Antunes JLF, Toporcov TN, Biazevic MGH, Boing AF, Scully C, Petti S. Alcohol drinking effect and oral cancer: independent or joint effect with smoking? Large case-control study. Public Library Of Science (PLoS One). 2013; 8:(7) https://doi.org/10.1371/journal.pone.0068132
Boffetta P, Hecht S, Gray N Smokeless tobacco and cancer. Lancet Oncol. 2008; 9:(7)667-675
Conway DI, Hashibe M, Boffetta P, Wunsch-Filho V, Muscat J, La Vecchia C, Winn DM. Enhancing epidemiologic research on head and neck cancer: INHANCE – The International Head and Neck Cancer Epidemiology consortium. Oral Oncol. 2009; 45:(9)743-746 https://doi.org/10.1016/j.oraloncology.2009.02.007
Delnevo CD, Pevzner ES, Hrywna M, Lewis MJ. Bidi cigarette use among young adults in 15 states. Prevent Med. 2004; 39:207-211
Ferreira Antunes JL, Toporcov TN, Biazevic MG, Boing AF, Scully C, Petti S. Joint and independent effects of alcohol drinking and tobacco smoking on oral cancer: a large case-control study. PLoS One. 2013; 8:(7) https://doi.org/10.1371/journal.pone.0068132
Gandini S, Botteri E, Iodice S Tobacco smoking and cancer: a meta-analysis. Int J Cancer. 2008; 122:(1)155-164
Hassonah Y, Scully C. Dokha: an emerging smoking habit with possible oral effects. Oral Dis. 2015; https://doi.org/10.1111/odi.12324
Lee YC, Marron M, Benhamou S Active and involuntary tobacco smoking and upper aerodigestive tract cancer risks in a multicenter case-control study. Cancer Epidemiol Biomarkers Prev. 2009; 18:(12)3353-3361
Lin WJ, Jiang RS, Wu SH Smoking, alcohol, and betel quid and oral cancer: a prospective cohort study. J Oncol. 2011; 2011
Malson JL, Lee EM, Murty R, Moolchan ET, Pickworth WB. Clove cigarette smoking: biochemical, physiological, and subjective effects. Pharmacol Biochem Behav. 2003; 74:739-745
Marron M, Boffetta P, Zhang ZF Cessation of alcohol drinking, tobacco smoking and the reversal of head and neck cancer risk. Int J Epidemiol. 2010; 39:(1)182-196
Parkin DM, Boyd L, Walker LC. 16. The fraction of cancer attributable to lifestyle and environmental factors in the UK in 2010. Br J Cancer. 2011; 105:(S2)S77-S81
Parkin DM. Tobacco-attributable cancer burden in the UK in 2010. Br J Cancer. 2011; 105:(S2)S6-S13
Petti S, Masood M, Messano GA, Scully C. Alcohol is not a risk factor for oral cancer in nonsmoking, betel quid non-chewing individuals. A meta-analysis update. Annls Hyg. 2013; 25:(1)3-14 https://doi.org/10.7416/ai.2013.1901
Petti S, Scully C. Determinants of oral cancer at the national level: just a question of smoking and alcohol drinking prevalence?. Odontology. 2010; 98:144-152
Hassona Y, Scully C, Abu Ghosh M, Khoury Z, Jarrar S, Sawair F. Mouth cancer awareness and beliefs among dental patients. Int Dent J. 2014; https://doi.org/10.1111/idj.12140
Rahman M, Fukui T. Bidi smoking and health. Public Hlth. 2000; 114:123-127
Rahman M, Sakamoto J, Fukui T. Bidi smoking and oral cancer: a meta-analysis. Int J Cancer. 2003; 106:600-604
Scully C, Petti S. Overview of cancer for the healthcare team; aetiopathogenesis and early diagnosis. Oral Oncol. 2010; 46:402-406
Shah SB, Chestnutt IG, Lewis MAO. ‘Hubble-bubble leads to trouble’ – waterpipe smoking and oral health. Dent Update. 2013; 40:800-804
Warnakulasuriya S, Scully C. Cancer of the mouth for the dental team; comprehending the condition, causes, controversies, control and consequences: 2. Main risk factors and epidemiology. Dent Update. 2010; 37:710-712
Watson CH, Polzin GM, Calafat AM, Ashley DL. Determination of the tar, nicotine, and carbon monoxide yields in the smoke of bidi cigarettes. Nicot Tobac Res. 2003; 5:(5)747-753
Geneva: World Health Organization; 2006
Wyss A, Hashibe M, Chuang SC, Lee YC, Zhang ZF, Yu GP Cigarette, cigar, and pipe smoking and the risk of head and neck cancers: pooled analysis in the International Head and Neck Cancer Epidemiology Consortium. Am J Epidemiol. 2013; 178:(5)679-690 https://doi.org/10.1093/aje/kwt029
Yen KL, Hechavarria E, Bostwick SB. Bidi cigarettes: an emerging threat to adolescent health. Archiv Pediatr Adolesc Med. 2000; 154:1187-1189
Znaor A, Brennan P, Gajalakshmi V Independent and combined effects of tobacco smoking, chewing and alcohol drinking on the risk of oral, pharyngeal and esophageal cancers in Indian men. Int J Cancer. 2003; 105:(5)681-686
A MEDLINE search early in 2015 revealed more than 250,000 papers on head and neck cancer; over 100,000 on oral cancer; and over 60,000 on mouth cancer. Not all publications contain robust evidence. We endeavour to encapsulate the most important of the latest information and advances now employed in practice, in a form comprehensible to healthcare workers, patients and their carers. This series offers the primary care dental team, in particular, an overview of the aetiopathogenesis, prevention, diagnosis and multidisciplinary care of mouth cancer, the functional and psychosocial implications, and minimization of the impact on the quality of life of patient and family.
CPD/Clinical Relevance: This article offers the dental team an overview of the main cancer risk factors, tobacco and alcohol, betel and other chewing habits, and environmental factors.
Article
Nicholas Kalavrezos Professor Crispian Scully
Mouth cancer arises out of DNA mutations (Article 1) which can affect various genes and are increased by various risk factors. The main known definitive risk factors for mouth cancer are using tobacco and drinking alcohol: it is thought that about 3 out of 4 head and neck cancers (75%) are linked to these habits (Figure 1). Other risk factors include betel use and similar chewing habits (Article 4). Radiation (eg sunlight, ionizing), which is implicated in lip cancer, and infection with the virus human papillomavirus (HPV), which plays a role in oropharyngeal cancer, are discussed in Article 5. This article discusses tobacco.
Figure 1. Cigarettes smoked by one person in an hour.
What are traditional cancer risk factors?
The cause of cancer in most people is unclear but risk depends on a combination of genes, environment and aspects of living (Figure 2).
Figure 2. Cancer is mainly related to lifestyle factors (acknowledgement to Warnakulasuriya S, Scully C. Cancer of the mouth for the dental team; comprehending the condition, causes, controversies, control and consequences: 2. Main risk factors and epidemiology. Dent Update 2010; 37: 710–712).
Anything that increases DNA mutations increases a person's chances of developing cancer and is called a ‘cancer risk factor’. A risk factor is something that increases the chances of developing cancer, but having a risk factor for cancer does not mean necessarily that cancer will develop: some people with risk factors never develop cancer, and yet other people without known risk factors can still develop cancer. It is impossible to control fundamental mouth cancer risk factors such as gender and age.
However, many factors can be controlled – modifiable risk factors – and many of these relate to the lifestyle chosen. Some risk factors are definitive and others are only possible risk factors. Tobacco and alcohol contain nitrosamines and other chemicals known to cause cancer. There appear to be two distinct pathways to mouth cancer – most cancers are related to tobacco or alcohol or betel, but some are related to HPV infection.
What are the traditional risk factors for mouth cancer?
The International Agency for Research on Cancer (IARC) and the World Cancer Research Fund/American Institute for Cancer Research (WCRF/AICR) are the gold standard in cancer epidemiology, and their conclusions about mouth cancer risk factors are shown in Table 1.
Increases risk (‘sufficient’ or ‘convincing’ evidence)
May increase risk (‘limited’ or ‘probable’ evidence)
May decrease risk (‘limited’ or ‘probable’ evidence)
Alcoholic beverages (oral, tonsil, pharynx)Betel quid with tobacco (oral, tonsil, pharynx)Betel quid without tobacco (oral)Human papillomavirus type 16 (oral, tonsil, pharynx)Tobacco, smokeless (oral)Tobacco smoking (oral, tonsil, pharynx, nasopharynx)X-radiation, gamma-radiation (salivary gland)Epstein-Barr virus (nasopharynx)Formaldehyde (nasopharynx)Salted fish, Chinese-style (nasopharynx)Wood dust (nasopharynx)
Solar radiation (lip)Human papillomavirus type 18 (oral, cavity)Radioiodines, including Iodine-131 (salivary gland)Asbestos (pharynx)*Mate, hot (pharynx)Printing processes (pharynx)Tobacco smoke, secondhand (pharynx)Hydrochlorothiazide (lip)
Non-starchy vegetables (not salted or pickled) (mouth, pharynx and larynx)Fruits (not salted or pickled) (mouth, pharynx and larynx)Foods containing carotenoids (mouth, pharynx and larynx)
*A traditional South American caffeine-rich drink.
What are the known modifiable risk factors for mouth cancer?
Most of the lifestyle (modifiable) cancer risk factors:
Are addictive – some are regarded as ‘legal highs’ – which is why they are so popular;
Affect other body systems and can cause other health problems;
Are often multiple habits;
Have often spread by migration.
The main modifiable risk factors are:
Habits;
– Tobacco use
– Betel use
Alcoholic beverage use;
Diet poor in fresh fruit and vegetables;
In the case of lip carcinoma, exposure to sunlight;
In the case of oropharyngeal carcinoma, exposure to HPV.
Tobacco
Tobacco is derived from plants Nicotinia tabacum and Nicotinia rustica of the genus Nicotiniana. It releases nicotine, (S)-3-(1-methyl-2-pyrrolidinyl) pyridine (Figure 3), the most abundant of the volatile alkaloids in the leaf. Nicotine is one of the most heavily used and highly addictive stimulant drugs. It acts on nicotinic cholinergic receptors, affects most organ systems and binds to a CNS receptor and, like cocaine, heroin and marijuana, raises the level of brain dopamine, as well as opioids and glucose, and activates the nucleus accumbens. The type of nicotine cholinergic receptor and the enzyme CYP2A6 (cytochrome P – a terminal oxidase enzyme) influence the chances of addiction. Nicotine also causes a discharge of adrenaline from the adrenals, which stimulates the CNS, and other endocrine glands, and a sudden release of glucose.
Figure 3. Nicotine formula.
Nicotine is absorbed readily from tobacco smoke in the lungs, acting in seconds on the brain, but affects the body for up to 30 min. Stimulation is followed by depression and fatigue, leading the abuser to seek more nicotine. If a person tries to stop smoking, withdrawal symptoms may appear with excessive anger, hostility and aggression.
Tobacco use also generates several carcinogens (cancer-causing chemicals) from the leaf, and most relevant for mouth cancer are the tobacco-specific nitrosamines (TSNAs) from manufactured tobacco, as well as:
PAH [Polycyclic aromatic hydrocarbons, eg benzene and aromatic amines];
Aromatic amines;
Heavy metals.
Tobacco contains over 60 carcinogens! Also, the production of free radicals results in alterations in various antioxidant enzymes (glutathione-S-transferase (GST), glutathione reductase, superoxide dismutase, catalase and glutathione peroxidase).
Cigarettes
Smoking tobacco products like cigarettes increases the risk of oral cancer. All forms of tobacco, both smoked and smokeless, are carcinogenic. There is for mouth cancer:
A 20-fold higher risk in heavy smokers (dark tobacco is worst);
A strong dose-response relationship.
Tobacco also predisposes to:
Cancers of the larynx, pharynx, lung, oesophagus, stomach, colon, liver, and breast;
Other diseases (eg heart diseases, bronchitis).
Use of tobacco puts the user at a higher than average risk of developing these cancers.
IARC classifies tobacco smoking as a cause of mouth, tonsil, pharynx and nasopharynx cancers. Smoking tobacco may cause 70% of mouth and pharyngeal cancers in men, and around 55% in women, in the UK. A meta-analysis showed that current smokers have a three-fold increased risk of mouth cancer, compared with people who have never smoked and nearly seven times the risk of pharyngeal cancer. The more cigarettes someone smokes, and the more years they smoke for, the higher the risk of mouth cancer. Compared with people who do not smoke, the risk of mouth cancer in those who smoke low/medium-tar cigarettes and high-tar cigarettes was 8.5- and 16.4-fold greater, respectively. (Note that cigarettes are classified as low/medium if the tar yield is less than 22 mg and high tar if the tar yield is greater than 22 mg).
Smoking cessation, however, leads to a fall in mouth cancer risk; by 1–4 years after smoking cessation the risk of mouth cancer is 35% lower than that of a current smoker, and by 20 years or more after cessation the risk is reduced to that of a never-smoker. The risk of oropharynx/hypopharynx cancer risk reduces by around half by 5–9 years of smoking cessation, and is almost that of a never-smoker by 20 years.
Tobacco consumption has dropped in the UK probably owing to the increased cost of a packet of cigarettes, as well as the ban on smoking in public buildings and vehicles (buses/trains/planes). On the other hand, self-rolled cigarettes, which have a higher carcinogen content, are also now more popular.
Bidis and kreteks
Bidis are small, thin, hand-rolled cigarettes from south Asia, which comprise tobacco wrapped in a tendu or temburni leaf. Kreteks – sometimes called clove cigarettes – are from Indonesia and typically contain a mixture of tobacco, cloves and other additives. Both bidis and kreteks have higher concentrations of nicotine, tar and carbon monoxide than conventional cigarettes and have at least comparable adverse health effects. People who smoke bidi have around three times the risk of mouth cancer compared with bidi never-smokers.
Cigars and pipes
People who have only smoked pipes or cigars, rather than cigarettes, also have an increased risk of mouth, pharynx and larynx cancers. People who smoke only cigars increase their risk by three-and-a-half times, and those who smoke only a pipe increase their risk by nearly four times. Pipe smokers or people who hold the cigarette for a long time on the lip have an increased risk of lip cancer.
Tobacco is also a major hazard to health and promotes many diseases, particularly heart disease, lung disease and cancers of the lung, oesophagus, mouth and bladder (Tables 2, 3 and Figure 4).
System
Possible effects
Bladder
Cancer
Cardiovascular
Ischaemic heart disease. If women smokers also take oral contraceptives, they are more prone to cardiovascular and cerebrovascular diseases than are other smokers
Women who smoke generally have earlier menopausePregnant women who smoke cigarettes run a greater risk of having still-born or premature infants or infants with low birth weight
Indeed, tobacco smoking is the largest avoidable cause of death and serious disability in the UK and most other developed countries. In the UK, around one in five adults, or about ten million people, are current smokers, five million of whom are expected to die prematurely from the habit. Smoking currently accounts for around 100,000, or about one in six, deaths each year in the UK.
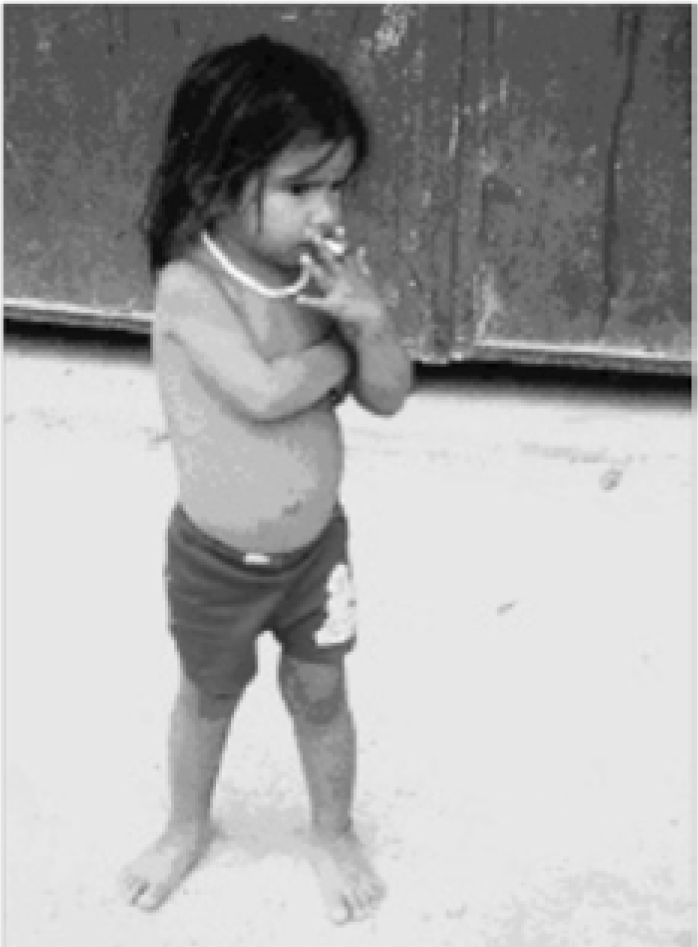
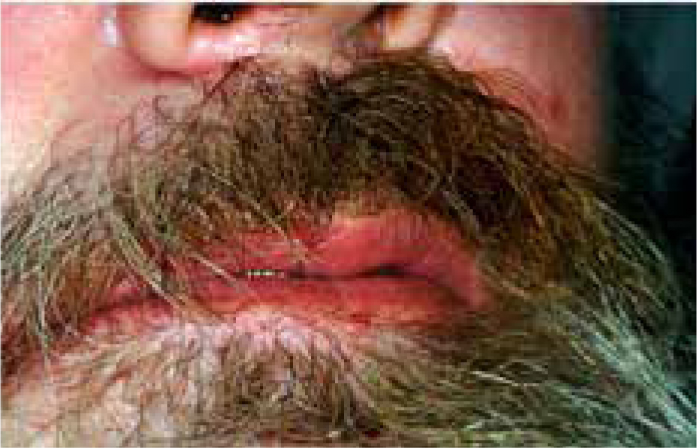
Smoking is strongly associated with socioeconomic disadvantage and, in most high income countries, the prevalence of smoking is considerably higher among more deprived people than in those from affluent backgrounds. In the UK, the unemployed are twice as likely to be smokers compared to employed people and smoking is highly prevalent among the homeless, those in custodial care and other marginalized or disadvantaged groups. Smoking is also more than twice as prevalent among people with mental health issues. Smokers in disadvantaged groups also typically start at a younger age (Figure 5), and they smoke more cigarettes per day (Figures 6, 7, 8 and 9), and take in more nicotine from each cigarette. Smoking thus strongly exacerbates health inequalities.
Figure 5. Brazilian child smoking.Figure 6. Skin staining from heavy cigarette smoking.Figure 7. Staining of moustache and beard from cigarette smoking.Figure 8. Tooth staining and lip leukoplakia in heavy smoker.Figure 9. Stomatitis nicotina.
Environmental (second hand) tobacco smoke (ETS)
Passive smoking can cause lung cancer, increases the risk of respiratory illnesses and may cause sudden infant death. Exposure to second-hand smoke also causes lower respiratory infections, asthma and wheezing illness, meningitis and middle ear disease. Smoking in pregnancy harms the foetus, increasing the risk of premature birth, low birth weight, foetal anomalies, and foetal mortality.
People exposed to secondhand smoke at home or in the workplace have a small increase in their risk of mouth or oropharyngeal cancer. Never-smokers who have ever been exposed to ETS at home or work have an 87% higher risk, and those exposed in this way for 15 years or more have more than double the risk.
Waterpipes
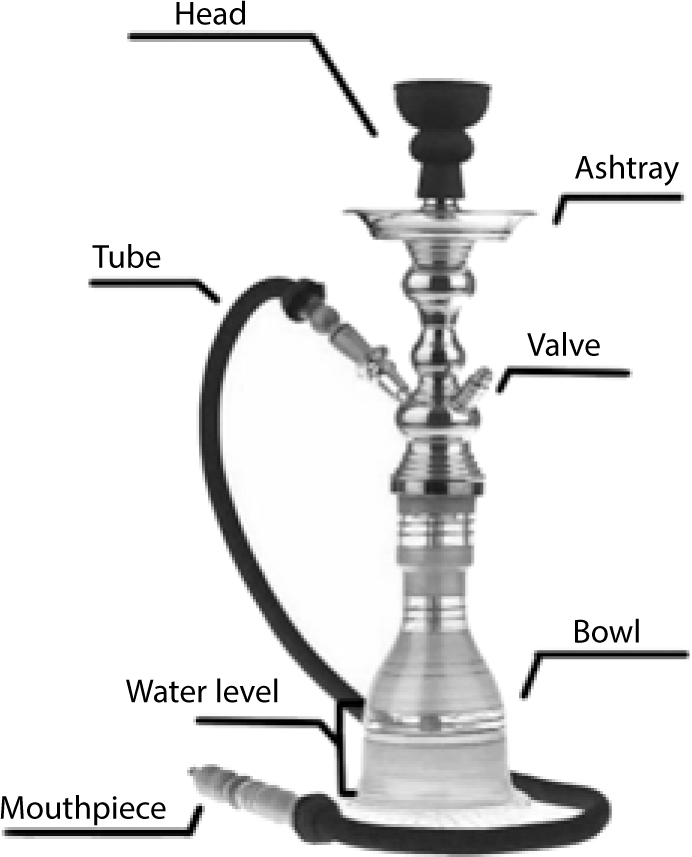
A frequent habit that emanated particularly in the Levant (the geographic and cultural region consisting of the eastern Mediterranean littoral between Anatolia and Egypt) and can now be seen worldwide, is of smoking tobacco in a waterpipe (Figure 10). A waterpipe is known by a variety of names (arghila, argileh, boory, goza, hookah, hubble bubble, narghile, nargile, nargila, narjeela, mada'a orarghile, shisha and qalyān).
Figure 10. A waterpipe.
Waterpipes contain tobacco flavoured with molasses in a mixture termed either tobamel (from tobacco plus ‘mel’ for ‘honey’ in Latin) or mu'essel (‘honeyed’ in Arabic). The flavoured tobacco is indirectly heated by burning embers or charcoal, and waterpipe users are exposed to similar nicotine levels as are tobacco cigarette smokers, but with higher levels of carbon monoxide, and they have carboxyhaemoglobin levels in their blood.
Waterpipe smoking is as harmful to health as is cigarette smoking. The harm relates to inhalation of tobacco smoke and also carbon monoxide. Second-hand smoke from waterpipes is a mixture of tobacco smoke in addition to the smoke from the fuel and therefore poses a risk for non-smokers.
Sharing a waterpipe mouthpiece is common and may pose other hazards, such as risk of communicable disease transmission, including tuberculosis and viral hepatitis. Local Government Regulation in England has issued supplementary guidance to regulatory officers on the enforcement of a smoking ban in ‘shisha bars’ (Figure 11).
Figure 11. A shisha bar in the UK.
Smokeless tobacco
There is a range of smokeless tobacco products, including:
Chewing tobacco;
Snuff – powdered tobacco designed to be snorted;
Snus – a type of smokeless tobacco popular in Sweden, which is placed under the upper lip.
Such more ‘sanitized’ forms of smokeless tobacco available in parts of Europe and the USA are carcinogenic despite claims to the contrary.
Smokeless tobacco is of two main types: chewing tobacco and snus (Figure 12). Both these types are addictive and can cause health problems. The ingredients are a variety of tobacco, sugar, salt, slaked lime, spices and flavourings. Chewing tobacco usually comes as leaves or plugs which release nicotine and flavours. Snus comes as a moist powder, or packed in small bags, which are put in the lower labial sulcus, inside the lower lip, where it may cause white lesions (snuff-dippers keratosis).
Figure 12. Smokeless tobacco.
Smokeless tobacco is used mainly by people from South Asia, South East Asia, the Middle East and East Africa and has many different names, including:
Ariva;
Chaw;
Chimo;
Chun;
Dohka;
Khaini;
lq'mik;
Manikchand;
Mawa;
Mishri, Mosheri or Misheri;
Nass, Naswat, Naswar or Niswar;
Paan Masala (Gutkha);
Qiwam or Kima;
Shammah;
Snuff;
Snus;
Supari;
Toombak;
Tulsi;
Zarda.
In the UK and Europe (except for Sweden), smokeless tobacco is rarely used except in minority ethnic groups. The cancer risk of smokeless tobacco seems to vary by geographical location, probably due to differences in the composition and format (eg chewing or inhaling nasally). Tobacco chewing in people from parts of Asia appears to predispose to mouth cancer, particularly when it is started early in life and is used frequently and for prolonged periods. The IARC classifies smokeless tobacco as a cause of mouth cancer. Risk of mouth cancer is increased five-fold in India and other Asian countries, and seven-fold in Sudan, doubled among smokeless tobacco users in the United States and Canada, but in the Nordic countries there appears to be no such increase.
One of the most dangerous and popular uses of smokeless tobacco is with areca (or betel) nut used in ‘betel quid’ made up of betel leaf, areca nut and slaked lime (Article 4).
Conclusion
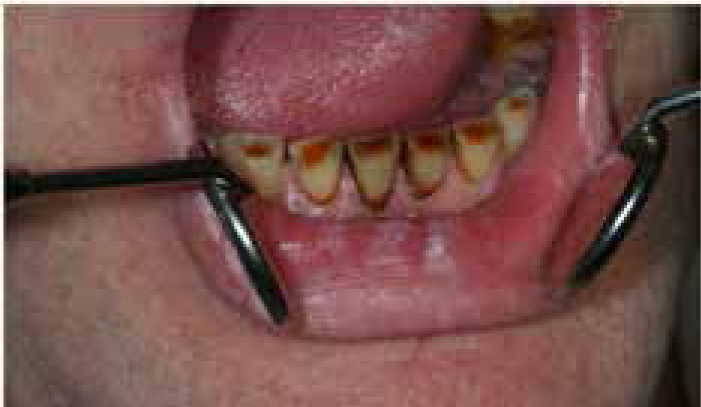
In addition to the risk of damage to oral health already discussed, tobacco users are also more likely to have gingival recession and caries.