The immune system: basis of so much health and disease: 5. complement Crispian Scully Eleni A Georgakopoulou Yazan Hassona Dental Update 2024 44:7, 707-709.
The immune system is the body's primary defence mechanism against infections, and disturbances in the system can cause disease if the system fails in defence functions (in immunocompromised people), or if the activity is detrimental to the host (as in auto-immune and auto-inflammatory states). A healthy immune system is also essential to normal health of dental and oral tissues. This series presents the basics for the understanding of the immune system, this article covers complement and other mediators of inflammation.
Clinical Relevance: Modern dental clinicians need a basic understanding of the immune system as it underlies health and disease.
Article
’Complement’ is a system of at least nine plasma proteins, synthesized mainly by the liver. Complement functions include:
Clumping of antigen-bearing agents;
Processing of immune (antigen-antibody) complexes;
Chemotaxis – attracting phagocytes;
Opsonization – enhancing phagocytosis of antigens;
Lysis – rupturing membranes of micro-organisms or foreign cells;
Altering the molecular structure of viruses;
Enhancing antibody formation;
Activation of mast cells and basophils to release histamine and other inflammatory mediators.
Complement proteins can be activated in sequence (comparable to the blood clotting cascade) by a variety of triggering agents.
There are at least three complement pathways:
The classical;
The alternative; and
The mannose-binding lectin pathway.
Activation of the complement pathways
The classical pathway
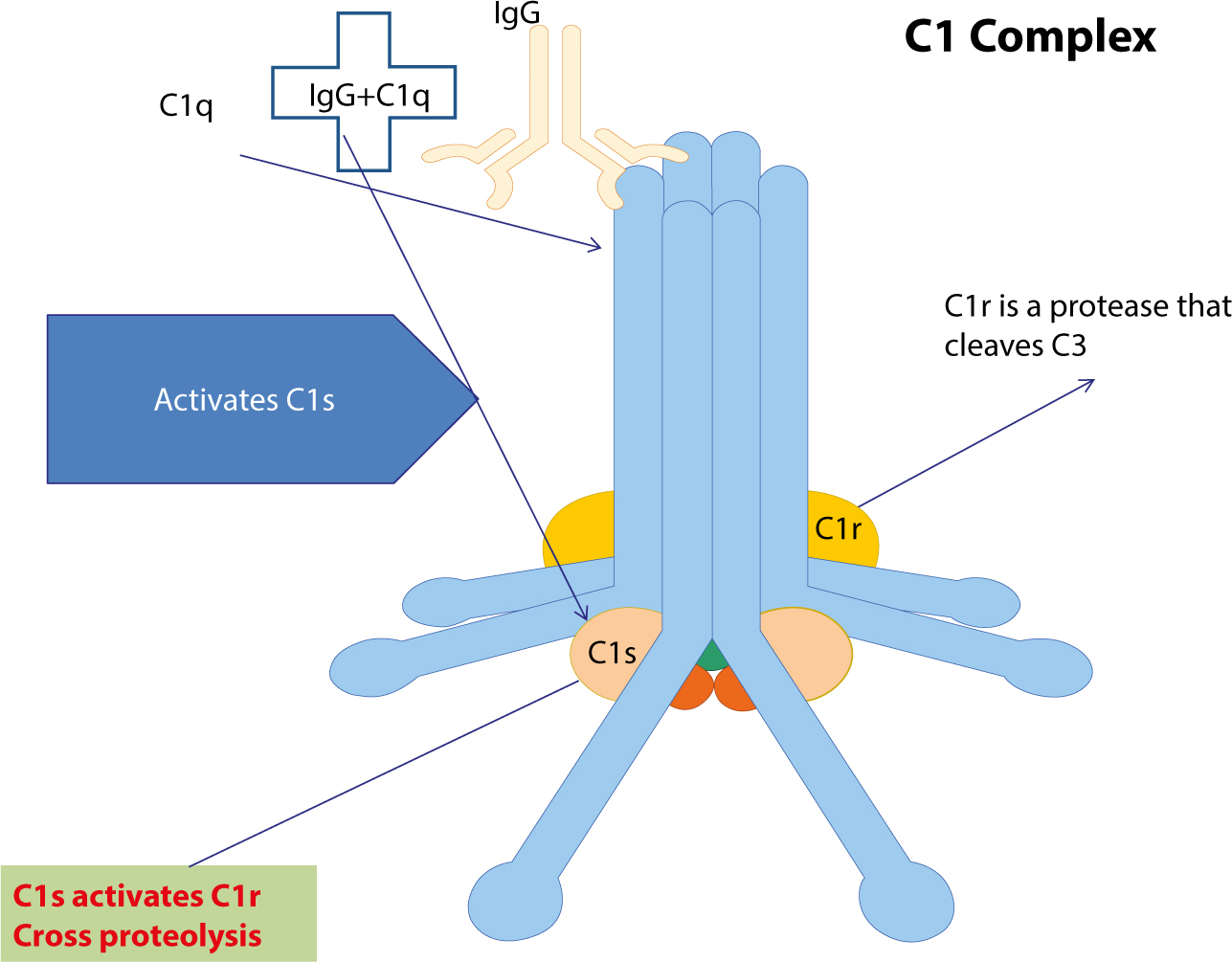
This is activated by immunoglobulins (antibodies), either attached to a cell surface antigen or as immune (antigen-antibody) complexes. Binding of complement component C1q (Figure 1) to IgG or IgM antibodies activates the rest of the complement pathway by auto-catalytically converting another component of C1, to an active enzyme that ultimately converts C3 to C3a, C3b and thus to C5a and C5b. C1 can also be activated by C-reactive protein, and serum amyloid protein (Figure 2).
Figure 1. C1 is the first protein of the classical pathway. C1q is an arrangement of six matching subunits with globular tops and extended collagen-like extremities. The extensions link to come together with two molecules of C1r and C1s, and create the C1 complex. The tops bind to the stable areas of immunoglobulin or directly to the pathogen surface, and modify the C1r, which is then cleaved and the active part triggers the C1s zymogen.Figure 2. Three pathways of complement activation have been described: 1. The classical pathway (left), which is initiated either by antibodies or by the straight fastening of C1q to the surface of pathogen; 2. The MB-lectin (MBL-centre) pathway, which is triggered by the mannose-binding lectin, a regular ingredient of normal serum that connects with various encapsulated bacteria; 3. The alternative pathway (right), which is activated straightforwardly on pathogen surfaces. All three pathways result in a sequential enzymatic pursuit which produces the final effector molecules of complement. The major results of complement activation are the opsonization of pathogens, the recruitment of inflammatory cells, and lysis of pathogens.
The alternative pathway
This is activated by a range of foreign cell-surface constituents such as of Gram-positive and Gram-negative bacteria (eg bacterial endotoxin [lipopolysaccharides, LPS], polysaccharide capsules, fungi, some viruses, tumour cells and aggregates of IgE and properdin. Activation of the alternative pathway requires four proteins, C3, Factor B, Factor D and properdin (Figure 2).
The mannose-binding lectin pathway
This is activated by mannose-binding protein which activates C1 (Figure 2).
Numbering of each component of the classical pathway
Numbering of each component of the classical pathway of complement is from C1–C9. The sequence in which complement components are activated is C1, C4, C2, C3 and C5–C9 (since C4 was identified before, its position in the path was established). When a complement component becomes enzymatically active, this is signified by drawing a bar above its name or designation. When a molecule is cleaved, the smaller portion is called the ‘a’ fragment, and the larger the ‘b’ fragment. The core event during complement activation is the proteolytic cleavage of C3 to C3a which is common to all three pathways as well as the downstream events.
Complement fragments are usually biologically active (Table 1)
The main activities of complement fragments include:
C3a and C5a (also termed anaphylatoxins) are mediators of inflammation, mast cell degranulation, smooth muscle contraction and chemotaxis for phagocytes;
C3b is capable of opsonizing micro-organisms for phagocytosis;
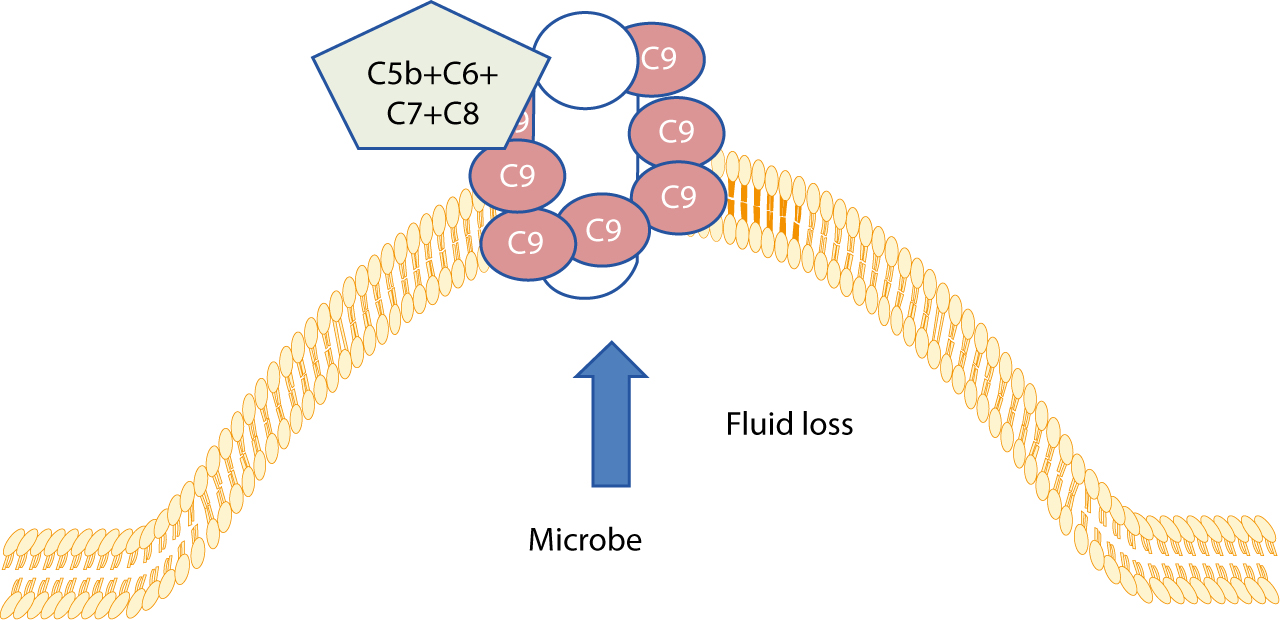
C5–C9 is a membrane attack complex capable of causing cell membrane damage (Figure 3).
Figure 3. This complex of C5b, C6, C7, C8 and C9 complement proteins creates pores on the surface of microbes which results in their lysis through osmotic loss of fluids.
Other features of complement
Phagocytes are attracted towards antigens by activated complement after an antigen-antibody reaction. Neutrophils and macrophages are dedicated phagocytes which can ingest and often kill opsonized (coated by specific antibody and activated complement components) micro-organisms, especially bacteria.
Complement can also have harmful effects if activated:
On a large scale (eg by Gram-negative bacilli);
By an autoimmune response to host cells (autoimmune disorders)
Complement thus has the potential to protect or damage the host.
Control of complement
Complement is controlled by a number of regulatory mechanisms, including control proteins in plasma and on the membranes of self-cells preventing them from being targeted by complement. Controls include (Table 2):
A family of proteins that regulate C3 convertase activity;
Protectin (CD59) – which inhibits C9 polymerization during the membrane attack complex formation;
Decay Accelerating Factor (DAF);
Membrane Inhibitor of Reactive Lysis (MIRL); and
Homologous Restriction Factor (HRF).
Evaluation of the complement system
Most complement components can be detected by using antibody sensitized sheep erythrocytes in a total haemolytic complement assay (CH50 assay) since this assay requires the functional integrity of C1–C9.
Deficiencies of alternative pathway components Factors D, H and I and properdin can be detected by a haemolytic assay using activators of the alternative pathway, such as unsensitized rabbit erythrocytes.
Individual components are detected by specialized functional and immunochemical tests. The assays for complement most applicable in daily practice are the immunochemical assays of C3 and C4. Such tests can indicate which pathway is activated and the possible cause. For example, a low C3 and C4 with a normal factor B (factor B is only involved in the alternative pathway) (Figure 2) indicate activation of the classical pathways (a possible cause could be systemic lupus erythematosus or vasculitis).
Other mediators of inflammation
Other mediators of inflammation include:
Reactive Oxygen Species (ROS);
Cytokines;
Vasoactive amines (histamine, serotonin, and bradykinin);
Prostaglandins, thromboxanes and leukotrienes; and
Liver acute phase proteins.
Reactive oxygen species (ROS)
Reactive oxygen species (ROS) include factors such as nitric oxide (NO). NO is produced via arginine catalysed by nitric oxide synthase; via arginase to ornithine and then ornithine decarboxylase (ODC) catalyses the conversion of ornithine to polyamines. Regulatory circuits control the production of ROS and NO, to avoid overproduction of these dangerous compounds.
Cytokines
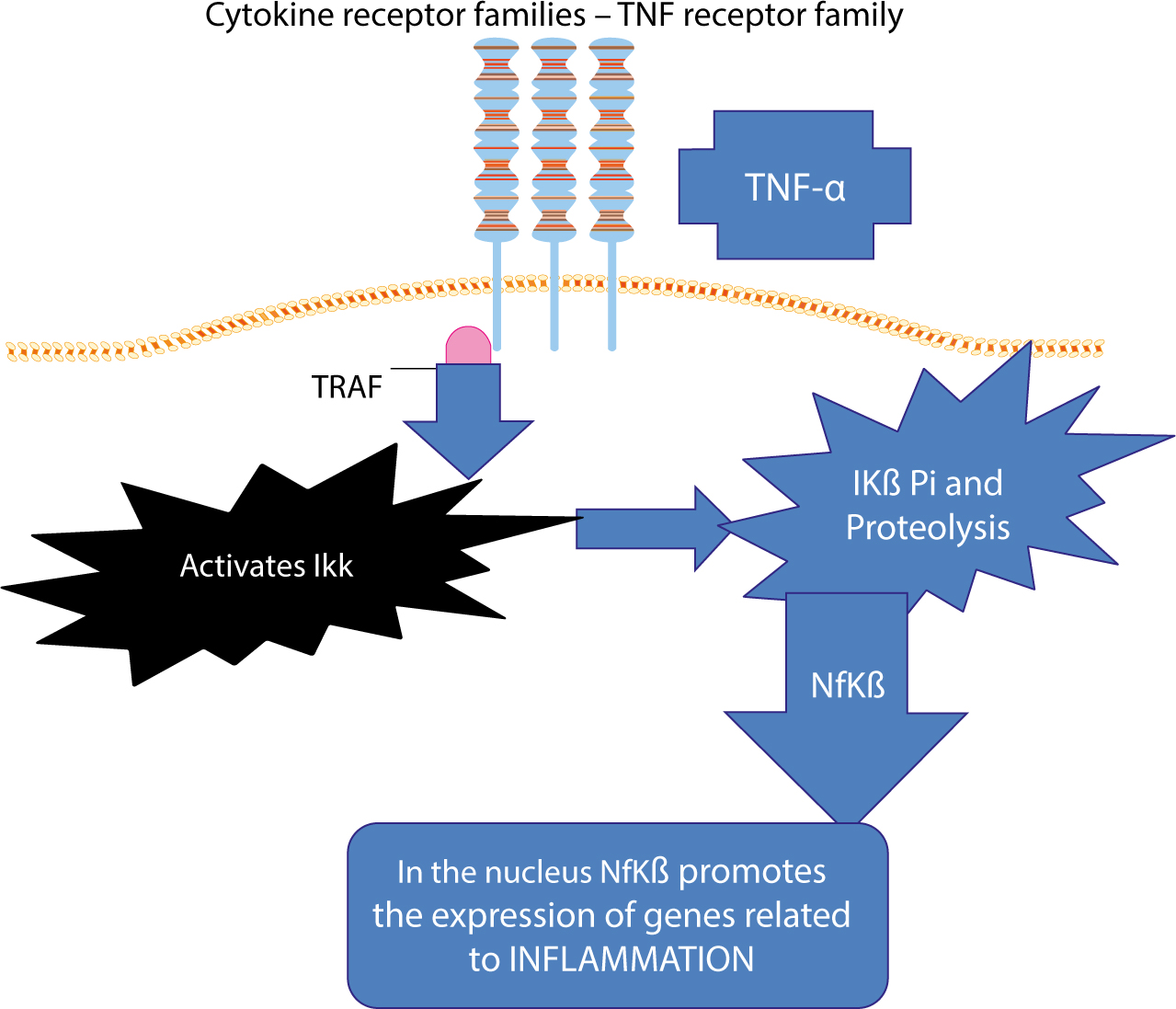
These are signalling molecules which can act in an autocrine or paracrine way via cell surface receptors to mediate and regulate the amplitude and duration of innate immunity, through activation of macrophages, controlling growth and differentiation of T- and B-cells. Cytokines are produced by activated microphages and Natural Killer (NK) cells in response to microbial infection, and act mainly on endothelial cells and leukocytes to stimulate the early inflammatory response to microbes. Pro-inflammatory cytokines include TNFs and interleukins (IL-1β, IL-6 and IL-8). TNF-alpha (TNF-α) is a dominant pro-inflammatory cytokine. Produced by monocytes and activated macrophages and a range of immunocytes and other cells, TNF-α is a soluble protein, which can bind to specific cell surface receptors such as TNF receptor (TNFR1), triggering inflammation, the immune response and cell differentiation. Binding of TNF-α to TNFR1 causes binding of a molecule called TNFR-associated death domain (TRADD), which can then recruit TNF-associated factor 2 (TRAF2), leading to activation of Nf-kβ, activator protein 1, and the JUN–n-terminal kinase pathway, resulting in inflammation. TRADD can also associate with the Fas-associated death domain, which leads to recruitment and cleavage of pro-caspase 8 and to programmed cell death (apoptosis) (Figure 4).
Figure 4. TNF-α binds to its membrane receptor and activates the TRAF molecule which, by a cascade of phosphorylations (Pi) and proteolytic changes of the Ikβ kinase complex, results in the translocation of active Nfkβ (nuclear factor kβ) transcription factor in the nucleus where it promotes the expression of inflammatory genes.
Thus TNF-α can induce either inflammation or apoptosis.
TNF can also have other effects, such as:
Up-regulating adhesion molecules on vascular endothelial cells;
Enhancing major histocompatibility complex (MHC) Class I and II antigen expression (co-stimulatory molecules on dendritic cells, and macrophages, for antigen presentation), thus initiating and perpetuating inflammation;
Inducing matrix metallo-proteinases (MMPs) production by stromal cells leading to tissue remodelling and enhanced tumour necrosis factor (TNF)-mediated secretion of keratinocyte growth factor (KGF);
Inducing fever, either directly via stimulation of prostaglandin synthesis by the hypothalamus, or indirectly by inducing release of IL-1;
Stimulating the liver production of collagenase, acute phase reactants, and IL-6, which then perpetuate inflammation via a cytokine cascade.
Some cytokines (for example, IL-8) are also chemotactic for specific cell types, and are thus also called ‘chemokines’. Interleukin-1 (IL-1) is synthesized from larger precursors (inflammasomes) cleaved by a caspase-1 in macrophages and neutrophils. IL-1, from macrophages and monocytes, stimulates synthesis and secretion of other interleukins which help to activate T-cells and thus initiate an adaptive immune response.
Vasoactive amines (histamine, serotonin and bradykinin)
These (and leukotrienes) sensitize pain receptors, cause vasodilatation and increased capillary permeability, and are also active in either recruiting and/or activating leukocytes to produce their own inflammatory mediators. Phagocytes also release inflammatory mediators (eg leukotrienes such as LTB4 and prostaglandins such as PGE2).
Prostaglandins, thromboxanes and leukotrienes
These are arachidonic acid-derived eicosanoids which are potent mediators of inflammation, and include:
Prostaglandin H2 (PGH2) released via the cyclo-oxygenase (COX) pathway, leading to several other prostaglandins (PGs) and leukotrienes (LTs) via the 5-lipoxygenase pathway;
Properdin (known also as Factor P), a protein involved in:
Complement activation (alternative pathway);
Inflammation;
Phagocytosis;
Virus neutralization.
Liver acute phase proteins
Liver acute phase proteins, including C-Reactive Protein (CRP), serum amyloid and serum amyloid A component, which are released into the circulation. CRP can bind to some bacteria and fungi, activating complement. Serum amyloid also activates complement. Serum amyloid A can stimulate macrophages to engulf debris.
Acute phase response
In response to injury, infection, physical trauma, or malignancy, phagocytes (neutrophils and macrophages) secrete several inflammatory cytokines (most notably IL-1, IL-6, IL-8 and TNF-α) which stimulate the liver to produce acute-phase reactants – proteins whose plasma concentrations increase in response to, and suppress, inflammation (Tables 3 and 4). For a protein to be considered as acute phase a plasma concentration change of 25% is required. Acute phase proteins are used as biomarkers of non-specific inflammation and can be detected both in acute and chronic inflammation. They can be helpful in screening for disease.