmacological agents which can be utilized in the treatment of RAS.18 Presently, there is no evidence to support the efficacy of one single agent over others. Successful management will usually employ more than one strategy at a time, individualized to each patient's needs.
Management of RAS in children should begin with education to explain the natural history of the disease and the scope of management.1,2,3,4,5 An ulcer diary can be helpful for the clinician and also allows the child to participate in his/her own management.2
Certain factors can aggravate RAS, therefore identifying these may help prevent further ulceration. Sources of trauma or parafunctional habits which may contribute to ulcer experience should be addressed, if necessary, by making a soft splint, polishing sharp teeth, coating orthodontic appliances with wax or counselling regarding tongue thrusting and bruxism.9 Exacerbation of ulcers is often noted by patients secondary to stress, such as school examinations, exposure to certain food substances, toothpaste additives and menstruation.1,18,19,20
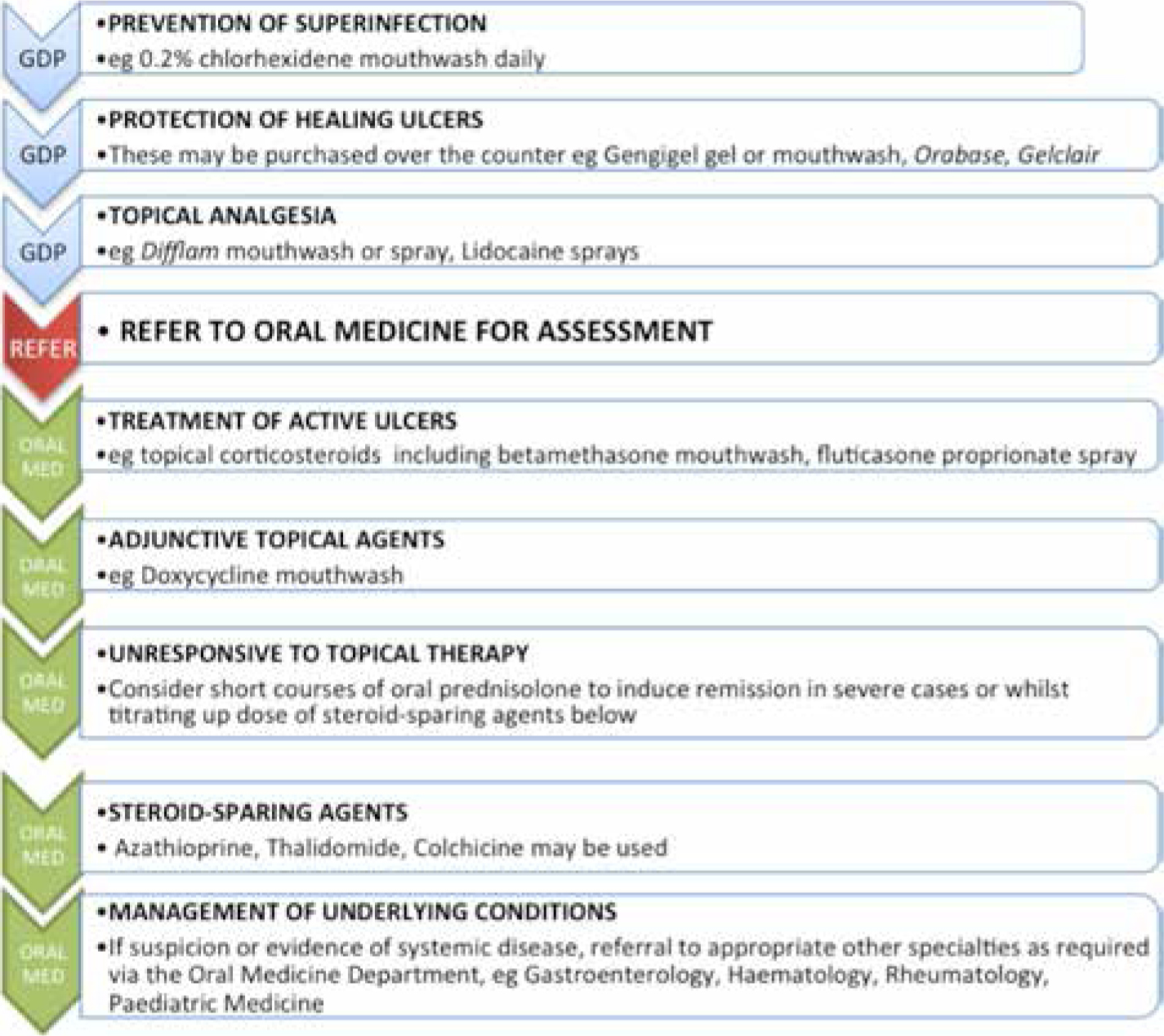
Treatment options vary (Figure 8), from the use of ‘Over The Counter’ preparations to topical and/or systemic prescribed therapies. In primary dental care, the prescription of several topical therapies is appropriate and may include antimicrobial mouthrinses, such as 0.2% chlorhexidine gluconate (Corsodyl® GlaxoSmithKline, Brentford, Middlesex), which will help with plaque control and reducing superinfection.11,21 Other useful agents include protective pastes, such as Orabase (active ingredient carmellose), Gengigel (active ingredient hyaluronate), Gelclair (active ingredient hyaluronate) and topical analgesics including 0.15% benzydamine hydrochloride (Difflam) or a 5% lidocaine spray or mouthwash useful prior to eating or toothbrushing.11,22 Advising patients to use sodium lauryl sulphate-free toothpastes may be beneficial in reducing the number of ulcers.20
Figure 8. Flow chart to guide selection of treatment of RAS in children.
Those patients with RAS severely impacting on quality of life, not responding to topical analgesics or antiseptics, or where there is a suspicion of an underlying systemic disease, should be referred to a specialist clinic or to Departments of Oral Medicine or Paediatric Dentistry. Regular and supervised use of topical corticosteroid may be introduced to reduce inflammation, promote healing and reduce the frequency of new ulcerations. Betamethasone sodium phosphate (Betnesol) 500 microgram tablets may be dissolved in water as a mouthwash.9 Another useful topical corticosteroid used is fluticasone propionate (Flixonase), which is available as a spray (50 microgram per actuation).6 It is important that the child is mature enough to use a mouthrinse correctly to avoid swallowing the solution (usually suitable for children aged 8 and above). Patients should be advised to commence topical therapy as soon as an ulcer appears or as soon as they start to feel an ulcer developing. The method of application of these topical agents depends on the number and site of the ulcers. If the patient only suffers 1 or 2 ulcers at a time, then a spray can be useful. When there are multiple ulcers at different sites, then a mouthwash is preferred. Doxycycline has been shown to decrease healing time.23 The usual preparation is to dissolve a 100 mg tablet in 10 ml of water, hold in the mouth for 3 minutes up to 4 times a day.23 It is important that only children over 12 are prescribed this owing to the adverse effects of tetracycline in the developing dentition.17,23
For severe RAS, that does not respond to topical measures alone, systemic immunosuppressants may be required. A short course of oral prednisolone may be required to gain control of the flare13 and resume normal oral intake.11 Systemic corticosteroids are not a long-term solution and the potential for stunting growth and development in a child, along with the other well-established risks, means that their use is rationalized to only when absolutely necessary.11
Steroid-sparing agents, such as Thalidomide,23 Azathioprine,24,25 or Colchicine26 may be used in severe recalcitrant cases (Figure 8). Thalidomide can be very effective and fast-acting in treating RAS. However, careful pre-treatment counselling concerning its well-established risks of teratogenicity and possible irreversible peripheral neuropathy must be discussed with the parents.1,27,28,29,30
Quality of life impacts
Episodes of oral ulceration in children have been shown to have a significant impact on various activities in daily life, including eating, speaking and toothbrushing.31,32 The overall impact of oral ulceration on these activities is reported to be similar to that of toothache.32 Despite this knowledge, there is limited evidence to identify the extent of these impacts.2
Oral ulcer diaries have been previously suggested as a successful means of recording both the incidence of oral ulceration and the impact on quality of life.2 Use of a diary enables accurate and contemporaneous recording of events between appointments and reduces the need for reliance on the child's and parent's memory.33 This information allows the clinician to tailor a management programme to meet the individual's needs more effectively. In addition to refining clinical management, it supports recognition of the impact of the condition on the patient's quality of life and prompts provision of suitable emotional support and reassurance. This has, in itself, been shown to be valued by children and can help improve patient perception of the ‘process of care’.33,34
Conclusion
Recurrent aphthous stomatitis is a common condition general dental practitioners will see regularly in their young patients. Simple topical measures can be employed before referral to secondary care for assessment and management. Better understanding of a patient's symptoms will support a more individualized management plan with the aim to improve quality of life. Paediatric oral medicine teams have a role in investigating patients with RAS and providing topical and systemic pharmacological management, as appropriate.