Dawson PE., 4th edn. St Louis, Missouri: Mosby; 2007
Poyser NJ, Porter RWJ, Briggs PFA, Chana HS, Kelleher MGD. The Dahl Concept: past, present and future. Br Dent J. 2005; 198:669-676
, 3rd edn. London, UK: Faculty of General Dental Practice; 2013
Wassell R, Naru A, Steele J, Nohl F.London, UK: Quintessence Publishing Co Ltd; 2008
Cracking the cracked tooth code: detection and treatment of various longitudinal tooth fractures. Endodontics: Colleagues for Excellence. 1997; Fall-Winter:1-13
Geurtsen W. The cracked-tooth syndrome: clinical features and case reports. Int J Periodontics Restorative Dent. 1992; 12:395-405
Eliyas S, Jalili J, Martin N. Restoration of the root canal treated tooth. Br Dent J. 2015; 218:53-62
Lynch C, McConnell R. The cracked tooth syndrome. J Can Dent Assoc. 2002; 68:470-475
Ratcliff S, Becker I, Quinn L. Type and incidence of cracks in posterior teeth. J Prosthet Dent. 2001; 86:168-172
Brannstrom M, Astrom A. The hydrodynamics of dentine: its possible relation to dentinal pain. Int Dent J. 1972; 22:219-227
Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 1: aetiology and diagnosis. Br Dent J. 2010; 208:459-463
Banerji S, Mehta SB, Millar BJ. Cracked tooth syndrome. Part 2: restorative options for the management of cracked tooth syndrome. Br Dent J. 2010; 208:503-514
A growing problem in dentistry is complications associated with failing amalgam restorations that have been in place for many years. At present, there is a wide variety of treatment options available in the clinician's armamentarium when this situation arises, however, without the correct diagnosis, the prognosis for the tooth may quickly diminish, despite the clinician's best efforts. A confusing array of symptoms and failures may confound even the most experienced dentist, which will inevitably lead to invasive and time consuming approaches in a desperate attempt to rectify the initial problem. This paper, the first part of a three-part series, discusses the possible aetiological factors responsible for restoration failure, including occlusal issues and cracks within the tooth structure. The second part of the series will focus on restorative options and root-treated teeth. The third, and final, part of the series will provide an overview of the previous papers and conclude with a case report.
CPD/Clinical Relevance: Failure of amalgam restorations is a commonly encountered clinical problem in general practice and no one case presents in the same way. A competent diagnosis regarding the occlusion and tooth structure, followed with implementation of the most appropriate, minimally invasive treatment option, requires an adequate knowledge of current literature.
Article
Amalgam has served as an excellent and versatile dental restoration for over 100 years. Traditional preparation designs were initially proposed by GV Black in the mid-nineteenth century. Furthermore, the serial replacement of restorations by ever larger and more complex restorations, termed the ‘restorative cycle’, has made it common practice to see large amalgam restorations still functioning. However, no restorative solution is eternal and the clinician must be able to detect the early signs of failure before irreversible damage occurs. When a patient does present with a sudden onset of symptoms, the nature of the problem may elude the unsuspecting dentist. A successful outcome can be further complicated when numerous, heavily restored teeth are present on the same arch. It is vital that the clinician is aware of the differential diagnoses in order to avoid unnecessary and overly invasive treatment options which are condemned to failure because the underlying cause(s) was(were) overlooked.
This article will focus on occlusal trauma, incomplete fractures and endodontic complications. These issues are commonly associated with the failure of amalgam restorations and they can be easily misdiagnosed. It is important to mention the other main causes of amalgam failure, including secondary caries and restoration fracture, which the reader will already be well versed in treating on a day-to-day basis in practice or in hospital.
Occlusal trauma
The topic of occlusion is an area which may be confusing, however, this is an important issue which cannot be ignored. Pathological occlusal contacts can be associated with a wide range of clinical symptoms, including tooth discomfort and sensitivity. In the worst case scenario, misdiagnoses can lead to unnecessary and invasive procedures such as endodontic therapy and even extraction.
Aetiology
The inter-cuspal position (ICP) is never stable long-term, even during adulthood.1 This is due to the deteriorating effects of micro-organisms, microtrauma and physical injury. Consequently, wear, restorations, fixed/removable appliances and tooth loss may occur over time, with inevitable changes to the occlusal relationships. Damaging premature contacts, deflective contacts and interferences may occur, which can lead to overloading and trauma of the dentition. Importantly, if the vigilant clinician identifies the signs of occlusal trauma at an early stage, then the preceding symptoms, complications, repeated treatment failures, breakdown of the patient-clinician relationship and additional treatment costs, can all be avoided.
Damaging occlusal contacts can also be the consequence of operator error. These situations arise when the occlusion has not been planned prior to the commencement of treatment and the new occlusal scheme has occurred by accident; the worst occlusal scheme is the arbitrary occlusal scheme. The clinician must avoid this predicament by adopting either the conformative or re-organized approach. The Dahl Concept is another accepted approach with favourable reports in the literature; relative axial tooth movement is observed when a restoration or appliance is placed in supra-occlusion, thereby creating space without tooth preparation.2
Signs and symptoms
When evaluating a patient suspected of having occlusal trauma there are a number of clinical and radiographic signs that may be present. It is important to note that each patient will respond differently to the same type of occlusal insult and a holistic approach should be taken for each case to exclude other causes. Indications of a traumatic occlusion may include one or more of the following clinical or radiographic signs.
Clinical
Mobility (progressive) – primary or secondary occlusal trauma;
Persistent discomfort on eating;
Fremitus – tooth movement when occlusal contact occurs;
Occlusal prematurities and discrepancies;
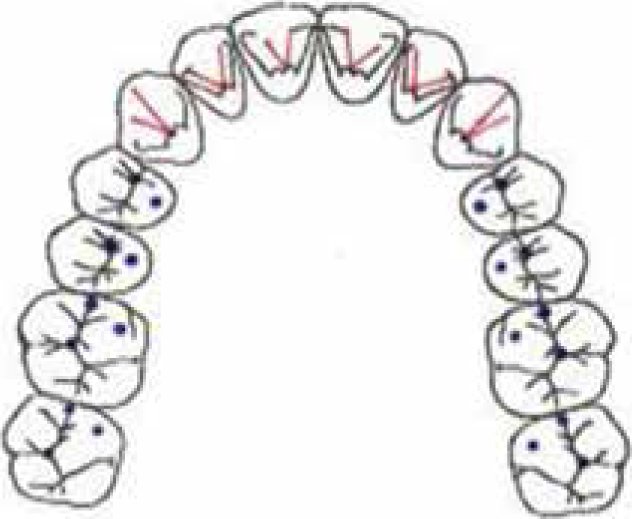
Toothwear facets and vertical enamel fracture lines – cracked teeth and fractured cusps are a feature of occlusal overload, especially where deflective contacts occur on heavily restored teeth. Fractures of the root may also occur (Figure 1);
Tooth migration and drifting – particularly where periodontal support is reduced;
Chipped or fractured restoration(s);
Repeated failure and decementation of restoration(s);
Thermal sensitivity and possible toothache – pulp hyperaemia, compression of the periodontal ligament (PDL) and abfraction lesions;
Abfraction lesions – V-shaped cervical notches;
A temporomandibular disorder (TMD) – highly debated topic outwith the scope of this article.
Figure 1. Following a series of extractions, the UR4 became a non-working side interference which resulted in an incomplete root fracture.
Radiographic
Widening of the PDL space;
Condensation and radiolucency of the alveolar bone or root resorption;
Funnelling of the PDL.
Diagnoses
Patient history evaluation and clinical assessment involving routine clinical examination, pulp-testing, radiographs and photographs. The FGDP 2013 guidelines advocate that a radiograph(s) should be taken to exclude pathology in heavily restored teeth.3
Occlusal examination must take place and it is vital to the overall treatment plan (Table 1).
Component of the Clinical Examination
Occlusal Examination and Clinical Signs which are an Indication of Occlusal Trauma
Inter-Cuspal Position (ICP)
Broad rubbing contacts can be indicative of occlusal issues compared with small and discrete markings.4Assess for Shimstock Holding contacts and carefully make a note of them. Ideally, there should be multiple and simultaneous contacts.There should be anteroposterior freedom in ICP to prevent overloading and avoid the sensation of a ‘locked’ occlusion.Empty mouth clenching, aka ‘the clench test’, can help identify an occlusal cause for the pain.1
Retruded Contact Position (RCP)
Assess for a premature deflective contact in CR, termed RCP, and make a note of the teeth.
The RCP–ICP Slide
Approximate the direction and distance of the slide, including whether the movement is predominantly horizontal or vertical.Note any signs of trauma to the teeth involved in the slide or to the anterior teeth, aka ‘the anterior thrust’.4
Excursive Movements
Take note of any non-working and working side interferences.Assess for any posterior interferences during protrusion.Canine and group function are both accepted lateral movements.
Muscles
This includes palpation of the: temporalis, lateral pterygoid, digastric, masseter, shoulder, neck, trapezius and sternomastoid muscles.
Temporomandibular Joint
Examination includes:Range of movement.Palpation of the joint – ideally assessed using a stethoscope.Assessment for joint sounds – clicking or crepitus.
It is vital to remove the causative factor(s) resulting in occlusal trauma. This will allow normal adaptive responses to initiate, with a return to comfort and reduced mobility.1 The methods of managing traumatic occlusion include:
Prolonged splint therapy – required when TMD is present, for assessment of centric relation and those with signs of sleep bruxism;
Orthodontics – this may also include surgery;
Occlusal adjustment – alteration of the occluding surfaces of the teeth or restorations. This is usually appropriate for heavy occlusal loading of a single tooth with relevant signs and symptoms;4
Occlusal equilibration – modifications are made to the occlusal surfaces of multiple teeth in order to equalize stress and achieve even occlusal contacts, with the aim of achieving a ‘perfected’ occlusion (Figure 2);
For complex cases, such as occlusal equilibration, it is recommended that study models are mounted on a semi-adjustable articular to assist with treatment planning, trial adjustments and diagnostic wax-ups (Figure 3).
Figure 3. Articulated wax-up model of the upper anteriors.
It should be noted that additional treatment(s) may also be required if damage to the tooth and/or surrounding structures has occurred. For example, periodontitis will be exacerbated by occlusal trauma (secondary occlusal trauma). Therefore, periodontal and occlusal treatments must occur for a successful outcome.
The cracked tooth
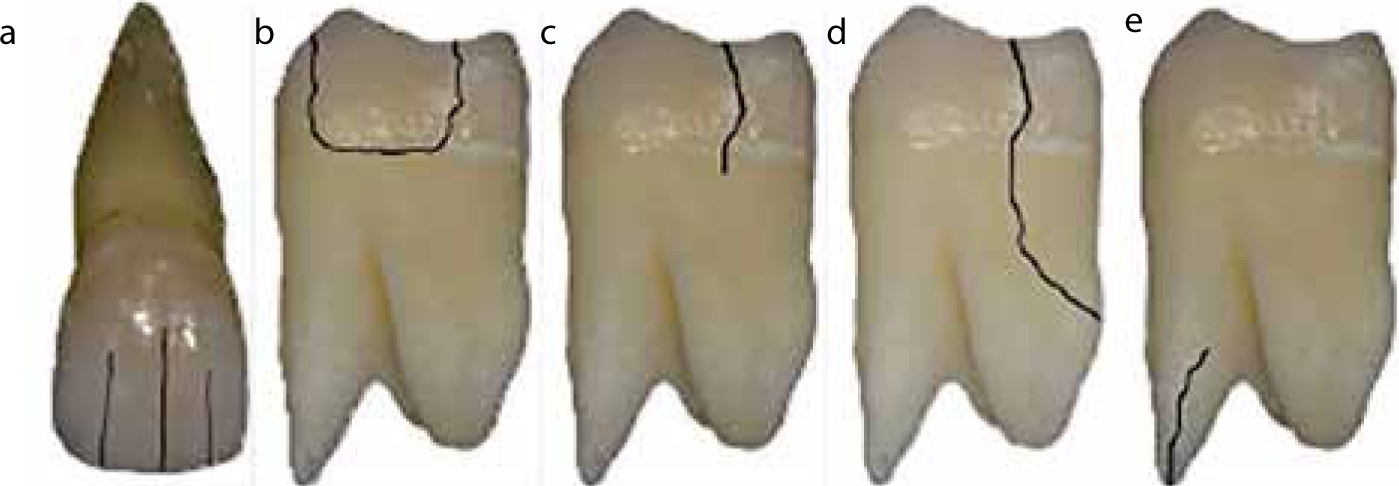
Numerous terms have been used over the years to describe cracks in teeth including, ‘cracked tooth syndrome’, ‘cracked cusp syndrome’ and ‘split tooth syndrome’. However, the term ‘syndrome’ is misleading as this infers that a crack is a disease process, which is clearly inappropriate. Therefore, to reduce confusion regarding this subject, the American Association of Endodontists5 proposed five types of tooth cracks, which will form the basis of classification within this paper.
Craze lines – asymptomatic as the fracture is contained within enamel (Figure 4a);
Fractured cusp – complete or incomplete fracture extending to the cervical third or the root surface (Figure 4b). The pulp is normally vital, with mild symptoms on biting and to cold;
Cracked tooth – incomplete ‘green-stick’ fracture which usually extends mesio-distally, but may also run bucco-lingually in mandibular molar teeth (Figure 4c).
Split tooth – the end result of a cracked tooth, which normally has a poor prognosis as the tooth is split into two separate fragments (Figure 4d). The tooth has often been root-filled and the patient normally complains of marked pain whilst chewing, particularly on one cusp.
Vertical root fracture – crack initiated at the root level, usually in a bucco-lingual direction. The crack may be complete or incomplete and almost all cases have a history of root canal treatment. Symptoms are vague and may mimic periodontal disease or failed root canal treatment (RCT). Root resection or hemi-section are potential treatment options in multi-rooted teeth (Figure 4e).
Figure 4.
(a–e) AAE5 classification of crack formations within teeth.
Aetiology of cracks
Although enamel has a low tensile strength and is brittle, it has a high modulus of elasticity and this, together with the support of the dentine-enamel junction, minimizes the possibility of fracture.6 Cracked teeth are generally more prevalent in adults, typically in the age range of 30–50 years, which is thought to be related to reduced dentine elasticity and increased fatigue.
The aetiology of incomplete fractures of enamel and dentine is multi-factorial in nature. A paper by Geurtsen demonstrated that cracks can be the result of abnormally high forces on structurally healthy teeth or normal physiologic forces on weakened teeth7 (Figure 5).
Figure 5. Split tooth UL6 which has occurred due to the size of the amalgam restoration weakening the tooth structure and high masticatory forces. The tooth is now unrestorable.
Healthy teeth
Incomplete fractures in healthy, unrestored teeth are less common and it is thought to occur only under specific circumstances where excessive forces are applied, including:
Parafunctional habits;
Trauma – contact sports, including a fall or blow to the face;
Masticatory accident – the patient bites on an unexpectedly hard food particle with unrestricted force.
Weakened teeth
Crack formation is evident in restored teeth, where normal cyclic contact stresses induce fatigue and facilitate incomplete fracturing.7 It is thought that micro-cracks form as a result of cuspal flexure and repeated thermal expansion of the restorative materials.
Moreover, endodontic treatment has been implicated in crack formation due to the necessary requirements of an adequate access cavity, which will inevitably impact the stiffness of the remaining coronal tooth structure (see later).8
In this regard, Lynch and McConnell9 subdivided cracks into four causative categories, namely: restorative, occlusal, developmental and miscellaneous. A good understanding of these factors (Table 2) will simplify diagnoses for the clinician as he/she will be aware of the high risk scenarios.
Classification
Factors
Restorative Procedures
Teeth with restorations are 29 times more likely to develop cracks9Loss of both marginal ridges, as cuspal strength is reduced by 63%9Cavity preparation >1/2 of the tooth widthDentine pinsImproper composite placement, ie non-incrementalHydraulic pressure of tight cast restorationsPoorly designed castingsDeep cusp-fossa anatomyOverzealous cavity preparation
Occlusal Factors
Masticatory ratio of force regarding the molars, premolars and incisors is 4:2:1.Therefore, much higher forces are applied to posterior teeth located close to the TMJs. This would explain why the incidence of cracked teeth occurs in the order: Mandibular second molars;Mandibular first molars;Maxillary premolars;Maxillary molars;Mandibular premolars.Additionally, it is thought that the maxillary palatal cusps act as plungers, resulting in a wedging effect with structural fatigue of the mandibular molars. If the teeth are involved in excursive interferences or parafunctional habits exist, the risk of fracture is increased.10Masticatory accidents (as already discussed).
Developmental Conditions
Structural weaknesses within the tooth which occurred during the formation.
Miscellaneous Factors
Intra-oral piercingsErosive toothwearCracking and crazing formation as a result of the high-speed handpiece Internal resorption
Signs and symptoms
Symptoms are variable depending on the extension of the crack with relation to the underlying pulp chamber, which determines the overall tooth vitality. Therefore, a complete fracture into the pulp chamber will give the symptoms of irreversible pulpitis, pulp necrosis or apical periodontitis. Even an acute apical abscess, with or without swelling or a draining sinus tract, may be present if the pulp has undergone necrosis.
Cracked teeth are characterized by sharp pain during mastication which increases as the occlusal force is raised. This is caused by a movement of dentinal tubular fluid flow due to movement of the fracture sites, stimulating odontoblasts within the pulp as well as stretching and rupturing odontoblastic processes within the dentinal tubules.9,11 The common signs and symptoms are listed in Table 3.
Sudden, sharp pain on biting/chewing and in some cases on release, termed ‘rebound pain’
Sensitivity to cold thermal stimuli; hyper-reactivity to hot and sugary stimuli may also occur
Symptoms may be present for periods ranging from weeks to months
Inconsistent ability to localize the affected tooth
Pain may be elicited by lateral cusp pressure, as evoked by ‘bite tests’ and tooth grinding
Fracture lines may be seen clinically or following removal of the restoration
Positive response to pulp tests, but with an exaggerated response to cold thermal stimuli
Radiographs are normally inconclusive
Diagnoses
Correct diagnoses can be very challenging and time consuming, as cracked teeth can mimic symptoms arising from other dental conditions including, but not limited to, acute periodontitis, dentine hypersensitivity, occlusal trauma and atypical oro-facial pain.
Following careful history-taking, the clinical examination should take place with the aid of the following.
Visual inspection
Magnification (dental loupes/microscope) and a good light source are strongly recommended.
Removal of restorations
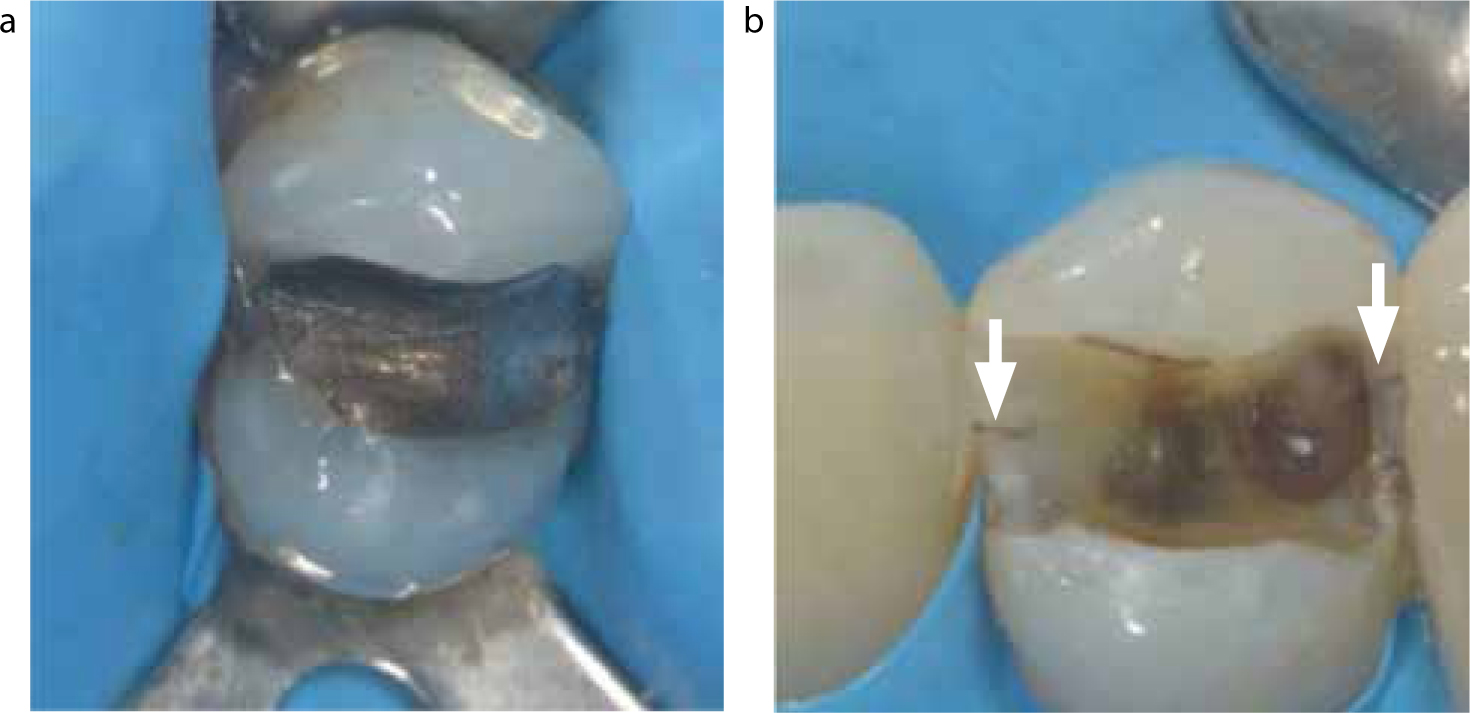
Removal of the old restoration allows for visualization of underlying fracture lines and exploration of the cavity floor (Figure 6).
Figure 6.
(a, b) A cracked tooth diagnosis is confirmed following removal of the amalgam restoration UR4.
Stabilization
Stainless steel orthodontic bands are a useful method of preventing further crack propagation, whilst aiding the diagnosis. If a fracture line is present then the symptoms should resolve within 2–4 weeks following cementation. If symptoms persist then root canal treatment is indicated for the cracked tooth, or the provisional diagnosis was incorrect.
Tactile sensation
A straight probe explorer may catch the crack on the tip of the instrument and may evoke sharp pain, confirming a cracked tooth.
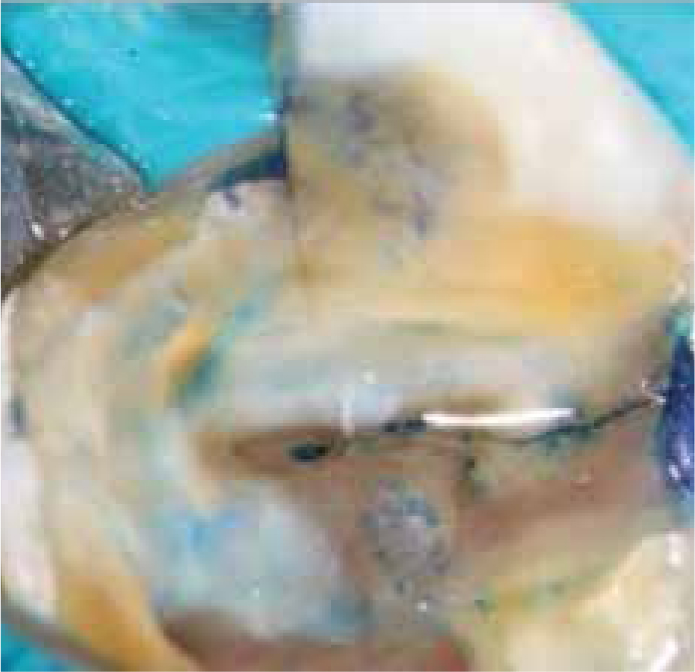
Dye test
Gentian Violet or Methylene Blue stains can be used to highlight cracks. This is a more time consuming method as the dye has to be sealed in the cavity for 2–5 days to take full effect (Figure 7).13
Figure 7. Methylene blue stain demonstrating the fracture line.
Transillumination
This is a very useful aid to assist the diagnosis of an incomplete crack. A standard composite light-curing unit is placed against the tooth and the light transmission will be blocked by the presence of a crack line (Figure 8).
Figure 8. Transillumination demonstrating fracture line on the lingual cusp.
Probing and percussion
Cracked teeth are rarely tender to percussion.
Detection of an isolated pocket distinguishes a cracked tooth from a split tooth.
Pulp test
Heat, cold and electric pulp tests; sometimes there is an exaggerated response to cold due to pulpal inflammation.
Bite test
This normally involves a Tooth Slooth (Professional Results Inc, Laguna Niguel, CA), cotton roll, wooden stick or a rubber plunger from anaesthetic cartridges. The Tooth Slooth will provide the most accuracy but, when this is not available, cotton wool can be a useful alternative with the patient biting down for five seconds before release. The aim is to mimic the symptoms and identify the location of the crack.
Cracks are normally orientated in a mesio-distal direction through the marginal ridges, however, they may also run bucco-lingually in mandibular molar teeth.5 Therefore, these sites should be inspected upon examination. Early identification is important to limit the crack growth with subsequent involvement of the pulp, periodontal tissues and catastrophic fracture.
Radiographs
Radiographs are an unreliable method for diagnoses of cracked teeth (Figure 9). This is because fracture lines are normally incomplete or run in a mesio-distal direction; even when a crack runs in a bucco-lingual direction it is not usually visible. Noticeable changes are only seen once the condition worsens and either the periodontal ligament or pulp becomes involved.
Figure 9. Pre-operative peri-apical radiograph of the split tooth UL6 shown earlier (Figure 5), prior to restoration removal. Note that there are no indications of the fracture.
Treatment
Immediate approaches for management of the cracked tooth depends on the location of the crack. Importantly, if pulpal involvement, other than reversible pulpits, is confirmed at the initial appointment then pulp extirpation should also be commenced.
Peripherally located cracks
Remove the compromised segment of tooth, such as for an incomplete fractured cusp, and restore as appropriate.
Centrally located cracks
Treatment options include:
Immobilization of the crack – a temporary crown is normally used, however, this is a highly destructive and time consuming approach;
Occlusal adjustment – destructive approach and only a temporary solution due to alveolar compensation.
Interestingly, Banerji et al13 outlined the concept of ‘direct composite splint’ (DCS). A 1.5 mm thickness of resin composite is bonded onto the entire occlusal surface of the tooth, thereby immobilizing the fractured segments. This can be performed without any tooth preparation, therefore it is a non-invasive, cost and time effective procedure which can be adopted in any general practice setting. Additionally, the DCS incorporates the Dahl Concept, where controlled intrusion and extrusion creates space for any definitive restoration. This, in the author's opinion, is the most appropriate treatment option at an emergency appointment as it satisfies the main issues: lack of time, confirms the diagnoses at subsequent review appointments and alleviates the patient's symptoms.
In the worst case scenario, the tooth is of a hopeless prognosis. If the crack extends into the root and below the level of the alveolar bone, or mobility of the separated fragments is evident (split tooth), then the tooth is deemed unrestorable. In these circumstances, extraction is indicated and the residual space can be restored, if necessary, with an implant, bridge or denture appliance.
Conclusions
The correct diagnoses of occlusal trauma and a cracked tooth may be easily overlooked if the relevant signs and symptoms are not recognized and the appropriate diagnostic tests are not performed. Importantly, it should be recognized that both diagnoses may even be identified in the same tooth at the same time, as occlusal trauma can initiate structural fatigue and crack formation. If the clinician is in any doubt, but strongly suspects a fracture, then it is recommended to place a DCS which will confirm the diagnoses whilst avoiding the risk of an unrestorable failure of the tooth between appointments. Attempts at heroic dentistry should be avoided and a realistic prognosis must be considered, accounting for patient time, health and finances. It is the mark of a good clinician to do everything in his/her power to save a tooth, but knowing when to accept a loss.