De Jongh A, Adair P, Meijerink-Anderson M. Clinical management of dental anxiety: what works for whom?. Int Dent J. 2005; 55:73-80
Armfield JM, Stewart JF, Spencer AJ. The vicious cycle of dental fear: exploring the interplay between oral health, service utilization and dental fear. BMC Oral Health. 2007; 7
Armfield JM, Slade GD, Spencer AJ. Dental fear and adult oral health in Australia. Community Dent Oral Epidemiol. 2009; 37:220-230
Oosterink FM, de Jongh A, Hoogstraten J. Prevalence of dental fear and phobia relative to other fear and phobia subtypes. Eur J Oral Sci. 2009; 117:135-143
Coriat IH. Dental anxiety; fear of going to the dentist. Psychoanal Rev. 1946; 33:365-367
van Wijk AJ, Hoogstraten J. The Fear of Dental Pain questionnaire: construction and validity. Eur J Oral Sci. 2003; 111:12-18
, 5th edn. Washington, DC: American Psychiatric Association; 2013
Moore R, Brodsgaard I, Abrahamsen R. A 3-year comparison of dental anxiety treatment outcomes: hypnosis, group therapy and individual desensitization vs. no specialist treatment. Eur J Oral Sci. 2002; 110:287-295
Deacon BJ, Abramowitz JS. Cognitive and behavioral treatments for anxiety disorders: a review of meta-analytic findings. J Clin Psychol. 2004; 60:429-441
Craske MG, Treanor M, Conway CC, Zbozinek T, Vervliet B. Maximizing exposure therapy: an inhibitory learning approach. Behav Res Ther. 2014; 58:10-23
Gauthier J, Savard F, Hallé J-P, Dufour L. Flooding and coping skills training in the management of dental fear. Scand J Behav Therapy. 1985; 14:3-15
Smith TA, Kroeger RF, Lyon HE, Mullins MR. Evaluating a behavioral method to manage dental fear: a 2-year study of dental practices. J Am Dent Assoc. 1990; 121:525-530
Moore R, Brodsgaard I, Berggren U, Carlsson SG. Generalization of effects of dental fear treatment in a self-referred population of odontophobics. J Behav Ther Exp Psychiatry. 1991; 22:243-253
Gros DF, Antony MM. The assessment and treatment of specific phobias: a review. Curr Psych Reps. 2006; 8:298-303
Garcia-Palacios A, Hoffman HG, See SK, Tsai A, Botella C. Redefining therapeutic success with virtual reality exposure therapy. Cyberpsychol Behav. 2001; 4:341-348
Botella C, Baños RM, Villa H, Perpiñá C, García-Palacios A. Virtual reality in the treatment of claustrophobic fear: a controlled, multiple-baseline design. Behav Ther. 2000; 31:583-595
Krijn M, Emmelkamp PM, Biemond R, de Wilde de Ligny C, Schuemie MJ, van der Mast CA. Treatment of acrophobia in virtual reality: the role of immersion and presence. Behav Res Ther. 2004; 42:229-239
Muhlberger A, Wiedemann G, Pauli P. Efficacy of a one-session virtual reality exposure treatment for fear of flying. Psychother Res. 2003; 13:323-336
Garcia-Palacios A, Hoffman H, Carlin A, Furness TA, Botella C. Virtual reality in the treatment of spider phobia: a controlled study. Behav Res Therap. 2002; 40:983-993
Parsons TD, Rizzo AA. Affective outcomes of virtual reality exposure therapy for anxiety and specific phobias: a meta-analysis. J Behav Ther Experiment Psychiatry. 2008; 39:250-261
McLay RN, Graap K, Spira J, Perlman K, Johnston S, Rothbaum BO Development and testing of virtual reality exposure therapy for post-traumatic stress disorder in active duty service members who served in Iraq and Afghanistan. Milit Med. 2012; 177:635-642
Baus O, Bouchard S. Moving from virtual reality exposure-based therapy to augmented reality exposure-based therapy: a review. Front Hum Neurosci. 2014; 8
North MM, North SM, Coble JR. Virtual reality therapy: an effective treatment for psychological disorders. Stud Health Technol Inform. 1997; 44:59-70
Raghav K, Van Wijk AJ, Abdullah F, Islam MN, Bernatchez M, De Jongh A. Efficacy of virtual reality exposure therapy for treatment of dental phobia: a randomized control trial. BMC Oral Health. 2016; 16
Wald J. Efficacy of virtual reality exposure therapy for driving phobia: a multiple baseline across-subjects design. Behav Ther. 2004; 35:621-635
Powers MB, Emmelkamp PM. Virtual reality exposure therapy for anxiety disorders: a meta-analysis. J Anxiety Disord. 2008; 22:561-569
Wolpe J.New York: Pergamon; 1969
Luyk NH, Beck FM, Weaver JM. A visual analogue scale in the assessment of dental anxiety. Anesth Prog. 1988; 35:121-123
Facco E, Zanette G, Favero L, Bacci C, Sivolella S, Cavallin F, Manani G. Toward the validation of visual analogue scale for anxiety. Anesth Prog. 2011; 58:8-13
Humphris GM, Morrison T, Lindsay SJ. The Modified Dental Anxiety Scale: validation and United Kingdom norms. Community Dent Health. 1995; 12:143-150
Kleinknecht RA, Klepac RK, Alexander LD. Origins and characteristics of fear of dentistry. J Am Dent Assoc. 1973; 86:842-848
Humphris GM, Freeman R, Campbell J, Tuutti H, D'Souza V. Further evidence for the reliability and validity of the Modified Dental Anxiety Scale. Int Dent J. 2000; 50:367-370
Davis TE, Ollendick TH, Öst LG.London: Springer; 2012
Hersen M.Texas, USA: Gulf Professional Publishing; 2006
Doering S, Ohlmeier MC, de Jongh A, Hofmann A, Bisping V. Efficacy of a trauma-focused treatment approach for dental phobia: a randomized clinical trial. Eur J Oral Sci. 2013; 121:584-593
Hoffman HG, Garcia-Palacios A, Patterson DR, Jensen M, Furness T, Ammons WF The effectiveness of virtual reality for dental pain control: a case study. Cyberpsychol Behav. 2001; 4:527-535
Thomas Juster F.New York: Columbia University Press; 1966
First MB, Gibbon M. The Structured Clinical Interview for DSM-IV Axis I Disorders (SCID-I) and the Structured Clinical Interview for DSM-IV Axis II Disorders (SCID-II).Oxford: John Wiley & Sons Inc; 2004
, 4th edn. : American Psychiatric Association; 2000
Campbell DT, Stanley JC, Gage NL.Boston: Houghton Mifflin; 1963
Krijn M, Emmelkamp PM, Olafsson RP, Biemond R. Virtual reality exposure therapy of anxiety disorders: a review. Clin Psychol Review. 2004; 24:259-281
Virtual reality exposure therapy for treatment of dental phobia Kumar Raghav Gujjar Ratika Sharma Ad De Jongh Dental Update 2024 44:5, 707-709.
Authors
Kumar RaghavGujjar
MDS(Paediatric Dentistry)
PhD Candidate, Department of Social Dentistry, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and VU University, 1081 LA Amsterdam, The Netherlands; Senior Lecturer, Faculty of Dentistry, SEGi University, No 9 Jalan Teknologi, Kota Damansara, PJU-5, Petalingjaya-47810, Selangor, Malaysia
PhD Candidate, School of Public Health, The University of Queensland, Public Health Building, Cnr Wyndham St and Herston Rd, Herston QLD 4006, Australia
Professor, Department of Social Dentistry, Academic Centre for Dentistry Amsterdam (ACTA), University of Amsterdam and VU University, 1081 LA Amsterdam, The Netherlands; School of Health Sciences of Salford University, Manchester, UK
Virtual Reality Exposure Therapy (VRET) has gained in popularity as an effective treatment for anxiety disorders. The purpose of this article is to determine the applicability of VRET in the treatment of dental phobia of two patients. Two case examples of female dental patients, aged 56 and 24 years, who met the criteria for dental phobia according to the Phobia Checklist, illustrate the use of VRET in the dental setting. VRET that is used as a psychological treatment for dental fear and dental phobia can potentially be given by a non-specialist (for example dental assistant), thereby making it a cost-effective therapy for the treatment of dental phobia.
CPD/Clinical Relevance: This article is the first of its kind to demonstrate Virtual Reality Exposure Therapy (VRET) in the treatment of dental anxiety.
Article
A substantial proportion of the population suffers from dental fear.1 This fear can result in a reduced number of dental visits2 and poor oral health.3 When the avoidance,4 anxious anticipation,5 or distress6 in the feared situations interferes significantly with the person‧s normal routine, occupational functioning, social activities or relationships, or there is a marked distress about having the dental fear, the condition is termed as ‘dental phobia’. Dental phobia is classified as a specific phobia within the DSM-5 (Diagnostic and Statistical Manual of Mental Disorders 5th edn).7
With regard to the treatment of fears and phobias, therapeutic procedures using gradual and systematic confrontations with the fearful objects and situations, such as systematic desensitization and in vivo exposure, are the first line treatments.8-10 These procedures can be applied either in imaginal (in vitro), or in real life (in vivo). Since imaginary procedures have been found to be less effective than in vivo exposure, the latter has generally been accepted as the treatment of choice.11 The basic assumption of in vivo exposure is that a fear response gradually extinguishes when the provoking stimulus (for instance, the sound of the drill) is repeatedly presented, but is not followed by an aversive event (eg one involving pain) so that the person learns that such feared consequences are not likely to happen.12
A large array of studies supports the efficacy of exposure therapy as the treatment of choice for specific fears and phobias,8,9,10 including dental-related fears.13,14,15,16 However, one major drawback of this approach that has been identified is that individuals may be too frightened to face their fears owing to the anticipatory anxiety5 of getting harmed while confronting the real situation (as in in vivo exposure therapy). This may result in refusal or termination of therapy.17 Thus, any therapy for dental anxiety which is less mentally demanding for dental phobic patients could potentially improve their compliance and adherence to treatment.
Virtual Reality Exposure Therapy (VRET) is a relatively novel cognitive-behavioral approach which has been successfully used for treating a number of specific phobia subtypes, including fear of enclosed spaces,18 fear of heights,19 fear of flying,20 and spider phobia.21 VRET is carried out in a contextually-related,22 computer-generated virtual environment, which facilitates systematic confrontations with the fear-provoking stimuli.
One important advantage of VRET is that the clients face the computer-generated (virtual) counterpart of their fearful stimuli in a gradual and controlled manner23 at their own pace,24 and under the privacy of the therapist‧s office.25 Additionally, while in vivo exposure is usually delivered by a trained psychologist, and requires training on the part of a therapist, administration of VRET may only need knowledge of computer operation and training to run the VRET software.26 Moreover, VRET may also be safer, less embarrassing, and cost-effective therapy compared to reproducing a real-world situation as in in vivo exposure.27 Indeed, a recent meta-analysis has suggested that VRET is equally effective, and slightly better compared to the gold standard in vivo exposure therapy, in the treatment of anxiety disorders.28
Although VRET exhibits a powerful modifying affect because of its immersive nature, the effectiveness of VRET has not been tested yet on patients suffering from dental phobia. The aim of this article is to present the initial findings of the application of VRET on two patients with dental phobia.
Case presentation
Two patients reported to the SEGi Oral Health Centre, Malaysia with a history of repeated avoidance of dental treatment and self-reported dental fear for more than two years. Patient A was a 56-year-old Malay female with a fear of pain and sensitivity resulting from the use of the dental drill. Her fear of dental drills had roots in a traumatic childhood dental experience. During the clinical interview she recounted that, at the age of 12 years, she was subjected to a dental drill and fill procedure whilst she experienced severe sensitivity and pain. On reporting the pain, she was ridiculed and forced to complete the treatment by the dentist and the nurse. She reported having painful memories of ‘very rough handling’ by her dentist and her experience of ‘gripping the handle of the dental chair tightly’. The scolding, belittlement and embarrassment accrued from the dental team initiated intense distrust and fear towards subsequent dental treatments. She had evaded dental treatment for the past two years when she reported to us. At the time of her visit, she required multiple dental fillings and was extremely anxious about her dental treatment procedures.
Patient B was a 24-year-old Malay female who was extremely fearful of getting pain and sensitivity from sharp dental instruments and dental drills. Similar to the previous case, her dental fear also had origins in a childhood traumatic dental experiences, starting when she was 10 years old. She described the dentist jabbing her gums many times while performing scaling which resulted in severe pain and bleeding. The dentist did not respond to her repeated pleas to stop because the scaler was hurting her. She was also horrified to see a significant amount of blood in her spit after the procedure. The second traumatic dental experience occurred when she was 16 years old, and visited another dentist for a tooth restoration procedure. She recollected feeling helpless during the procedure as the injection was ineffective and, despite complaining about sensitivity, the dentist did not stop drilling her tooth. Her traumatic dental experiences resulted in an extreme distrust of dentists and complete avoidance of any dental treatment for three years. During her visit, she required several dental procedures such as scaling and dental restorations and was extremely anxious about her dental treatment.
The specific clinical criteria of the two patients included, the lack of any:
Hearing or visual impairments such as stereoscopy blindness or nystagmus;
Mental disorders such as psychosis, post-traumatic stress disorder, developmental or intellectual disability and cognitive impairment;
Known balance disorders such as vertigo and cybersickness;
Previous history of epileptic seizures;
History of cardiac problems.
Furthermore, both patients had no other specific phobia and had never received any treatment for their dental anxiety in the past.
The patients were interviewed using the ‘phobia checklist’4 for dental phobia. Based on the history, examination and ‘phobia checklist’ criteria, the diagnosis ‘dental phobia’ was confirmed for both the patients.
Treatment
The patients were given an explanation about the procedure of VRET in detail and informed consents were obtained from both patients. They self-rated their baseline level of state anxiety with a Visual Analogue Scale (VAS-A), and their level of dental trait anxiety with both the Modified Dental Anxiety Scale (MDAS), and the Dental Fear Survey (DFS). In addition, prior to therapy, the patients underwent a behaviour test to assess their ability to confront dental situations.
VRET was conducted with a simulator computer which rendered the virtual dental environment and the other (user interface) computer allowed the researcher (KR) to control and individualize stimuli presented. The simulator computer comprised a DELL XPS 8700 Desktop with a NVIDIA GeForce GTX 750 TI OC 2GB GDDR5 graphic card. The simulator computer displayed a 3D stereoscopic scene through the Oculus Development Kit-2 Head Mounted Device (HMD) to the patient.
The patients were asked to sit in the dental chair and were assisted in wearing the HMD by the researcher. The VR (Virtual Reality) system displayed a surrounding 3D stereoscopic scene of a simulated dental operatory with a dental chair, overhead light, and dental instruments through the HMD to the patients. To enhance immersion characteristic of the virtual environment, the typical smell of a dental clinic (drops of oil of cloves on cotton wool) was introduced. Initially, the patients were made to view the simulated dental environment scene passively for two minutes to facilitate orientation. The built- in motion tracking in the HMD allowed the patients to turn their heads and look around. The patients were able to see their virtual counterpart inside the HMD as they explored the virtual dental operatory by moving their heads.
The researcher was able to view and control what the patients were seeing in the simulated dental environment on the user interface computer screen (eg virtual dentist movements). Patients were exposed to the following hierarchy of virtual scenarios:
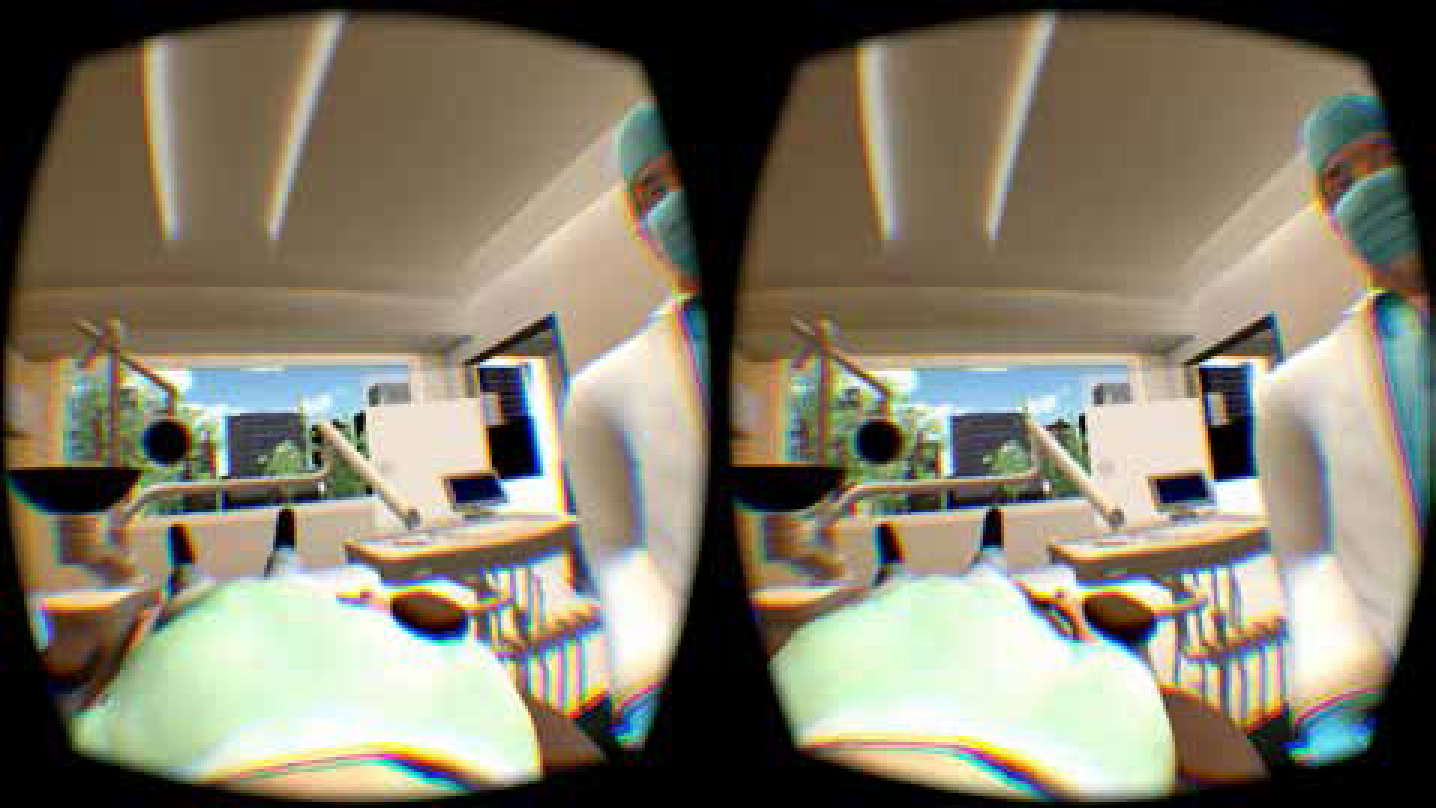
Sitting on the dental chair (no tools) – screen shot shown in Figure 1;
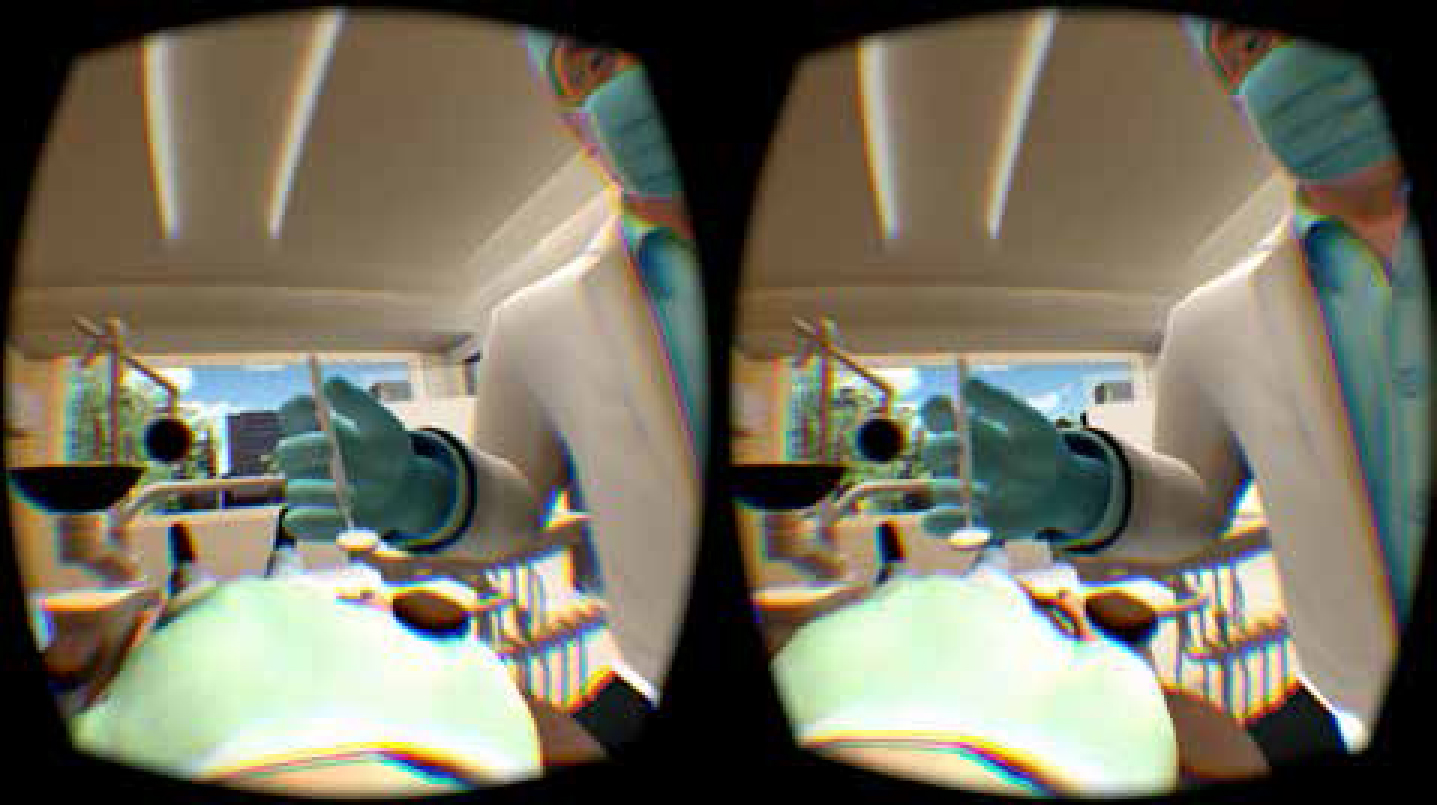
Inspection of the oral cavity using mouth mirrors – screen shot shown in Figure 2;
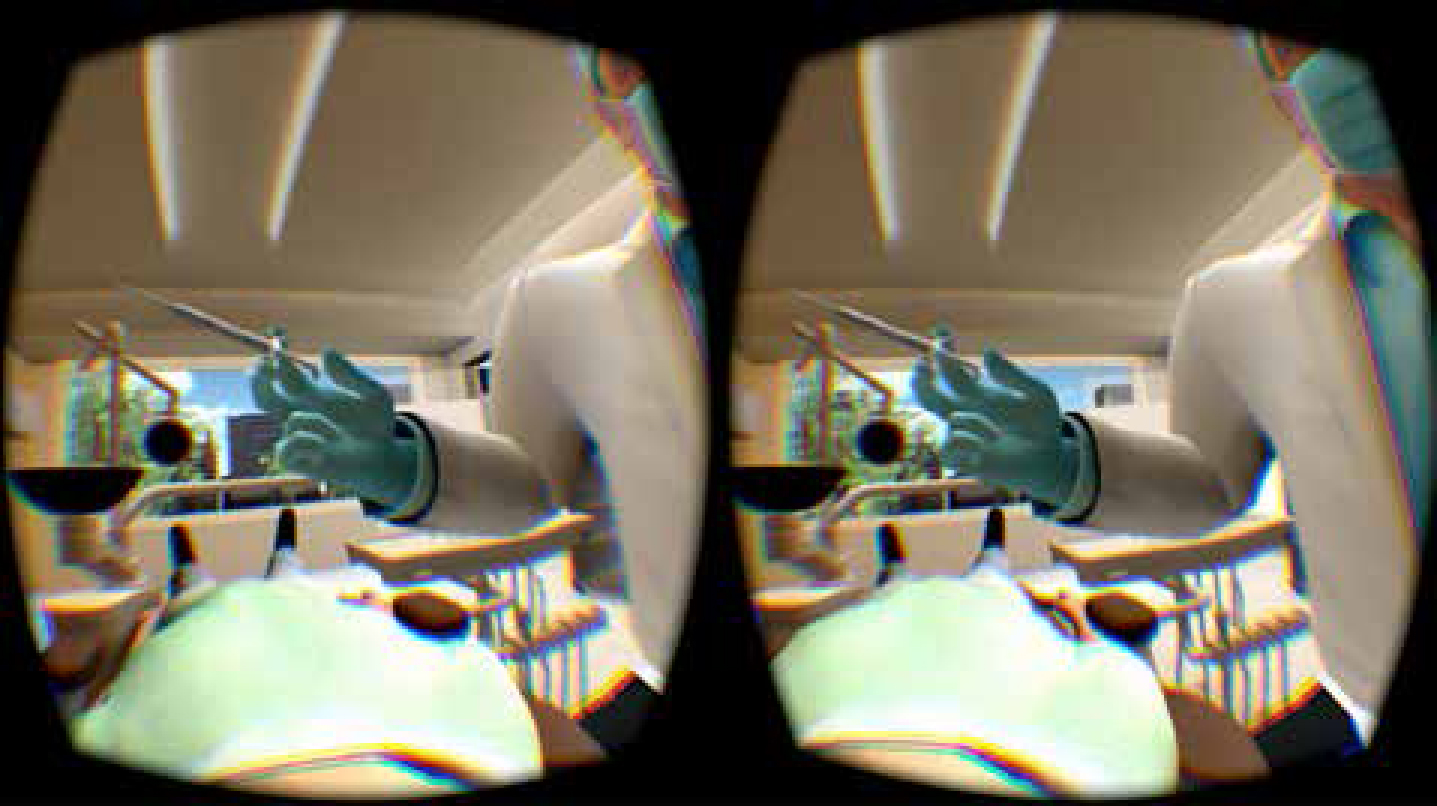
The introduction of an injection – screen shot shown in Figure 3;
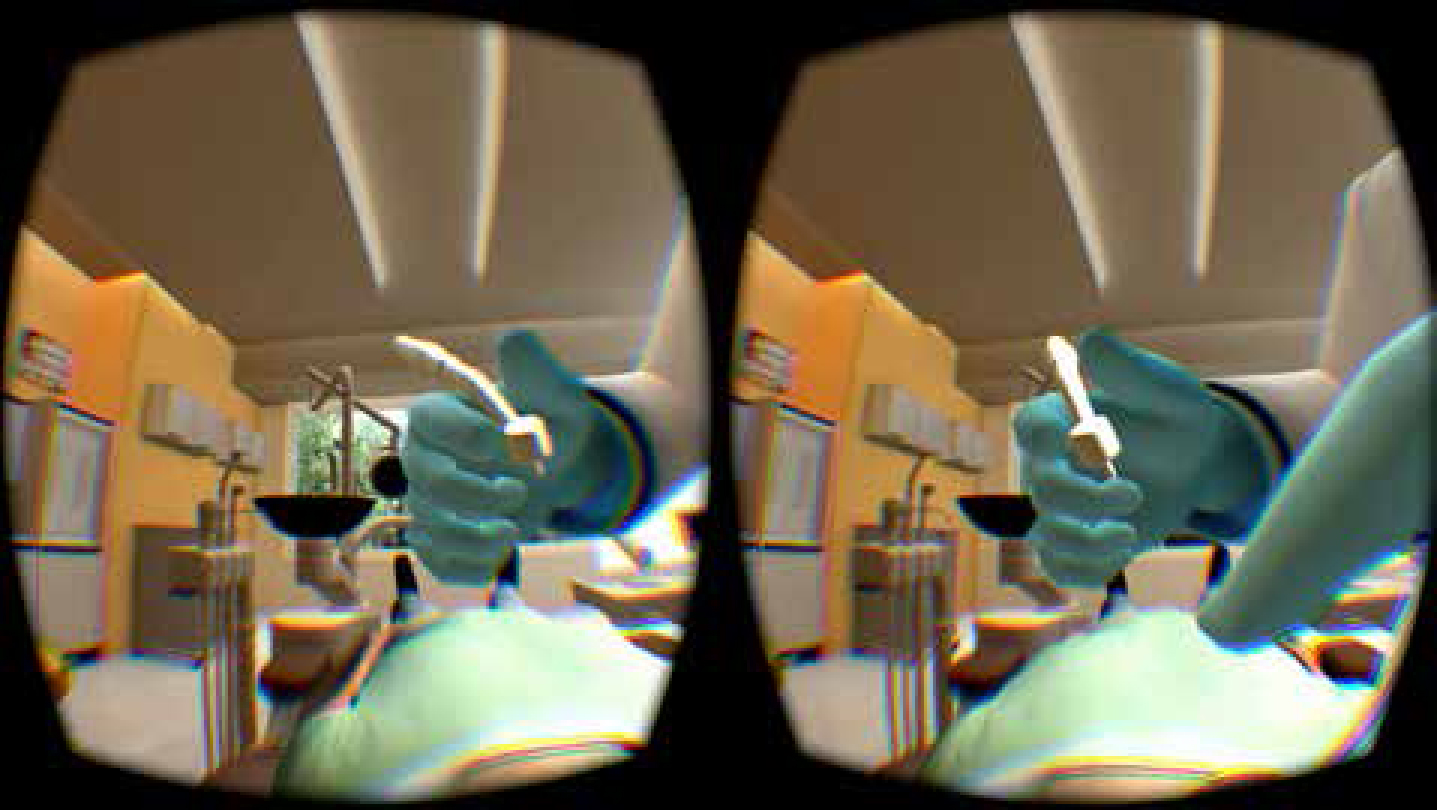
The introduction of drills without sounds – screen shot shown in Figure 4;
The introduction of drills with sounds – screen shot shown in Figure 4.
Figure 1. Screen shot of scenario 1 – sitting on the dental chair.Figure 2. Screen shot of scenario 2 – during examination of the oral cavity with mouth mirrors.Figure 3. Screen shot of scenario 3 – during introduction of the dental injection.Figure 4. Screenshot of scenarios 4 and 5 – during dental drill procedure.
Exposure to the above mentioned scenes was well-controlled.
Patients received the VRET in multiple sessions with different scenarios. They were asked to rate their current distress at the end of each exposure, using a Subjective Units of Distress Scale (SUDS). Each scenario sequence was repeated a number of times until a patient‧s distress decreased substantially before proceeding to the next scenario. The patients were encouraged to keep their mouths slightly open from scenario 2 through 5 and were instructed to follow the directions of the researcher. They were assured that their mouth would not be touched at any point during the VRET session. The patients were allowed to progress at their own pace. If the SUDS scores of the patient during exposure to any of the VR scenarios increased, the subsequent exposures were continued until the participant felt able to overcome the fearful stimuli as demonstrated by lower SUDS scores (≤3).
After the VR exposure session, the patients reported their state anxiety (VAS-A) and dental trait anxiety (MDAS and DFS) levels. They also rated their VR experience, intentions to undergo VRET in the future, and underwent a behaviour test to determine the extent of the patients' ability to confront dental situations immediately after VRET. The patients were offered the opportunity to return to the SEGi Oral Health Centre later and avail themselves of an actual dental procedure. They were not offered any incentive or discount for the dental treatment.
The patients' state anxiety level (VAS-A), and severity of dental trait anxiety (MDAS, and DFS) were assessed at baseline, immediately after VRET, after their first dental visit post VRET, and at 6 months follow-up. Also at 6 months follow-up, the phobia checklist was used to determine whether the patients fulfilled the criteria for dental phobia.
Measures
Subjective Units of Distress Scale (SUDS)
A SUDS29 was used to index the intensity of subjective distress currently experienced by the patients. It is used by therapists as a standard measure to evaluate the progress of exposure-based therapies. Typically, the patient is asked by the therapist: ‘On a scale of 0–10, where 0 is no discomfort and 10 is the worst discomfort you can experience, how much discomfort do you feel right now?’ For this article, the researcher recorded the SUDS scores during each exposure of the VRET session. Patients were moved to the next hierarchy level of VRET only when their current anxiety level was reduced to ≤3 SUDS score. Patients were not aware of this criterion. Each scenario was repeated until the anxiety decreased to the desired level (≤3) and only then was the next scenario introduced.
State anxiety
State anxiety level was determined utilizing the Visual Analogue Scale for Anxiety (VAS-A)30 at baseline, immediately following VRET, after their first dental visit and at 6 months post VRET. The VAS-A has been found to be a simple, sensitive, fast, reliable and valid tool to measure level of state anxiety.31
Dental trait anxiety
Severity of dental trait anxiety was measured using Modified Dental Anxiety Scale (MDAS)32 and Dental Fear Survey (DFS)33 at baseline, immediately after VRET, after their first dental visit and at 6 months post VRET. Possible MDAS scores range from 5 to 25, with greater scores indicating higher level of dental trait anxiety. The MDAS has shown high levels of internal consistency and good construct validity.34 Possible DFS scores range from 20 to 100, with greater scores indicating higher levels of dental anxiety. The DFS has established reliability, validity and sensitivity.35
Behaviour test
A behaviour test was conducted prior to, and immediately after, VRET based on the self-reported measure of the patients' level of discomfort to the contrived situation.36 The test was similar to the VRET scenarios, and provided a baseline behavioural assessment measure to compare the responses of the patient before and after the VRET. The test was similar to the one used by Doering et al37 and consisted of introducing five situations that usually occur during a dental visit:
Sitting in the dental chair;
Inspection of the oral cavity using two dental mirrors;
Showing the patient an approaching dental syringe;
Showing the patient an approaching dental drill without sound;
Showing the patient an approaching dental drill with sound.
Patients were asked by the observer to assess his/her level of anxiety on a scale of 0–10 in each situation37 during each of the aforementioned dental situations. This behaviour test was performed at baseline and after completion of VRET.
VR experience
Immediately after VRET, the patients rated the level of ‘presence’, ‘realism’ and ‘severity of nausea’ using 11-point verbal rating scales (VRS).38 Their intentions to undergo VRET in the future and to revisit the dental office for treatment were also measured using the 11-point VRS.39
Phobia checklist
The phobia checklist was used for the assessment of dental phobia in this article.4 This specific screening tool for measuring dental phobia has been validated against the Structured Clinical Interview for DSM-IV40 with a sensitivity of 0.95, specificity of 0.99, and an overall hit rate of 97%.4 The phobia checklist consists of four questions based on the DSM-IV-TR criteria41 for specific phobia. The patients are told to mark either a ‘YES’ or ‘NO’ response against the following questions related to their dental anxiety:
The sight of the feared object or experiencing the situation evokes an excessive fear response;
The fear is greater than justified;
Avoidance or giving up things because of the fear;
Avoidance of the situation or object causes daily impairment.
An individual is categorized as dental phobic only upon answering ‘YES’ against all four questions of the phobia checklist. In the present article, the checklist was administered during diagnostic interview and at 6 month follow-up. At diagnostic interview, both patients responded ‘YES’ against all the statements and hence were classified as dental phobic.
Results
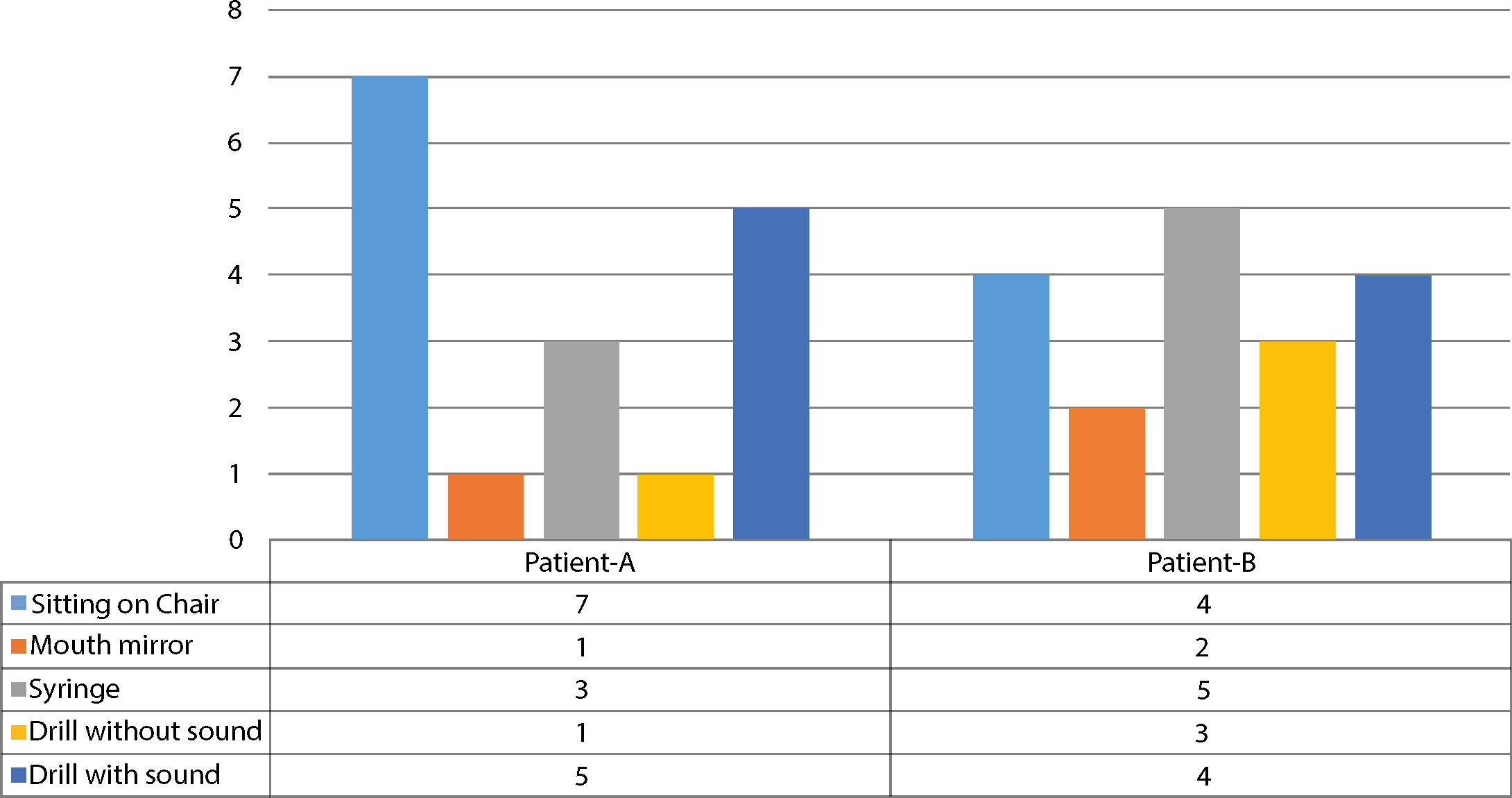
Patient A and B received VRET in a single appointment for a duration of 25 minutes and 20 minutes, respectively. Table 1 shows self-reported dental anxiety scores at different time points for both patients. The state anxiety (VAS-A) and dental trait anxiety (MDAS, DFS) scores showed a downward trend following VRET. The gains were maintained until follow-up of 6 months for both the patients. Table 2 shows reduction in behavioural test scores post-VRET. Figure 5 shows the number of VRET sessions that were required to reach SUDS of ≤3 with different VR scenarios for both the patients.
Figure 5. Number of VRET sessions that were required to reach SUDS ≤3 with different VR scenarios.
Measures
Patient-A
Patient-B
Baseline
Immediately after VRET
1st Dental Treatment after VRET
6 Months follow-up
Baseline
Immediately after VRET
1st Dental Treatment after VRET
6 Months follow-up
VAS-A
70
15
10
10
55
0
0
0
MDAS
21
13
8
7
17
7
7
7
DFS
71
25
34
32
65
35
26
23
Behaviour test
Patient-A
Patient-B
Pre-VRET
Post-VRET
Pre-VRET
Post-VRET
Sitting on the chair
6
2
6
1
Mouth mirror
5
3
7
1
Syringe
5
3
10
2
Drill with no sound
7
3
7
1
Drill with sound
7
3
7
2
Patients A and B rated the ‘presence’ they felt during VRET at 10 and 8, respectively. Both rated the ‘realism’ of the virtual world at 10. Patient A reported mild nausea after the VRET. When evaluated for their intentions to undergo VRET in the future, patient A indicated that there was ‘a good possibility’, and patient B indicated this to be ‘very probable’. Patient A indicated to be ‘almost sure’ and patient B to be ‘certain’ about revisiting the dental clinic again. Within 6 months after VRET, patient A underwent scaling, multiple fillings and crown placement at a private clinic, whereas patient B underwent scaling and multiple dental restorations. Upon evaluation at 6 months follow-up, both patients did not meet the criteria for dental phobia based upon the phobia checklist for dental phobia.
Discussion
To our knowledge, this article was the first to explore the applicability of VRET in the treatment of dental phobia. VRET resulted in a notable reduction of various self-reported dental anxiety scores. The treatment gains were maintained after having undergone a real dental treatment, and at six month follow-up. Both patients enjoyed the therapy and acknowledged that it had proved very useful to them in reducing their dental anxiety. Most importantly, their tendency to avoid dental treatment disappeared, and both of them were able to undergo dental procedures successfully within 6 months after receiving VRET. Notably, both patients no longer met the criteria for dental phobia at 6 months follow-up. Efficacious use of VRET in the treatment of dental anxiety as demonstrated in this article is comparable to its success in the treatment of other anxiety disorders, such as fear of enclosed spaces,18 fear of heights,19 fear of flying,20 and spider phobia.21
There are substantial limitations that relate to experimental methodology in general,42 hence we need to be cautious in interpreting the results. The study was conducted on only two female dental phobic patients. Furthermore, after VRET, the self-reported anxiety measures were not recorded during all dental visits but only after their first real dental visit and at 6 months follow-up. However, both the patients responded well to VRET. The approximate duration of the VRET session ranges from 20–150 minutes, based on the results of our pilot studies. From a practical point of view, one minor issue associated with the use of VR seems to be the occurrence of simulation sickness experienced by some patients. In the present case, patient A, who had not reported any history of simulation sickness, developed very mild nausea following VRET. The reason could be due to prolonged VR exposure for 25 minutes. To this end, it is important to note that, for VRET to be effective, the VR environment should make the patients ‘feel present’19,43 in the fear-provoking environment24 just as a realistic experience enables the patients to confront their anxiety-provoking stimuli.17 Although this has the potential disadvantage of inducing some simulation sickness, the positive effects of VRET on dental anxiety in this article could be attributed to high levels of presence and realism experienced by both the patients. There is evidence to suggest that simulation sickness can be prevented by administering VRET for less than 20 minutes or by giving breaks to the patient during the VRET sessions.38
An advantage of VRET is that it is flexible to use as the exposure scenarios can be stopped, paused, restarted and repeated whenever, and for as many times, as considered necessary.24 VRET for the treatment of dental phobia may not require any special training; a basic knowledge to operate the computer and to run the VRET software may be sufficient to administer VRET. The entire exposure process may be accomplished by a dental auxiliary using a computer in the safety and privacy of the practitioner‧s office.24 Moreover, it can be used in situations where in vivo exposure is considered risky for the patient.27 The results from this article seem to be promising. However, in order to establish the efficacy of VRET in the treatment of dental anxiety, these results are awaiting replication using carefully controlled trials.