The immune system: basis of so much health and disease: 2. innate immunity Crispian Scully Eleni A Georgakopoulou Yazan Hassona Dental Update 2024 44:3, 707-709.
The immune system is the body's primary defence mechanism against infections, and disturbances in the system can cause disease if the system fails in defence functions (in immunocompromised people), or if the activity is detrimental to the host (as in auto-immune and auto-inflammatory states). A healthy immune system is also essential to normal health of dental and oral tissues. This series presents the basics for the understanding of the immune system, this article covering innate immunity.
Clinical Relevance: Modern dental clinicians need a basic understanding of the immune system as it underlies health and disease.
Article
Crispian Scully Eleni A Georgakopoulou Yazan Hassona
Innate immunity is:
The main line of defence;
Active at, and from, the time of infection.
The characteristics of innate immunity are that the response:
Occurs either immediately or very rapidly after infection;
Does not react against the body's own antigens (no auto-immunity);
Has a limited ability to discriminate (ie it shows no specificity);
Has a limited recognition repertoire (recognizes molecular patterns common to groups of microbes);
Responds to a second exposure to the same agent in the same way as it does to the first exposure;
Involves myeloid cells such as phagocytes, as well as mediators and receptors;
Cells and proteins may be found ‘in site’ present throughout the body, constantly on guard for ‘foreign invaders’.
Innate immunity includes the fundamental mechanisms that facilitate resistance to infection, which include:
The epithelial anatomical barriers of the skin and mucous membranes;
Secretions such as saliva and tears; and
The inflammatory response – characterized by increased localized blood flow and capillary permeability releasing soluble factors from the bloodstream and an influx of phagocytes such as neutrophils and macrophages.
Innate immunity can be divided into:
First line – non-inflammatory reaction (innate defences) and
Second line – local inflammation.
Innate defences
Innate defences include basic mechanisms resisting infections; predominantly including:
Anatomical barriers;
Physiological barriers;
Protective reflexes;
Cells;
Protective chemical mediators;
Inflammasomes.
Anatomical barriers
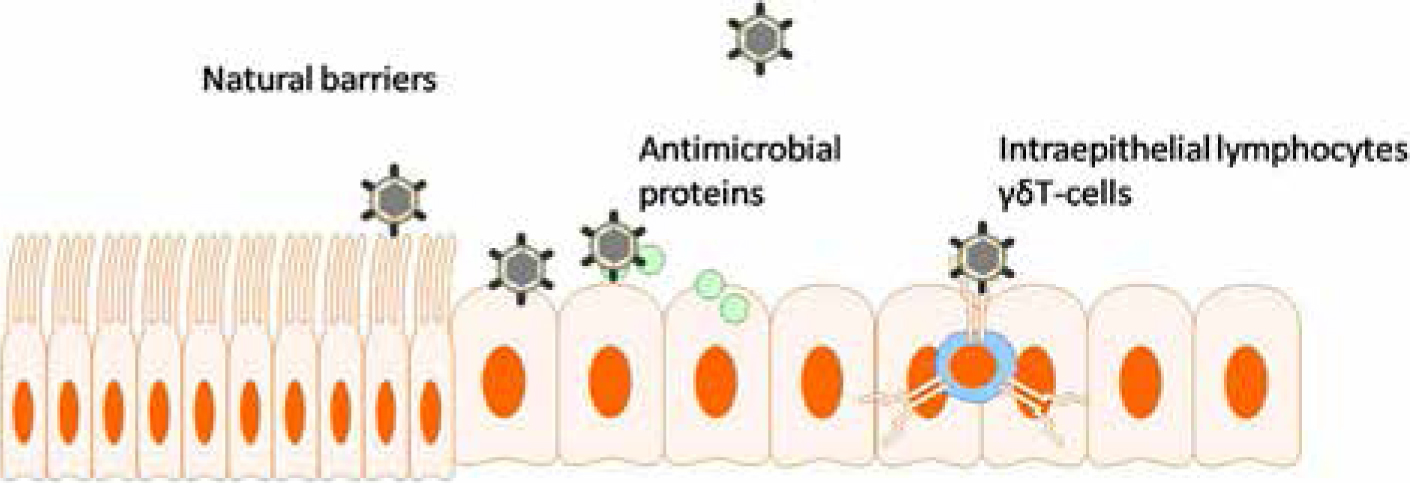
Anatomical barriers include the epithelia of skin and mucous membranes, and also in the respiratory tract, cilia (Figure 1).
Figure 1. The epithelia as a defence to microbes.
Skin
Skin has the following properties:
Consists of sheets of protective, dry, cornified epithelial cells;
Secretes antibacterial substances (fatty acids and enzymes) from sebaceous glands;
Normal microbial flora competes with potential pathogens by competing for essential nutrients, and producing inhibitory substances.
Mucosae
Mucoase have the following properties:
Fluids and mucus mechanically clean surfaces of mucosae of oral cavity, gastro-intestinal tract, genito-urinary tract and respiratory tract;
Normal microbial flora competes with potential pathogens.
Physiological barriers
Physiological barriers include pH (eg stomach acidity), oxygen tension, temperature and various soluble factors.
Protective reflexes
Protective reflexes include:
Blink reflex;
Coughing;
Sneezing;
Swallowing.
Hence, anatomical and physiological barriers together with the protective reflexes try to block all the entrance gates for microbes: such as ingestion, inhalation, skin contact, sexual contact and exchange of body fluids.
Cells
Cells of the innate immune system are either present in the connective tissue of epithelia, for example tissue macrophages which are also known as histiocytes (histo=ιστός=tissue in Greek), including hepatic Kupffer cells, alveolar macrophages, giant cells of granulomas, osteoclasts and dermal Langerhans cells) or migrate to the epithelia to fight invaders (eg polymorphonuclear neutrophils (PMNs).
Cells of the innate immune system may be divided according to their properties into phagocytes and non-phagocytes, and granulocytes and non-granulocytes (Table 1). Cells of the immune system are discussed in article 4.
Cells
Phagocytes
Non-phagocytes
Granulocytes
Eosinophils
NK-cells
Neutrophils
Basophils
Mast cells
Non-granulocytes
Fixed macrophages
Dendritic cells
Wandering macrophages
Γδ–T-cells
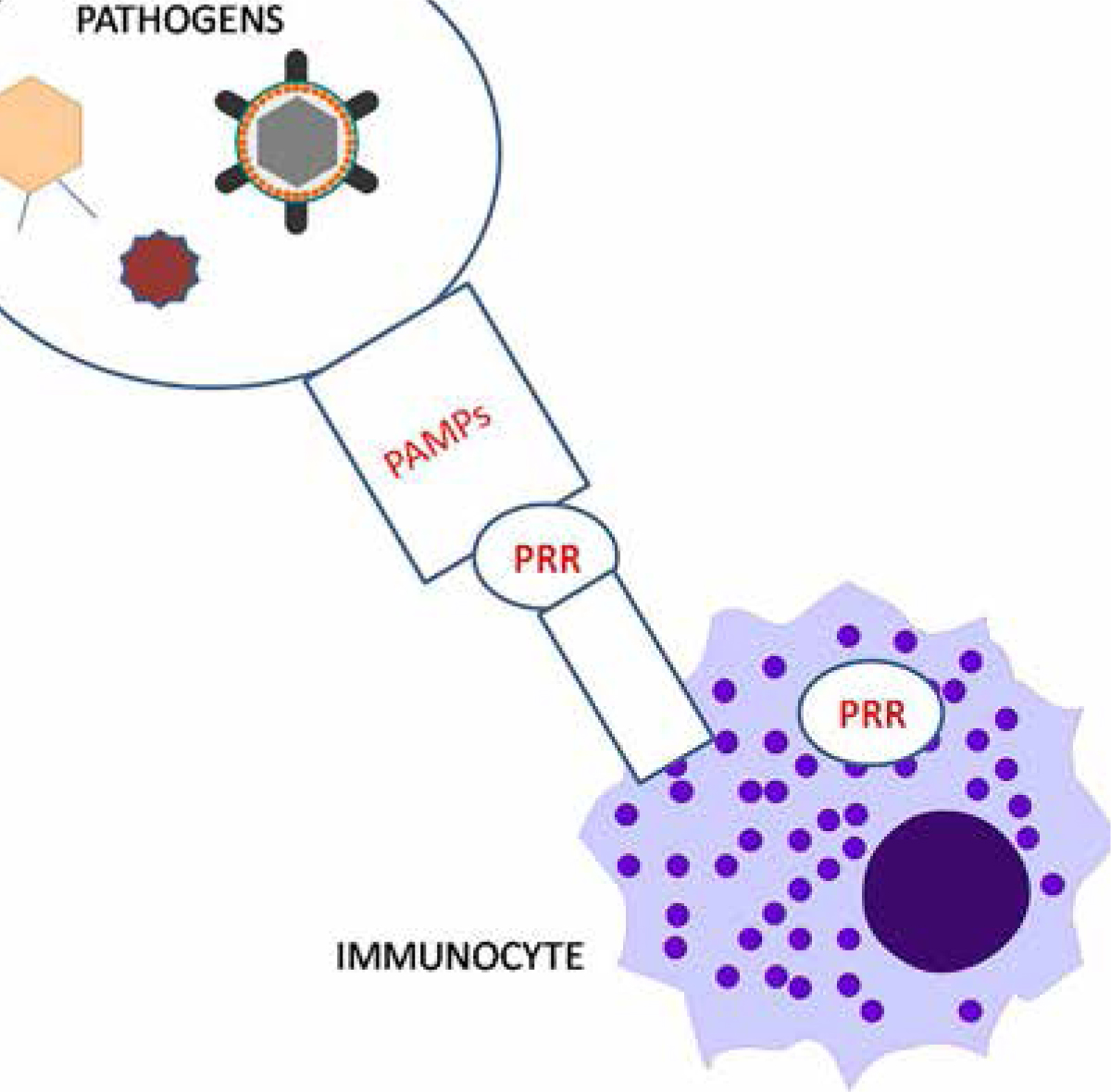
Cells involved in innate immune responses recognize pathogens through pattern recognition receptors (PRRs) which identify molecules on the surface of pathogens called microbe-associated molecular patterns (MAMPs) or pathogen-associated molecular patterns (PAMPs) (Figure 2).
Figure 2. Pathogens carry molecules (pathogen-associated molecular patterns [PAMPs]), which are recognized by the pattern recognition receptors (PRRs) of the cells of the innate immune system.
PAMPs can trigger their recognition when they bind to pattern recognition receptors (PRRs) on leukocytes. PAMPs include:
Lipopolysaccharide (LPS or ‘endotoxin’, mainly found on Gram-negative bacteria);
Peptidoglycans (mainly on Gram-positive bacteria);
Lipoproteins;
Flagellin;
Ds-RNA (double-stranded ribonucleic acid);
DNA (deoxyribonucleic acid).
Pattern recognition receptors (PRRs) recognize all types of pathogens, forming inflammasomes which, once activated, modulate the release of inflammatory cytokines and reactive oxygen species, and enhance phagocytosis, and dendritic cell maturation.
PRRs are found on a range of cells including:
Natural killer (NK) cells;
Macrophages;
Neutrophils and other granulocytes;
Dendritic cells;
Fibroblasts;
Platelets.
There are different types of PRRs, including those shown in Table 2 and Figures 3, 4 and 5.
PRR
Terminology
Activities
Toll-like receptors
TLRs (cell surface receptors)
12 TLRs identified. When activated, cause phosphorylation of IL-1 receptor protein kinases, which activate the tumour necrosis factor (TNF) receptor, and thus the NF-κB, and MAPK (mitogen-activated protein kinases) pathways, releasing pro-inflammatory cytokines.
Nucleotide oligomerization domain (NOD or CARD 15)-like receptors
NLRs (cytosolic receptors)
Recognize NOD proteins, leading to activation of both NF-κB and JNK (C-Jun N terminal kinase) inflammatory pathways.
C-lectin receptors
CLR
Recognize C-type lectins, and function as receptors for cell-cell adhesion, and for antigen uptake, recognizing glycans (eg mannose) and internalizing antigens for presentation to lymphocytes.CLRs are divided into 2 clusters: group I CLRs: the mannose receptor family and cluster II CLRs: the sialoglycoprotein receptor family.
Others
CD14, a phagocyte-expressed PRR that functionally interacts with TLR; peptidoglycan recognition proteins.Vitamin D receptor (VDR).Retinoic acid inducible gene receptors (RLRs).DNA-sensing inflammasome, which probably plays a role against DNA viruses, intracellular bacteria and in recognizing DNA immune complexes (eg in lupus erythematosus).
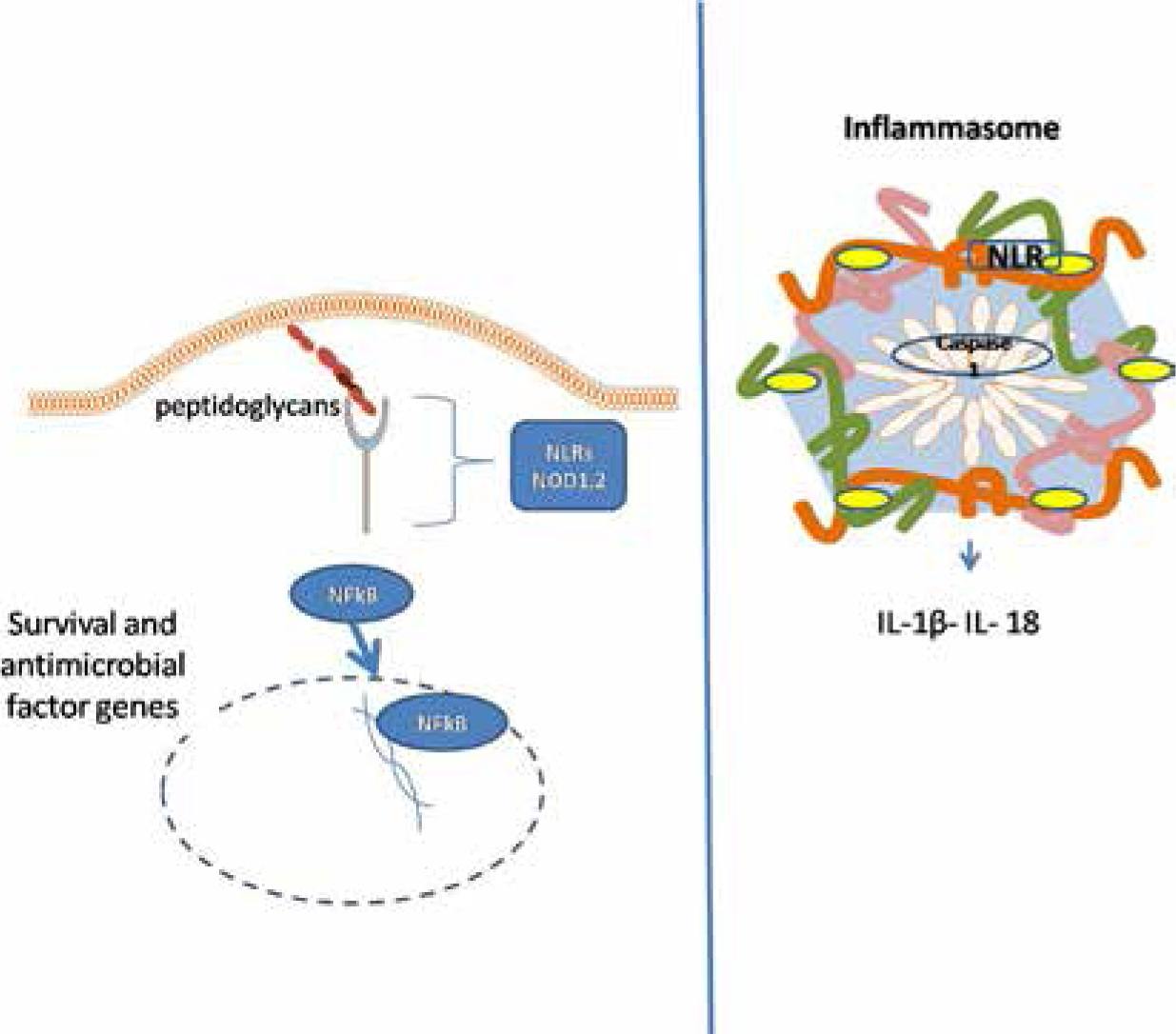
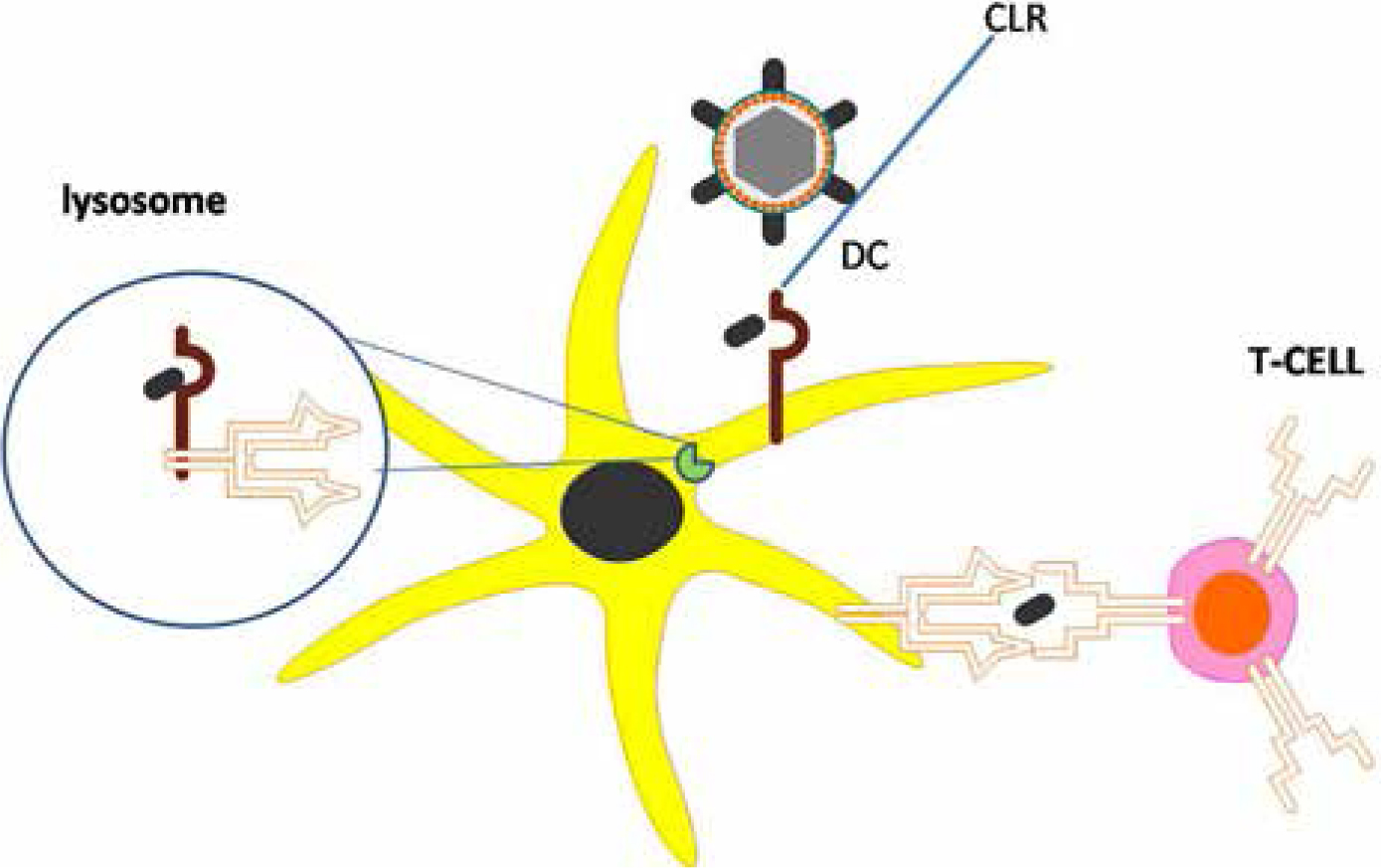
Figure 3. Toll like receptors (TLRs) located on the surface of immunocytes recognize antigens common to groups of pathogens. TLRs found on endosome which contain pathogens are designed to distinguish between foreign and cellular nucleic acids. For example, mycobacterial antigens via surface TLR2 activate dendritic cells and subsequently stimulate CD4–T-cells. Similarly, endosomal TLR7 identifies single-stranded RNA in endosomes, which contain viral genomes internalized by macrophages and is also involved in the pathogenesis of systemic lupus erythematosus.Figure 4. NOD like receptors (NLRs) are intracellular PRRs which recognize foreign antigens. NOD 1,2 NLRs recognize peptidoglycans and mediate the activation of NFkB which subsequently induces the expression of pro-inflammatory cytokines. Other NLRs (Ipaf, Nalp1, cryopyrin) assemble with caspase 1 to form the structure of the inflammasome and mediate the activation of the auto-inflammatory cytokines IL-1β and IL-18. These cytokines play an important role in the periodic fever syndromes.Figure 5. C-type lectin receptors (CLRs) on the surface of dendritic cells (DCs) recognize carbohydrate parts of microbes and internalize them, these molecules are then be processed by DCs and presented to T-cells by MCH Class I and II (CD8 and CD4 cells, respectively).
Protective chemical mediators
Protective chemical mediators include:
The complement system, which helps or ‘complements’, the ability of antibodies and phagocytes to clear pathogens from an organism, and is an important mediator of acute inflammation (the complement system is described in detail in Article 5);
The coagulation system activated platelets, for example, release betalysins which can lyse Gram-negative bacteria.
Other factors include:
Pattern recognition receptors (PRRs);
Lactoferrin, transferrin (iron-binding proteins);
Lactoperoxidase (saliva and milk);
Lysozyme (saliva and tears; hydrolyzes bacterial cell walls);
Cytokines such as interleukin-1 and interferons;
Fibronectin;
Host defence peptides (HDPs) produced by PMNLs and epithelial cells and found in secretions, such as saliva. The main HDPs are shown in Table 3. They function by virtue of:
Antimicrobial activity;
Regulation of innate and acquired immune responses;
Suppression of host responses to inflammatory products such as lipopolysaccharide (LPS).
Inflammasomes are proteins which, once activated, trigger an inflammatory cascade. Innate immunity is also dependent upon inflammasomes and inflammation. Inflammasomes are triggered by the recognition of pathogens by leukocytes (Figure 4) and, once activated, result in the production of many pro-inflammatory mediators. The exact composition of an inflammasome depends on the activator which initiates the inflammasome assembly, but all inflammasomes inevitably activate the inflammatory cytokines: interleukin-1β (IL-β) and IL-18.
Central to many of the subsequent reactions is NF-κB (nuclear factor kappa-light-chain-enhancer of activated B-cells) – a protein complex involved in cellular responses to stimuli such as stress, free radicals, cytokines and viral or bacterial antigens.
When the PRRs and inflammasomes of leukocytes are activated, their granules are exocytosed and inflammatory mediators released. For example, large amounts of TNF-α and histamine are released by stimulated mast cells and other cells involved in inflammation. Inflammasomes also contain pro-caspase 1 (IL-1β converting enzyme [ICE]) which, when activated, consequently produces the inflammatory cytokines IL-1β and IL-18.
IL-1β is a potent pyrogen (fever producer) which activates lymphocytes, NK cells and endothelial cell secretion of interferon gamma (IFN-γ) and initiates the acute phase response.
Conclusion
Innate immunity is the first line of defence against pathogens.
It is characterized by the speed of onset, and the lack of memory and discrimination (specificity).
In addition to the protective effects of anatomical and physiological barriers, innate immunity involves protective reflexes, immune cells, and inflammatory products.
Cells involved in innate immunity recognize pathogens through various receptors known collectively as pattern recognition receptors (PRR).
IL-1β, IL-18, and NF-kB are particularly important in mediating inflammation and innate immune responses.