Stockholm: European Centre for Disease Prevention and Control; 2015
Unemo M, Nicholas RA. Emergence of multidrug-resistant, extensively drug-resistant and untreatable gonorrhea. Future Microbiol. 2012; 7:1401-1422
de Kraker ME, Davey PG, Grundmann H Mortality and hospital stay associated with resistant Staphylococcus aureus and Escherichia coli bacteremia: estimating the burden of antibiotic resistance in Europe. PLoS Med. 2011; 8
Laxminarayan R, Duse A, Wattal C, Zaidi AK, Wertheim HF, Sumpradit N Antibiotic resistance – the need for global solutions. Lancet Infect Dis. 2013; 13:1057-1098
Smith R, Coast J. The true cost of antimicrobial resistance. Br Med J. 2013; 346
Roca I, Akova M, Baquero F, Carlet J, Cavaleri M, Coenen S The global threat of antimicrobial resistance: science for intervention. New Microbes New Infect. 2015; 6:22-29
Costelloe C, Metcalfe C, Lovering A, Mant D, Hay A. Effect of antibiotic prescribing in primary care on antimicrobial resistance in individual patients: systematic review and meta-analysis. Br Med J. 2010; 340
Vellinga A, Murphy AW, Hanahoe B, Bennett K, Cormican M. A multilevel analysis of trimethoprim and ciprofloxacin prescribing and resistance of uropathogenic Escherichia coli in general practice. J Antimicrob Chemother. 2010; 65:1514-1520
Goossens H, Ferech M, Vander Stichele R, Elseviers M Outpatient antibiotic use in Europe and association with resistance: a cross-national database study. The Lancet. 2005; 365:579-587
Outterson K, Powers JH, Seoane-Vazquez E, Rodriguez-Monguio R, Kesselheim AS. Approval and withdrawal of new antibiotics and other antiinfectives in the US, 1980–2009. J Law Med Ethics. 2013; 41:688-696
Leeds: Health and Social Care Information Centre; 2015
Kuriyama T, Absi EG, Williams DW, Lewis MA. An outcome audit of the treatment of acute dentoalveolar infection: impact of penicillin resistance. Br Dent J. 2005; 198:759-763
Leeds: The Information Centre for Health and Social Care; 2008
Levy SB, Marshall B. Antibacterial resistance worldwide: causes, challenges and responses. Nat Med. 2004; 10:S122-S129
Sedgley CM, Lee EH, Martin MJ, Flannagan SE. Antibiotic resistance gene transfer between Streptococcus gordonii and Enterococcus faecalis in root canals of teeth ex vivo. J Endod. 2008; 34:570-574
Kuriyama T, Karasawa T, Williams DW, Nakagawa K, Yamamoto E. An increased prevalence of β-lactamase-positive isolates in Japanese patients with dentoalveolar infection. J Antimicrob Chemother. 2006; 58:708-709
Lewis MAO, MacFarlane TW, McGowan DA. Antibiotic susceptibilities of bacteria isolated from acute dentoalveolar abscesses. J Antimicrob Chemother. 1989; 23:69-77
Robertson D, Smith AJ. The microbiology of the acute dental abscess. J Med Microbiol. 2009; 58:155-162
Kuriyama T, Nakagawa K, Karasawa T, Saiki Y, Yamamoto E, Nakamura S. Past administration of beta-lactam antibiotics and increase in the emergence of beta-lactamase-producing bacteria in patients with orofacial odontogenic infections. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 89:186-192
Chate RAC, White S, Hale LRO, Howat AP, Bottomley J, Barnet-Lamb J The impact of clinical audit on antibiotic prescribing in general dental practice. Br Dent J. 2006; 201:635-641
Seppanen L, Lemberg KK, Lauhio A, Lindqvist C, Rautemaa R. Is dental treatment of an infected tooth a risk factor for locally invasive spread of infection?. J Oral Maxillofac Surg. 2011; 69:986-993
Cope A, Francis N, Wood F, Mann MK, Chestnutt IG. Systemic antibiotics for symptomatic apical periodontitis and acute apical abscess in adults. Cochrane Database Syst Rev. 2014; 6
Fedorowicz Z, van ZEJ, Farman AG, Agnithotry A, Al-Langawi JH. Antibiotic use for irreversible pulpitis. Cochrane Database Syst Rev. 2013; 12
Palmer NA, Dailey YM, Martin MV. Can audit improve antibiotic prescribing in general dental practice?. Br Dent J. 2001; 191:253-255
Palmer NAO, Dailey YM. General dental practitioners' experiences of a collaborative clinical audit on antibiotic prescribing: a qualitative study. Br Dent J. 2002; 193:46-49
Burke FJ, McCord JF, Cheung SW. The provision of emergency dental care by general dental practitioners in an urban area. Dent Update. 1994; 21:184-186
Martin MV, Longman LP, Hill JB, Hardy P. Acute dentoalveolar infections: an investigation of the duration of antibiotic therapy. Br Dent J. 1997; 183:135-137
The increasing emergence of antibiotic resistance is a major international public health problem. As a consequence, it is essential that steps are taken to conserve the effectiveness of existing antimicrobial agents. Consumption of antibiotics is the prime contributor to the development of resistance. General dental practitioners write almost 1 out of 10 prescriptions for antibiotics in primary care within the UK and therefore the prudent prescribing of antibiotics in dentistry has never been more vital. This paper outlines the impact of antimicrobial resistance on modern healthcare, describes the current use of antibiotics in general dental practice, and recommends pragmatic ways in which dental practitioners can evaluate and optimize their prescribing.
CPD/Clinical Relevance: Dental professionals have a responsibility to both their patients and the wider community to prescribe antibiotics appropriately.
Article
The ability to treat infectious diseases safely and effectively has medically, socially and economically revolutionized the 20th Century. Life expectancy in 1927, the year before penicillin was discovered, was 57 years for men and 61 years for women.1 The life expectancy of individuals born in 2012 has increased by over 20 years, to 79 years for men and 83 years for women.2 One of the principal reasons that people are living longer is a dramatic improvement in healthcare, specifically the ability to control infectious diseases using antimicrobial agents. However, there is now worldwide concern that the increasing emergence of antibiotic resistance may render these ‘wonder-drugs’ ineffective, transporting healthcare back to the pre-antibiotic era.
Public health problems associated with antimicrobial resistance
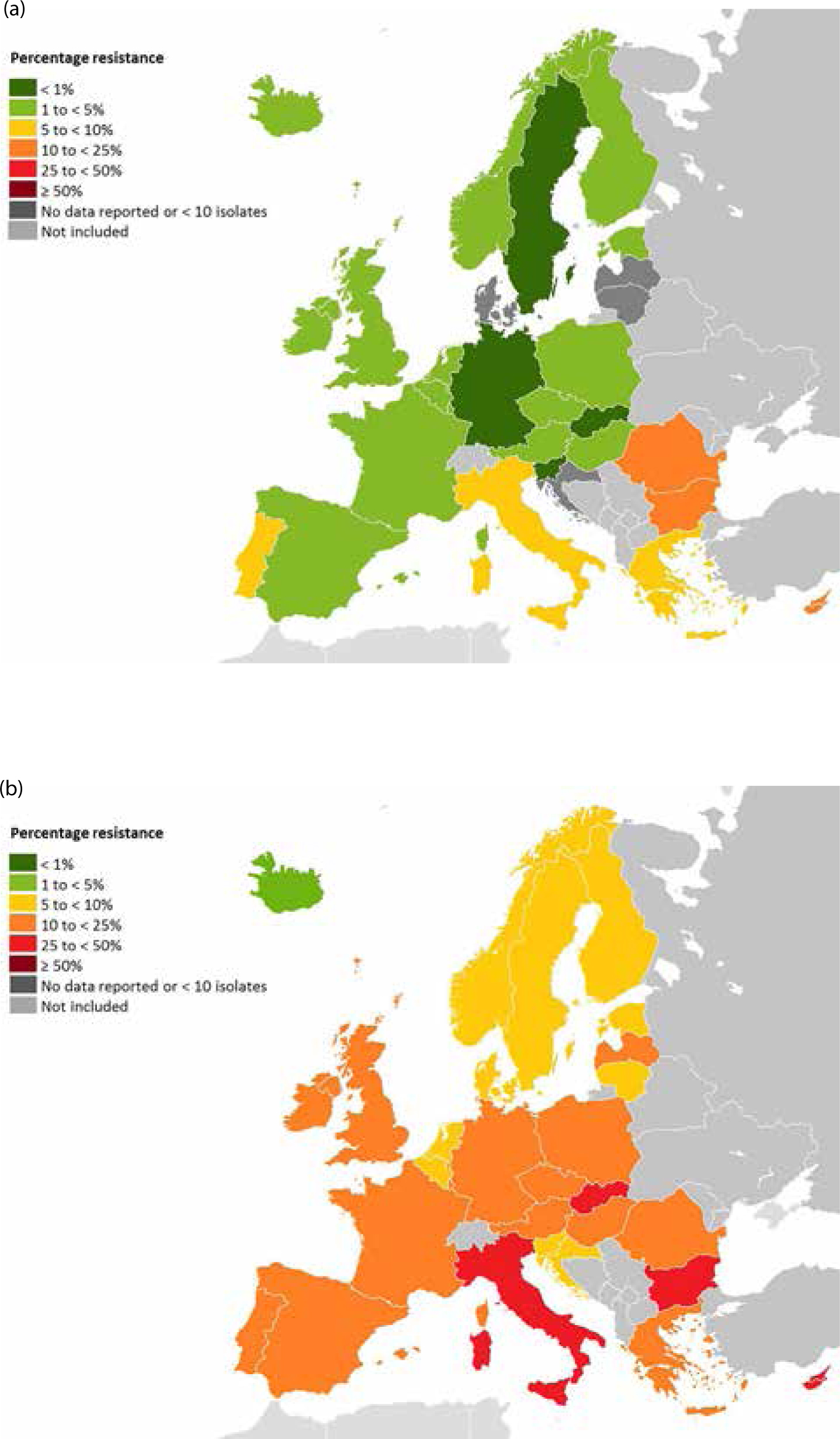
Antimicrobial resistance is the ability of micro-organisms, such as bacteria, fungi and viruses, to resist the action of an antimicrobial agent.3 Resistance is not a new phenomenon; soon after his discovery of penicillin Alexander Fleming delivered a stark warning about the potential consequences of abusing antibiotics. In his 1945 Nobel Lecture, Fleming spoke about the ability of microbes to develop or acquire resistance to penicillin, and how resistant bacterial strains could be spread between individuals with potentially fatal outcomes.4 During the subsequent four decades, the problem of antimicrobial resistance did not go away, but was largely masked or ignored due to the spectrum of new antimicrobial agents becoming available clinically. However, the situation changed during the 1980s when the incidence of bacterial resistance was still increasing but the previously plentiful supply of new antimicrobial drugs was reducing. Since the 1980s, the number of new antibiotics approved for use has fallen dramatically (Figure 1), yet the proportion of bacterial isolates demonstrating resistance to frequently used antibiotics has increased (Figure 2).
Figure 1. Food and Drug Administration (FDA) (USA) approvals of new systemic antibiotics (not withdrawn and subsequently withdrawn), 1983–2012. Sources: Boucher HW, Talbot GH, Bradley JS et al. Bad bugs, no drugs: no ESKAPE! An update from the Infectious Diseases Society of America. Clin Infect Dis 2009; 48: 1–12; Boucher HW, Talbot GH, Benjamin DK et al. 10 x ‘20 Progress – development of new drugs active against Gram-negative bacilli: an update from the Infectious Diseases Society of America. Clin Infect Dis 2013; 56: 1685–1694; Outters on K, Powers JH, Seoane-Vazquez E et al. Approval and withdrawal of new antibiotics and other antiinfectives in the US, 1980–2009. J Law Med Ethics 2013; 41: 688–696.Figure 2. Proportion of E.coli isolates resistant to third generation cephalosporins in Europe: (a) 2003 (b) 2013. Source: European Centre for Disease Prevention and Control ecdc.europa.eu/en/healthtopics/antimicrobial_resistance/database/Pages/map_reports.aspx
With the increasing emergence of resistant bacterial strains, infections are becoming progressively more difficult to manage. Already the treatment options for patients who are infected with multidrug-resistant bacteria are limited to a few remaining last-line antimicrobials, such as the carbapenems.5 In addition, widespread infections, in particular sexually transmitted diseases (STDs), are increasingly becoming refractory to first-line treatment. Traditionally, gonorrhoea could be effectively managed by a single high dose of penicillin. However, in recent years there has been the emergence of multidrug-resistant N. gonorrhoeae strains, and experts are now warning that the era of untreatable disease is near, representing a serious threat to public health.6
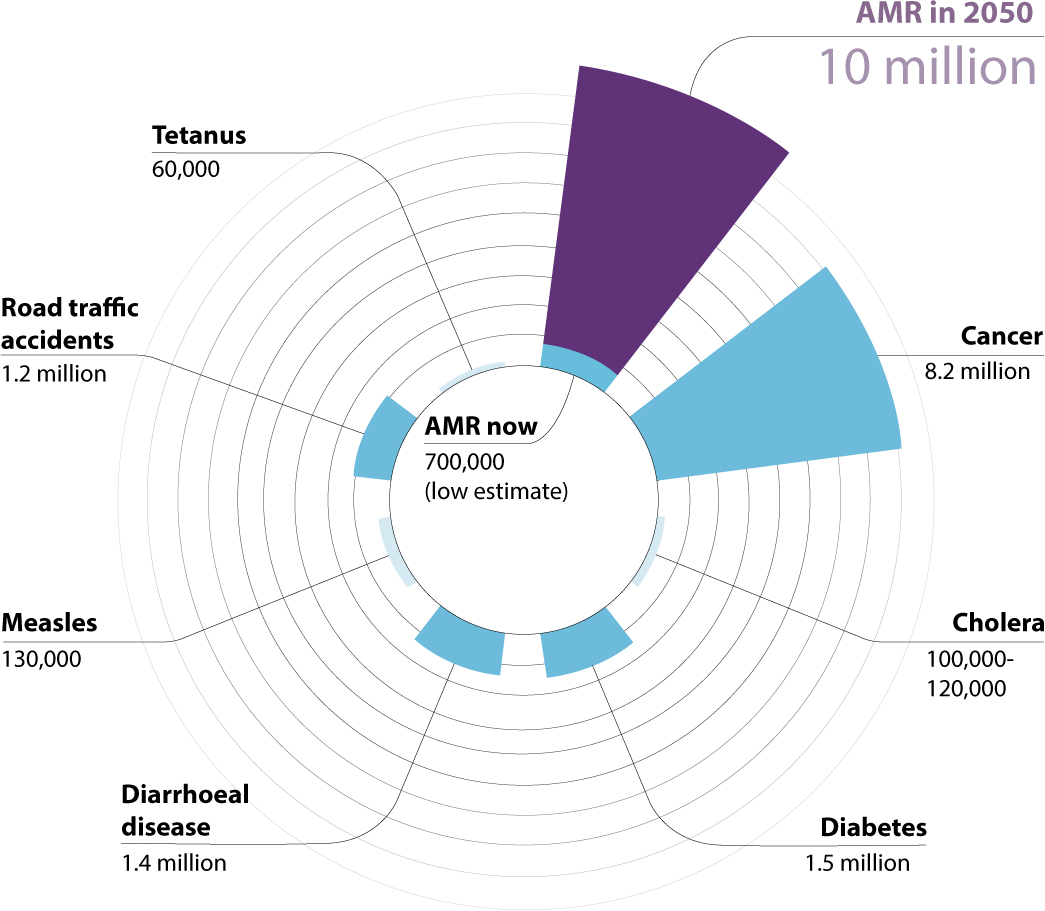
Infections involving resistant bacteria are not only more difficult to treat than those caused by sensitive strains, but they often result in patients spending longer periods of time in hospital. The cost associated with prolonged treatment is higher and patients have a greater likelihood of dying from their infection.7 In Europe in 2007, bloodstream infections (bacteraemia) caused by methicillin-resistant Staphylococcus aureus (MRSA) were associated with 5,500 potentially avoidable deaths and over 255,000 extra hospital days.7 The total inpatient costs alone were €44 million, not considering additional outpatient costs and productivity losses.7 Furthermore, excess morbidity and mortality associated with antibiotic resistant infections is projected to increase in the future and it has been estimated that, by the year 2050, resistant infections may be responsible for 10 million deaths worldwide (Figure 3).8
Figure 3. Comparative deaths from antimicrobial resistance (AMR) and other causes, 2050 (pro-jected). Source: Review on Antimicrobial Resistance. https://amr-review.org/sites/default/files/December%20report%20-%20comparative%20deaths.jpg
An additional consequence of escalating rates of resistance relates to the reliance on antibiotic therapy to facilitate other, now routine, medical or surgical interventions, such as chemotherapy, surgical procedures and solid organ transplantation.9 There is concern that, as resistance increases, even everyday operations may be impossible due to the risk of infection. The authors of a study published in 2013 estimated that, without antimicrobials, the rate of post-operative infection from a hip replacement would be between 40–50%, and that up to 30% of individuals who develop an infection would subsequently die.10 If this scenario becomes reality then a reduction in the number of hip replacements performed would in turn result in an increase in patient morbidity from musculoskeletal pain.10
Mechanisms of antimicrobial resistance
Antibiotic resistance arises due to mutations in the genetic code of a bacterium. This can either occur as a spontaneous mutation or following the acquisition of genetic elements conferring resistance. Whilst the emergence of resistant micro-organisms would occur irrespective of the presence of antimicrobial agents, exposure to these drugs provides the necessary selective pressure for the emergence and spread of resistant pathogens.9 Resistance genes then pass between bacterial species, facilitated by poor hygiene practices, interpersonal contact and worldwide travel. The use of antimicrobial agents, whether this is in patients, livestock, or the environment is therefore the driving force behind the increasing emergence of resistance and the resultant public health threat.11
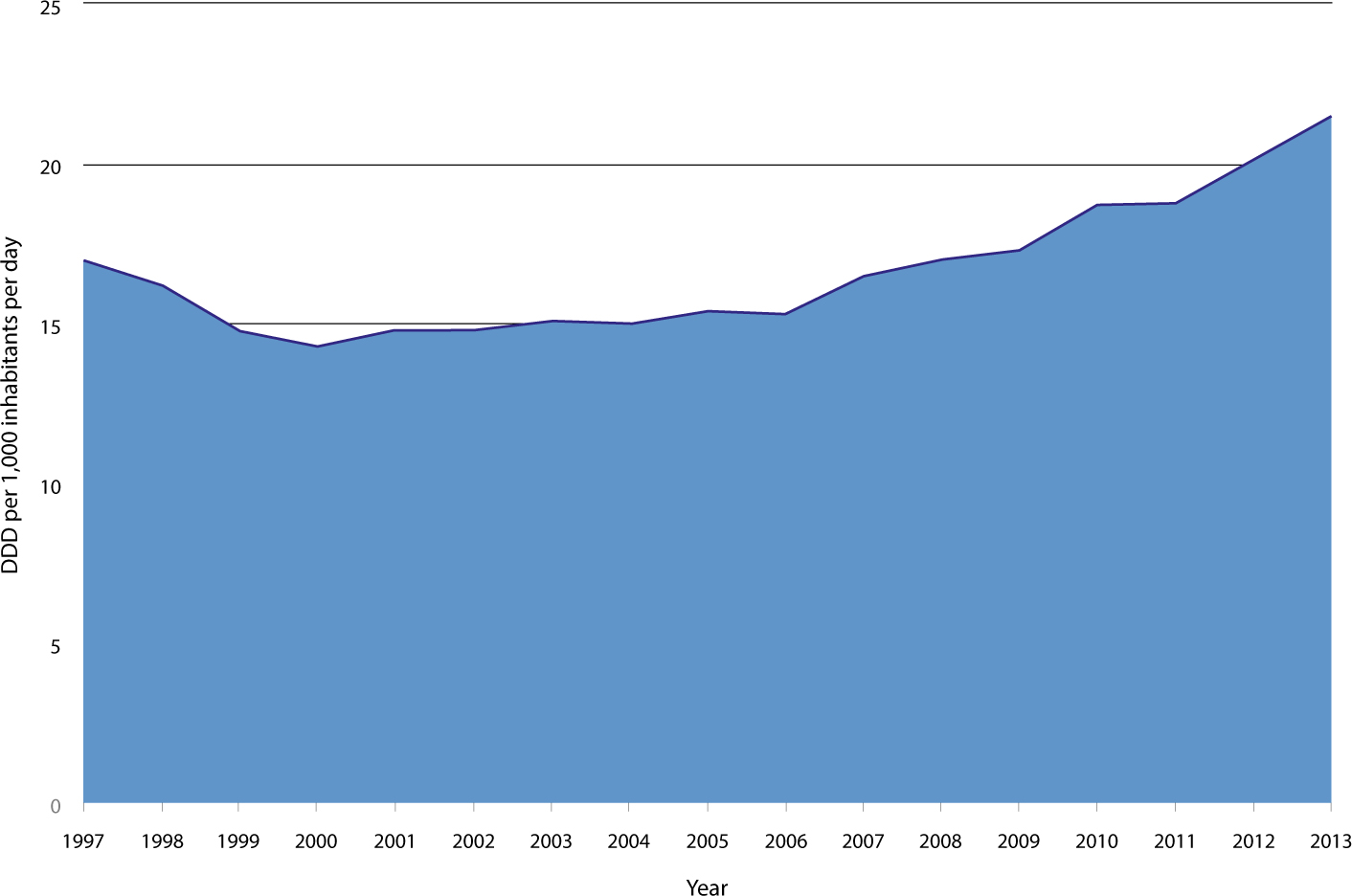
An association between antibiotic use and resistance has been demonstrated at the individual,12 community13 and country level.14 However, despite concern about antimicrobial resistance, worldwide antibiotic consumption is on the rise, particularly in developing countries where infectious diseases are widespread and antibiotics are freely available to buy over-the-counter.9 Even in the UK, where there is widespread awareness of the public health problems associated with resistance, prescription of antibiotics in primary care increased by 42% between 2003 and 2013, as demonstrated by an increase in Defined Daily Doses (DDD) of 15.1 per 1,000 people per day to 21.5 per 1,000 people per day15 (Figure 4). Furthermore, during the same period there has also been a change in the type of antibiotics prescribed; prescriptions of broad spectrum agents have become more frequent, while narrow spectrum antibiotics are being prescribed less often.16 This change in prescribing pattern is of particular concern since broad-spectrum agents are more likely to predispose to the selection of resistant strains than antibiotics that have a narrow range of activity.
Figure 4. Consumption of systemic antibiotics in primary care in the United Kingdom, 1997–2013. DDD, Defined Daily Doses. Source: European Centre for Disease Prevention and Control ecdc.europa.eu/en/healthtopics/antimicrobial_resistance/esac-net-database/Pages/trend-consumption-by-country.aspx#sthash.6CEyOQuF.dpuf
As awareness of antimicrobial resistance has increased, so too have calls for national and international efforts to slow its development. In May 2015, the World Health Organization submitted its Global Action Plan for Antimicrobial Resistance to the 68th World Health Assembly.17 The plan set out five strategic objectives:
To improve awareness and understanding of antimicrobial resistance;
To strengthen knowledge through surveillance and research;
To reduce the incidence of infection;
To optimize the use of antimicrobial agents; and
To develop the economic case for sustainable investment that takes account of the needs of all countries, and increase investment in new medicines, diagnostic tools, vaccines and other interventions.17
The plan recognized that the development of new antibiotics alone is not the answer.17 Whilst, as of December 2014, it was estimated that a total of 37 antibiotics were currently in development, experience suggests that the vast majority of these will never progress to licensing.18 Furthermore, even when a novel drug achieves market approval, it may not prove successful in clinical practice, since a significant number are withdrawn on efficacy grounds (Figure 1).19 Therefore, a key message of the WHO strategy is to preserve the effectiveness of existing antimicrobial medicines through conservation and stewardship programmes. Such stewardship seeks to engage with all sectors and disciplines, including health, agriculture, food security and economic development in a ‘one-health approach’.17
Antibiotic use in dentistry
In the UK, it is estimated that 80% of antibiotics are provided in primary care, and that approximately 9% of all primary care antibiotics are prescribed by general dental practitioners.20 In 2014, dentists in England prescribed 3.7 million antibacterials, at a cost of £6.4 million.20 However, since this figure does not include antibiotics provided to patients on a private basis, the true number of antibiotics prescribed by dentists is likely to be higher. The majority of the prescriptions made in dental primary care for an antibiotic involve members of the penicillin group, in particular amoxicillin.20 Other antibiotics frequently used, but to a lesser degree, are metronidazole, clindamycin and erythromycin.20 The selection of a particular antibiotic is made in general dental practice by necessity on an empirical basis due to logistical issues that effectively prevent the taking and sending of pus samples for analysis. As such, microbiological investigation of samples of pus is used extremely rarely.21 Despite increasing awareness about the potential contribution of dental prescribing to the emergence of antimicrobial resistance, the types and number of antibiotics prescribed by dentists has remained relatively constant over the last decade.20,22
The prescribing of any course of an antibiotic is associated with the potential for the emergence of resistant strains. Once a resistance is established, the loss of resistance genes within a bacterial population occurs slowly, even in the absence of the selecting antibiotic.23 Endodontic biofilms are thought to be particularly conducive for gene transfer, which may result in the spread of resistance genes between bacterial strains.24 Resistance has been increasingly encountered in acute dental infections over the last two decades,25,26 with the highest incidence of resistance detected in isolates of Prevotella species.27 The increased prevalence of resistant bacteria in dento-alveolar abscesses is highly likely to be due, in part, to the prescribing of β-lactam antibiotics, such as phenoxymethylpenicillin (penicillin V) and amoxicillin, by general dental practitioners, since this has been found to produce a 3-fold increase in the prevalence of β-lactamase, producing penicillin-resistant bacteria.28
In the UK, most antibiotics prescribed in general dental practice are associated with the management of acute infections, such as dento-alveolar (apical) abscesses or periodontal infection.29 Yet both these conditions should primarily be managed by local surgical measures; such as tooth extraction, drainage of a swelling or extirpation of the pulp. Evidence-based clinical guidelines, such as those published by the Scottish Dental Clinical Effectiveness Programme (SDCEP)30 and the Faculty of General Dental Practice (UK)31 strongly recommend that antibiotic therapy should only be prescribed when there is evidence of spreading infection, or in instances where surgical treatment has been unsuccessful. Since such unfavourable clinical features are only present in a minority of cases, it is obvious that most acute dental conditions can be successfully managed without the use of an antibiotic. However, evidence from UK general dental practice suggests that the use of antibiotics in the treatment of acute conditions is more widespread, with antibiotics being provided in situations where they are unlikely to be of clinical benefit, or prescribed without a surgical intervention to relieve or remove the source of infection. Not only does this unnecessarily expose patients to the adverse effects associated with an antibiotic, but also places them at a risk of developing antibiotic resistant colonies. Furthermore, providing an antibiotic without removing the source of infection may result in the patient suffering greater morbidity at a later date from untreated dental disease.32
Antimicrobial stewardship in general dental practice
Each and every dental practitioner has a professional responsibility to prescribe responsibly for his/her patients' best interests.33 Whilst most practitioners would recognize that acute conditions are best managed by surgical operative treatment, there are instances where the clinician may find the practicalities of this a challenge. Clinical time pressures, a patient's unwillingness to undergo operative treatment or requests for antibiotics are all known to influence dental prescribing practices.34 Indeed, current evidence suggests that between 71–81% of antibiotics prescribed in general dental practice do not adhere to published recommendations and guidance.35 Increased emphasis on teaching is therefore required to ensure that dental professionals are prescribing judiciously, performing operative treatment when it is indicated, and reinforcing to patients that it is both safe and appropriate to treat ‘toothache’ and dental pain operatively, without the need to use an antibiotic.
To minimize the potential contribution of dental prescribing to global antimicrobial resistance, the most important initial decision to be made by the dental surgeon is not which antibiotic to prescribe, but whether to prescribe an antibiotic at all.36 Current evidence suggests that antibiotic therapy is not required in the management of pulpitis, apical periodontitis, alveolar osteitis (dry socket), or pericoronitis in the absence of signs of spreading infection.31,37,38 All dentists are therefore encouraged to carry out an audit of their prescribing of antimicrobial agents to ensure that they are only providing antibiotics in situations where their use is clinically indicated. The use of clinical audit can significantly improve compliance with prescribing guidelines, especially when combined with collaborative discussion between practitioners.29,39 Therefore, dental practitioners are encouraged to carry out clinical audits of antimicrobial prescribing on a whole-practice basis, involving all members of the dental team.29,39 Postgraduate resources and funding are available in the UK to support the undertaking of such audits, and dentists are encouraged to contact their local Deanery to explore this. Clinical audit can also help practitioners identify factors in their practice that may act as barriers to optimal prescribing, such as clinical time pressures when treating emergency attendees,40 and take steps to address these, such as setting aside time to dedicated treatment sessions for emergency dental care.41
Clinical audit can also help ensure that, when an antibiotic is indicated, the correct drug is being prescribed. Amoxicillin and metronidazole are currently generally regarded as first-line agents for the treatment of odontogenic infections, whilst erythromycin is recommended for a patient who reports a hypersensitivity to penicillin and where metronidazole is contra-indicated.30 The prescription of co-amoxiclav, clindamycin, clarithromycin and azithromycin is not routinely recommended unless advised by a specialist, as they offer no advantage over first-line agents for most dental patients, but could contribute to the development of resistance and antibiotic-associated colitis.30 Similarly, prescription of cephalosporins, such as cephalexin, for dental infections is actively discouraged as they are implicated in the development of pseudomembranous colitis and Clostridium difficile infections.
Finally, audit can help practitioners ensure that, when prescribing, they are using the correct dose, frequency and duration necessary to eliminate the causative bacterial pathogen(s), whilst minimizing the selection of resistant bacterial strains. Evidence suggests that the longer antibiotics are taken, the greater the likelihood of resistance developing.28 Therefore, the historically taught concept of a complete course of antibiotic therapy is now regarded as obsolete. As such, there is a move towards shorter courses of treatment. Current guidelines recommending that, when provided in conjunction with an operative intervention, antibiotics should be prescribed for a maximum of five days and that, in many instances, it may be possible for the patient to discontinue therapy after two or three, subject to clinical review.31,42 It is therefore no longer necessary to tell patients ‘to complete’ their course of antibiotic therapy. If there is sufficient clinical evidence that the patient's host defences have regained control of the infection and that source of infection has been removed, the antibiotic therapy should be terminated.36
In addition to auditing their current practice, all dental practitioners should consider registering to become an ‘Antibiotic Guardian’ if they have not already done so.43 This scheme, which was developed by Public Health England in collaboration with government departments and professional bodies, calls on healthcare professionals and members of the public to make a ‘pledge’ about how they will conserve the effectiveness of existing antibiotic therapies. One of the pledges for dentists specifically encourages practitioners to discuss with patients alternative ways of managing toothache other than antibiotics (Figure 5). This may be particularly important since a patient's expectation or request for antibiotics is thought to increase the likelihood of an antibiotic being prescribed when one is not indicated.33 Educating patients that local measures are likely to result in more rapid resolution of the symptoms of acute dental conditions than antibiotics alone may reduce the number of patients who decline surgical treatment, thereby minimizing the number of unnecessary prescriptions.
Managing increasingly limited resources is one of the principal challenges of 21st Century healthcare. It is the duty of all clinicians who hold the responsibility of being a prescriber to make evidence-based decisions about their use of antibiotics, and to educate their patients about the reasons for doing so. Prudent prescribing by all dental practitioners is necessary to minimize the potential contribution that the dental profession makes to the emergence of antimicrobial resistance. Given the consequences of increasing levels of resistance, it is important that the dental profession makes a serious commitment to ensuring the accountability of his/her antibiotic prescribing decisions to preserve these invaluable agents for generations to come.