Alani A, Owens J, Dewan K, Summerwill A. A national survey of oral and maxillofacial surgeons' attitudes towards the treatment and dental rehabilitation of oral cancer patients. Br Dent J. 2009; 207:540-541
Aramany MA. A history of prosthetic management of cleft palate: Pare to Suersen. Cleft Palate J. 1971; 8:415-430
Aramany MA. Basic principles of obturator design for partially edentulous patients. Part I: Classification. J Prosthet Dent. 2001; 86:559-561
Brown JS, Shaw RJ. Reconstruction of the maxilla and midface: introducing a new classification. Lancet Oncol. 2010; 11:1001-1008
Parr GR, Tharp GE, Rahn AO. Prosthodontic principles in the framework design of maxillary obturator prostheses. J Prosthet Dent. 2005; 93:405-411
Aramany MA. Basic principles of obturator design for partially edentulous patients. Part II: Design principles. J Prosthet Dent. 2001; 86:562-568
Devlin H, Barker GR. Prosthetic rehabilitation of the edentulous patient requiring a partial maxillectomy. J Prosthet Dent. 1992; 67:223-227
Kornblith AB, Zlotolow IM, Gooen J, Huryn JM, Lerner T, Strong EW Quality of life of maxillectomy patients using an obturator prosthesis. Head Neck J Sci Specialties Head Neck. 1996; 18:323-334
Sharma AB, Beumer J. Reconstruction of maxillary defects: the case for prosthetic rehabilitation. J Oral Maxillofac Surg. 2005; 63:1770-1773
Walter J. Obturators for acquired palatal defects. Dent Update. 2005; 32:277-284
Irish J, Sandhu N, Simpson C, Wood R, Gilbert R, Gullane P Quality of life in patients with maxillectomy prostheses. Head Neck J Sci Specialties Head Neck. 2009; 31:813-821
Nadeau J. Maxillofacial prosthesis with magnetic stabilizers. J Prosthet Dent. 1956; 6:114-119
Beumer III, Curtis TA, Marunick MT.St Louis, Toronto, London: The CV Mosby Co; 1979
Rehabilitation of oncology patients with hard palate defects part 2: principles of obturator design Rahat Ali Asmaa Altaie Brian Nattress Dental Update 2024 42:5, 707-709.
The first part of this series on the conventional rehabilitation of oncology patients with hard palate defects discussed the dental challenges posed by oncology patients and the surgical/restorative planning interface for conventional dental rehabilitation. This article will describe Aramany's classification of hard palate defects, Brown's classification of palatal defects and focus on the basic principles of obturator design which need to be appreciated when prosthetically rehabilitating a patient with a hard palate defect.
CPD/Clinical Relevance: A good understanding of basic removable prosthodontic theory relating to denture design, dental materials science and head and neck anatomy is a prerequisite when designing an obturator for a patient.
Article
Resecting a palatal tumour will result in a surgical defect. The resulting defect can be managed by primary surgical closure, reconstruction with a surgical flap or prosthetic obturation. The decision as to which modality of treatment is chosen should be made within an oncology multidisciplinary team with input from surgeons, clinical oncologists, radiologists and restorative dentists.1 With modern surgical techniques, it is encouraging to see that more surgeons are offering reconstructions for head and neck oncology patients post resection.
The use of microvascular flaps to reconstruct head and neck cancer patients has increased over the years, with deep circumflex iliac artery (DCIA) and radial forearm free flaps (RFFF) being used to reconstruct maxillary defects.2 It is encouraging to see that the use of dental implants to rehabilitate oral cancer patients has also increased since 1995.2 There is, however, a cohort of patients who have not been reconstructed and may be unsuitable for, or may not be interested in, implant-based rehabilitation. Such patients with acquired hard palate defects will need conventional dental rehabilitation with an obturator. For these patients, the obturator will help to separate the oral and nasal cavities, help to restore normal speech and swallowing and provide support for the lip and cheek.
This article is the second paper in a series of three. It will focus on the conventional, non-implant based prosthetic obturation of oncology patients with surgically acquired hard palate defects. It will describe Aramany's classification of hard palate defects, Brown's classification of palatal defects and focus on the basic principles of obturator design.
Principles of obturator design
Defects have been successfully managed with obturators (Latin: ‘obturare’ meaning ‘to block up’) for many years. Ambroise Pare was probably the first individual to close a palatal defect artificially in the 1500s.3 The early obturators were used primarily to close congenital defects as opposed to acquired defects. The pioneering works of these prosthodontists set the foundation for the current generation of maxillofacial prosthodontists.
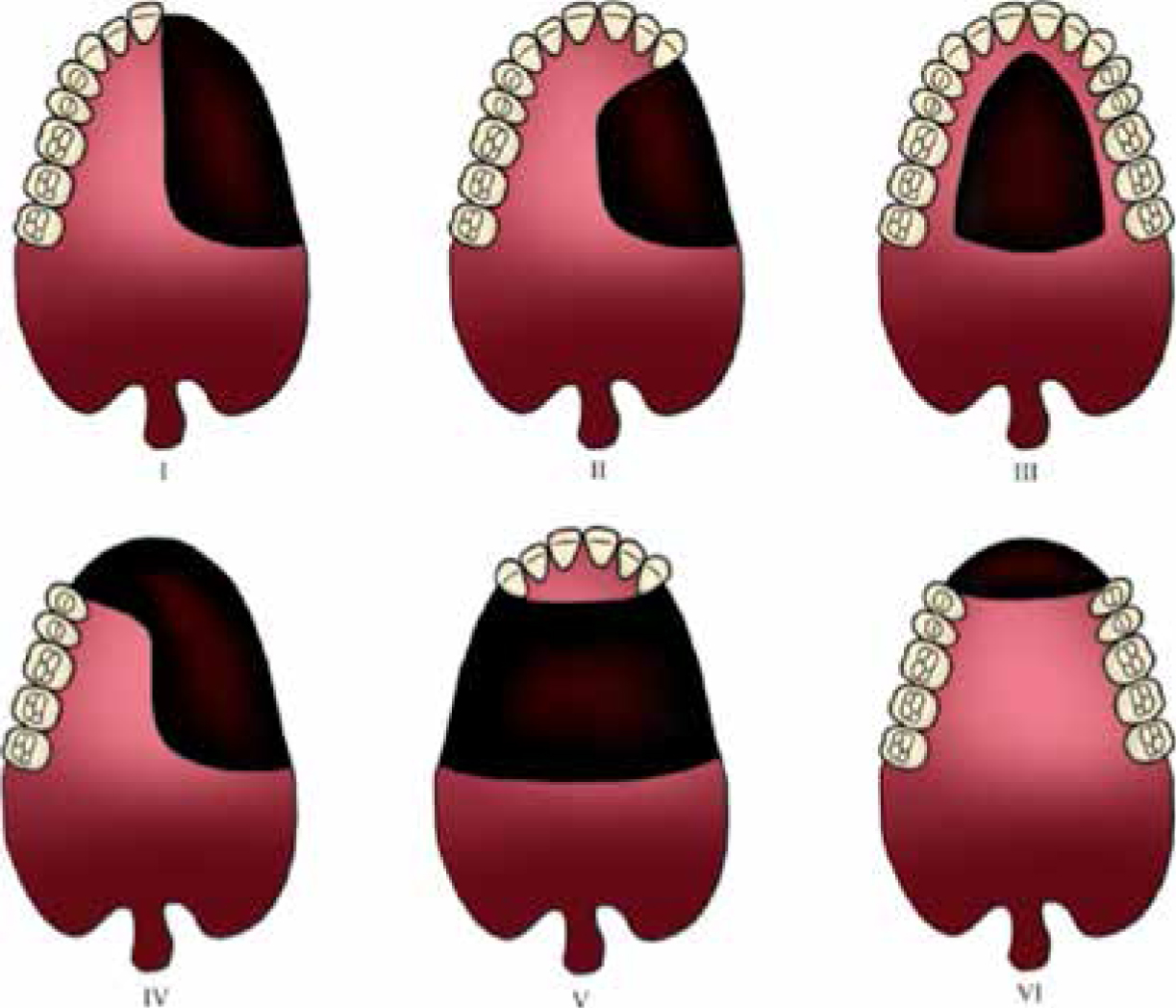
Aramany classified partially dentate maxillectomy patients into six groups.4 This classification is based on the relationship of the defect to the remaining abutment teeth and represents a systematic means of describing maxillectomy patients and potentially framework designs for an obturator (Figure 1). Although it is a very useful classification, it only considers the defect in the horizontal plane and gives no indication of the extent of the defect in the vertical axis.
Figure 1. Aramany's classification of maxillectomy defects. Class I = midline resection; Class II = unilateral resection; Class III = central resection; Class IV = bilateral anterior-posterior resection; Class V = posterior resection and Class VI = anterior resection.
Brown and co-workers suggested a modified classification of maxillary defects.5 It describes the defect in both the vertical and horizontal planes for both dentate and edentulous maxillectomy patients. The vertical classification is as follows:
Class 1: Maxillectomy without an oral/antral communication;
Class 2: Low level maxillectomy not involving the orbital floor or contents;
Class 3: High level maxillectomy involving the orbital contents;
Class 4: Radical maxillectomy involving orbital exenteration.
The horizontal component of the defect is classified as:
a: Palatal defect only, sparing the alveolus;
b: Less than or equal to half the maxilla, unilateral maxillectomy;
c: Less than or equal to half bilateral or transverse anterior defect;
d: Greater than half maxillectomy.
For any removable prosthesis to be successful, it must be retentive, stable and have good support. These prosthetic principles are especially applicable to an obturator.
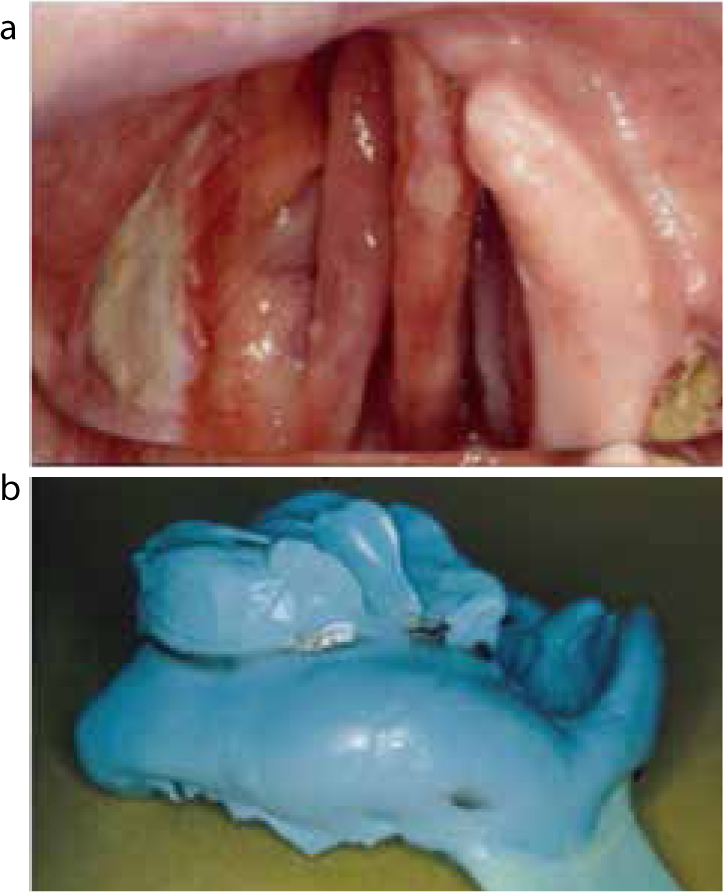
Support can be defined as the resistance to movement of a prosthesis towards the underlying tissue. For an obturator, support can be derived from the residual hard palate, alveolar ridge, the remaining teeth and from within the defect itself. According to the recommendations of Desjardins,6 a flat-vaulted hard palate and a broad ridge are better adapted to provide support than a high tapering palate and a narrow tapering alveolar ridge. To maximize support for the patient's new denture, maximum palatal coverage of the hard palate should be employed (Figure 2). If the remaining teeth are to be used to provide support, they should be loaded with rest seats and used in sufficient numbers to minimize movement of the prosthesis towards the underlying mucosa. They should be located as close to the defect as possible and not place excessive torque on the teeth6 (Figure 2c, d). Given the demands that will be placed on the abutment teeth to provide adequate support, they should be periodontally sound.
Figure 2.
(a, b) A palatal defect that was obturated with an acrylic obturator. To minimize any torquing forces on the UR6, a flexible wrought gold clasp was used. (c, d) A patient with an extensive defect where a swing-long prosthesis was provided. Note the use of multiple cast clasps and rests, the extension of the metal connector on to the UL3 for support/indirect retention and maximal palatal coverage.
The presence of the defect allows structures within it to be used to obtain support for the prosthesis. This support can be achieved by contact of the prosthesis with any anatomical structure that provides a firm base, and includes the floor of the orbit, pterygoid plate and nasal septum.6 Using the orbital floor increases the vertical height of the appliance and can create difficulties with insertion and removal. Care must also be taken to avoid pressure on the sensitive turbinate nasal bones. The nasal septum is also not ideal to provide support as it is partly cartilage and has very little surface area that can be utilized. The most commonplace to use for support (within the defect) is the pterygoid plate. Positive contact on to the plate can act like a tripod and stabilize the device, minimizing its rotation into the defect.
Retention of a prosthesis refers to its resistance to vertical displacement. As with support, retention can be gained from the residual maxillary structure, or anatomical structures within the defect. Implants within the residual alveolar ridge, the surgical defect or the zygomatic bones can also be used to help retain the obturator. Any remaining teeth can be an asset for retaining the prosthesis as they can be engaged (with clasps). Movement of the obturator may generate tremendous torquing forces, which in turn will be dissipated by the retaining abutment teeth. It is recommended that, to maximize direct retention, clasps are located as close to and as far from the defect, with at least one clasp in between these two extreme points.6 The preparation of guide planes to produce one single path of insertion can also aid in retention.7 If the abutment teeth have good bony support and no signs of active periodontitis, a cast clasp and rest seat can be prescribed to augment retention and support for the prosthesis (Figure 2c, d). For Aramany Class IV defects, retention can be maximized by placing retentive clasp arms on the remaining premolar and molar teeth, if they are periodontally sound and have adequate root support.8 For Class Aramany II defects, clasps can be prescribed for the anterior and posterior teeth.7 If the teeth have a guarded long-term prognosis, wrought gold or stainless steel clasps should be used to minimize torquing forces on the abutments (Figure 2a, b).
Retention can also be obtained from the defect itself. Naturally occurring undercuts within the residual hard/soft palate can be engaged by the prosthesis to augment retention. Extension of the obturator into the area superior to the lateral scar band, created by the use of a split skin graft at the time of surgery, provides an ideal undercut to aid retention of the appliance (Figure 3). Extension of the obturator on to the nasopharyngeal surface of the soft palate will also improve retention.9 Therefore, at the surgical planning stage, it is imperative that the surgeon tries to preserve as much palatal tissue as possible, without compromising resection of the tumour. Patient satisfaction with an obturator will significantly decrease if more than one quarter of the hard palate or one third of the soft palate is resected.10
Figure 3.
(a, b) A patient where a split thickness skin graft was prescribed for the lateral aspect of the resection. It formed an undercut that was recorded on the master impression and engaged by the obturator.
So far, the concept of retention has been discussed with respect to vertical displacement of the appliance. An obturator is unique in that it can also rotate out of the defect due to the force of gravity and function. It is difficult to eliminate this and patients may use adhesive to prevent the obturator from dislodging. To minimize this, indirect retention can be incorporated into the prosthesis by extending the connector beyond the axis of rotation on to any residual teeth that are present, assuming that they are periodontally sound. For Class II Aramany defects, this could involve extending the metal framework/indirect retainer on to the opposite side of the defect and on to the remaining canine and premolar teeth.8
Stability refers to the resistance to dislodgement by functional forces. If an obturator is designed to gain optimal support and retention from the remaining tissues (eg maximal lateral extension into the defect/extension of the bracing components on to the abutment teeth), the need for stability will also be appeased. In particular, Sharma and Beumer discussed the need to extend the bung up the lateral wall of the defect maximally to improve retention, stability and provide support for the lip and cheek.11 Desjardins has further recommended that the posterior part of the obturator is lower (in height) than the anterior portion. This design feature will encourage downward movement of any fluid into the nasopharynx.6
There are essentially two principal styles of obturator:
The fully extended hollow bulb (usually rigid); and
The open top which may be designed with either a rigid or flexible rim.12
The use of either design is dictated by the requirements of individual cases.
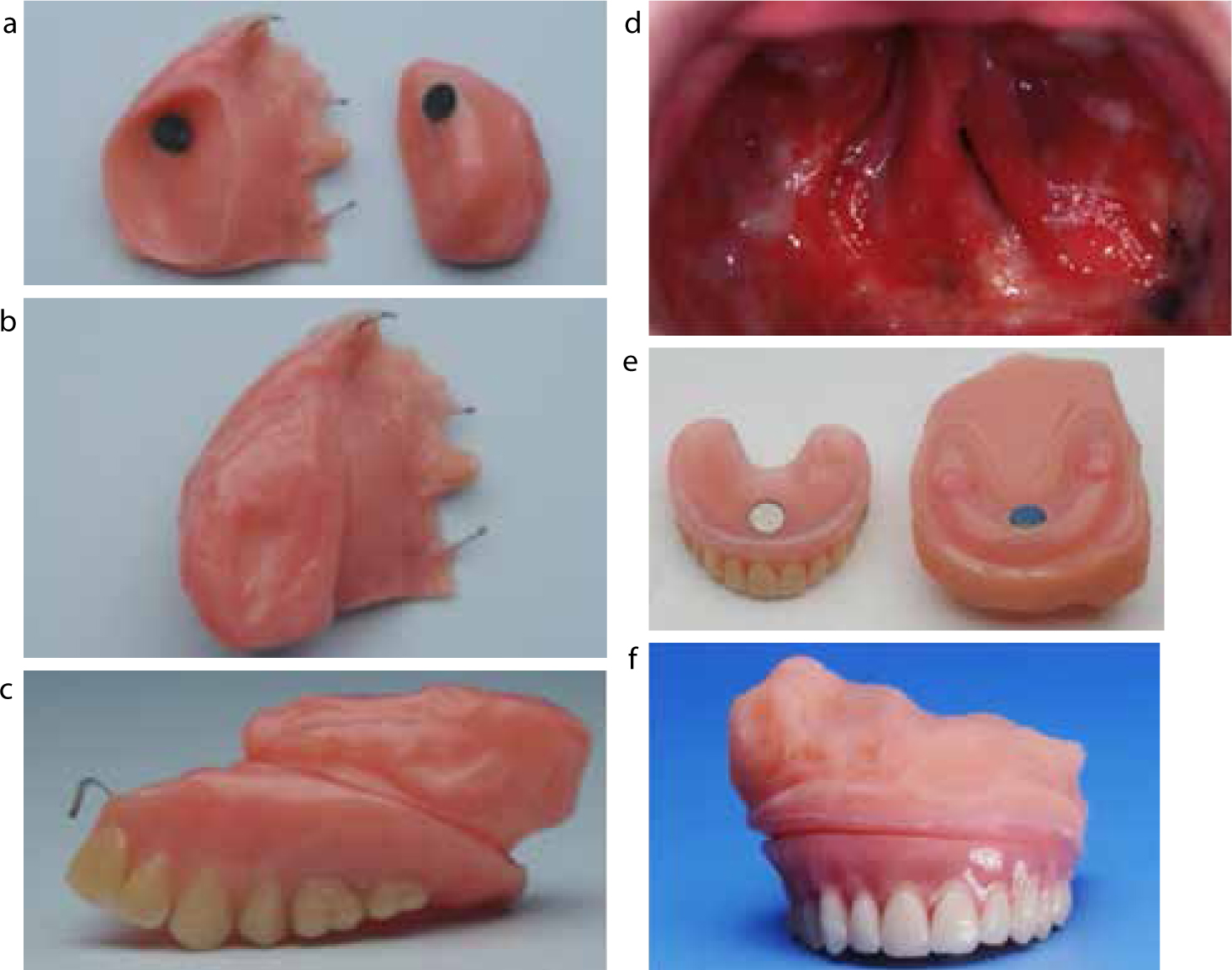
Hollow bulb obturators improve speech resonance and decrease the weight of the obturator. This helps to minimize any downward displacement of the prosthesis due to gravity or function. It was reported that 29% of obturator patients experience significant oral/nasal leakage.13 Therefore, the bulb must be carefully manufactured to produce an adequate seal and partition between the oral and nasal cavities. Hollow bulbs can also gain support from structures within the defect. Patients may have problems with insertion, and therefore a two-part design may have to be considered to overcome this problem, especially if the patient has significant trismus (Figure 4). If a two-part obturator is used, magnets can be used to unify the segments into one prosthesis. Magnets have been used to stabilize maxillofacial prostheses for over half a century14 and can be useful adjuncts for the restorative dentist. Typically, a magnet is embedded in the bung which the patient locates first into the defect. A separate magnet is on the denture portion of the appliance, which the patient inserts second. Such a design allows each segment of the obturator to have a separate path of insertion. Given that the magnets are self-seeking, it is easy for the patient to unite the denture with the bung.
Figure 4.
(a, b, c) A two-part, rigid hollow bulb obturator connected by magnets. (d, e, f) A patient who had her entire hard and soft palate resected. She was rehabilitated with a two-part obturator connected by magnets. The bung was made of resilient soft lining material.
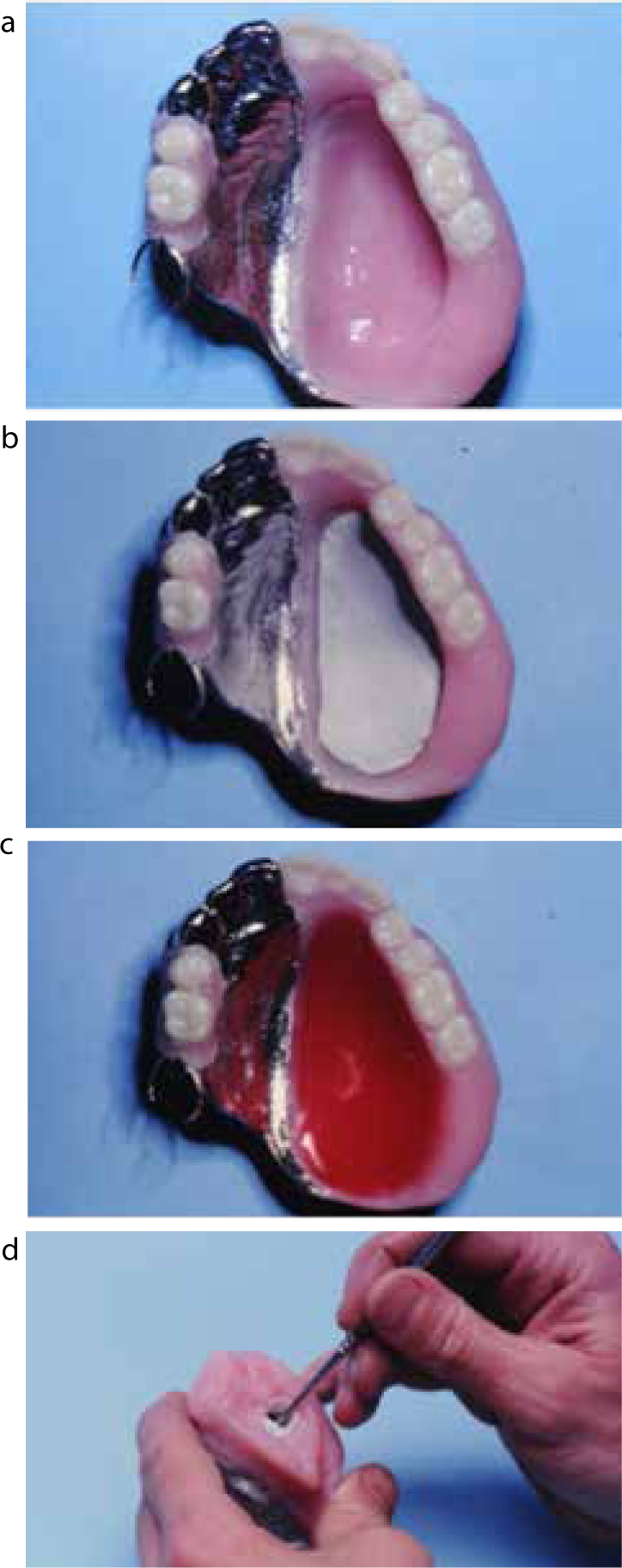
A method of producing a hollow bulb obturator is shown in Figure 5. The technician makes the hollow bulb in wax, before packing, flasking and processing it in acrylic resin. The hollow bulb is subsequently filled with ‘plaster of Paris’ and pumice. A lid is then waxed over the pumice/plaster-filled bulb before processing the obturator for a second cycle. Once complete, the pumice/plaster is carefully removed from the bulb via a small cavity in the superior aspect of the bung. This opening is then restored with self-cured acrylic resin.
Figure 5.
(a–d) Production of a hollow bulb for an oburator.
Using a flexible bung (Figure 4) can atraumatically engage undercuts within the defect more effectively than hard acrylic. These are typically made out of resilient lining material. Retention of the silicone bung is excellent when adequate tissue undercuts remain around the soft palate and on the buccal aspect of the defect.9 However, silicone rubbers flex under load. Consequently, the seal on the surgical site may be compromised when the patient masticates on the resected area. As a result, patients often chew on the unresected site. There are further problems with flexible bungs made of resilient lining material. They will need regular replacement and are difficult to adjust.15 Adjustment of the silicone bung can produce a rough surface which is difficult to clean and may encourage fungal growth.9 Therefore, where possible, the authors favour the use of hard acrylic. Open top designs tend to be smaller and lighter. The bulb can be carefully moulded to render the appliance more retentive (Figure 6). However, they clearly will accumulate unpleasant nasal secretions and will need to be cleaned regularly.
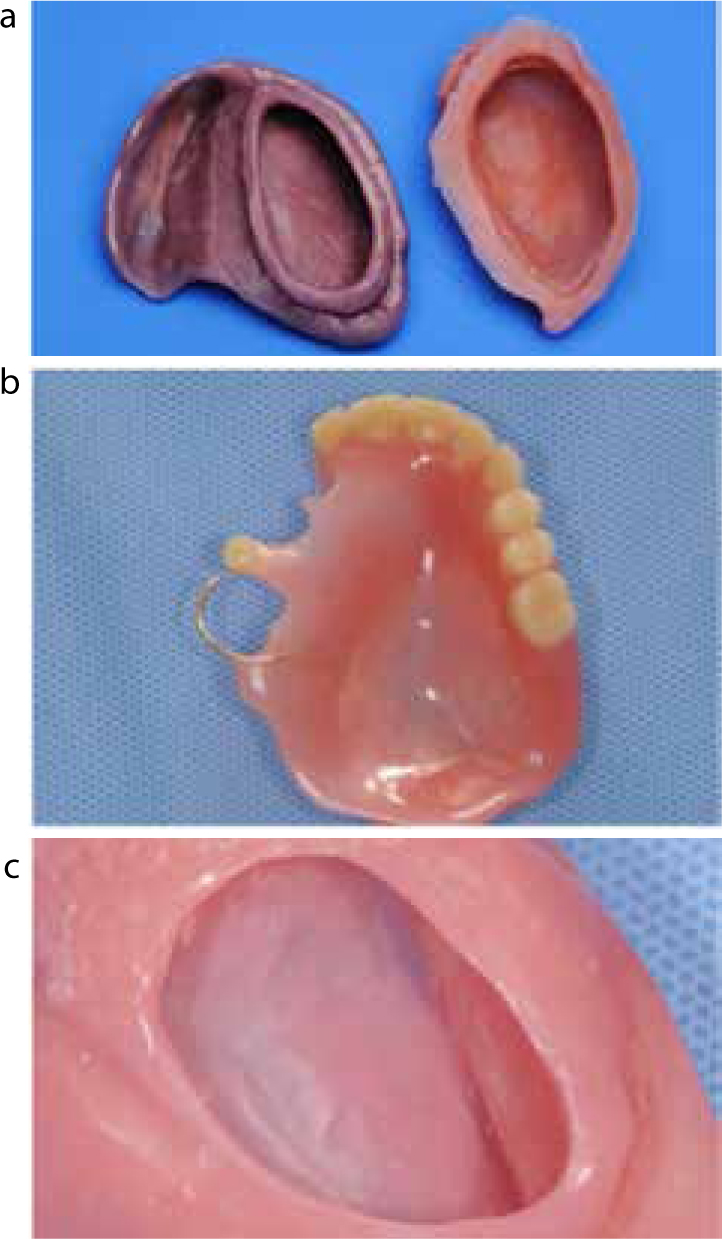
Figure 6.
(a) A two-part, acrylic obturator with a flexible open lid bung. (b, c) A one-part, acrylic obturator with a rigid, open lid bung.
Discussion
Given the variability in the different types of patient/defect/residual denture-bearing anatomy which the clinician may encounter, it is not possible to discuss specifics of obturator design. Therefore, the authors have attempted to discuss the general principles which underpin appliance design in this paper. The works of Desjardins6 and Aramany4 have been heavily quoted whilst describing the design features of an obturator. Their recommendations are not based on the results of any clinical, prospective, randomized control trials. Rather, they are based on their experiences having provided numerous prostheses for oncology patients. Readers are encouraged to study their published works to gain further insight into this complex and challenging field. Furthermore, a good understanding of basic prosthodontic theory relating to denture design, dental materials science and head and neck anatomy is an absolute prerequisite for anyone managing head and neck resection patients. These fundamental principles need to be understood when designing an obturator. The next and final part of this series will describe the clinical stages involved in the construction of an acrylic, one part, hollow bulb obturator.