London: Royal College of Surgeons of England Faculty of Dental Surgery; 2000
Ashley MP, Pemberton MN, Saksena A, Shaw A, Dicksonas S Improving patient safety in a UK dental hospital: long-term use of clinical audit. Br Dent J. 2014; 217:369-373
Ramoni RB, Walji MF, White J From good to better: toward a patient safety initiative in dentistry. J Am Dent Assoc. 2012; 143:956-960
Bailey E, Tickle M, Campbell S Patient safety in primary care dentistry: where are we now?. Br Dent J. 2014; 217:339-344
Pemberton MN, Ashley MP, Shaw A, Dickson S, Saksena A Measuring patient safety in a UK dental hospital: development of a dental clinical effectiveness dashboard. Br Dent J. 2014; 217:375-378
International Ergonomics Association.
The Robert Francis Report. Nurs Educ Today. 2013; 33:181-182
NHS England.
: Healthcare Improvement Scotland and NHS Education Scotland; 2011
London: NQB; 2014
Carayon P Human factors in patient safety as an innovation. Appl Ergon. 2010; 41:657-665
London: DoH; 2012
Sevdalis NLondon: The Health Foundation; 2013
McCulloch P, Mishra A, Handa A, Dale T, Hirst G, Catchpole K The effects of aviation-style non-technical skills training on technical performance and outcome in the operating theatre. Qual Saf Health Care. 2009; 18:109-115
Kodate NRA, Anderson JE, Flin R Non-Technical Skills (NTS) for enhancing patient safety: achievements and future directions. Jap Soc Qual Saf Healthcare (JSQSH). 2012; 7:366-370
Boet S, Bould MD, Fung LL, Qosa H, Perrier L, Tavares W Transfer of learning and patient outcome in simulated crisis resource management: a systematic review. Can J Anesth. 2014; 61:571-582
Schmutz J, Manser T Do team processes really have an effect on clinical performance? A systematic literature review. Br J Anaesth. 2013; 110:529-544
Catchpole K, Mishra A, Handa A, McCulloch P Teamwork and error in the operating room – analysis of skills and roles. Ann Surg. 2008; 247:699-706
Mishra A, Catchpole K, Dale T, McCulloch P The influence of non-technical performance on technical outcome in laparoscopic cholecystectomy. Surg Endosc. 2008; 22:(1)68-73
Mazzocco K, Petitti DB, Fong KT, Bonacum D, Brookey J, Graham S Surgical team behaviors and patient outcomes. Am J Surg. 2009; 197:678-685
General Dental Council. 2013.
WHO Patient Safety Curriculum Guide. 2011.
Yule S, Paterson-Brown S Surgeons' non-technical skills. Surg Clin N Am. 2012; 92
Yule S, Flin R, Paterson-Brown S, Maran N Non-technical skills for surgeons in the operating room: a review of the literature. Surgery. 2006; 139:140-149
Fletcher G, Flin R, McGeorge P, Glavin R, Maran N, Patey R Anaesthetists' non-technical skills (ANTS): evaluation of a behavioural marker system. Br J Anaesth. 2003; 90:580-588
Yule S, Flin R, Paterson-Brown S, Maran N NOTSS: a non-technical skills taxonomy for surgeons. Br J Surg. 2005; 92
Christman A, Schrader S, John V, Zunt S, Maupome G, Prakasam S Designing a safety checklist for dental implant placement: a Delphi study. J Am Dent Assoc. 2014; 145:131-140
Pinsky HM, Taichman RS, Sarment DP Adaptation of airline crew resource management principles to dentistry. J Am Dent Assoc. 2010; 141:1010-1018
Gupta A, Ankola AV, Hebbal M Optimizing human factors in dentistry. Dent Res J. 2013; 10:254-259
Thornton LJ, Stuart-Buttle C, Wyszynski TC, Wilson ER Physical and psychosocial stress exposures in US dental schools: the need for expanded ergonomics training. Appl Ergon. 2004; 35:153-157
Hayes M, Cockrell D, Smith DR A systematic review of musculoskeletal disorders among dental professionals. Int J Dent Hyg. 2009; 7:159-165
Thornton LJ, Barr AE, Stuart-Buttle C, Gaughan JP, Wilson ER, Jackson AD Perceived musculoskeletal symptoms among dental students in the clinic work environment. Ergonomics. 2008; 51:573-586
Finsen L, Christensen H, Bakke M Musculoskeletal disorders among dentists and variation in dental work. Appl Ergon. 1998; 29:119-125
Akesson I, Balogh I, Hansson GA Physical workload in neck, shoulders and wrists/hands in dental hygienists during a work-day. Appl Ergon. 2012; 43:803-811
Haddad O, Sanjari MA, Amirfazli A, Narimani R, Parnianpour M Trapezius muscle activity in using ordinary and ergonomically designed dentistry chairs. Int J Occup Environ Med. 2012; 3:76-83
Robson R ECW in Complex Adaptive Systems. In: Wears R, Hollnagel E, Braithwaite J Kent: Ashgate; 2015
Hollnagel EToronto: Sustainable Transformation: Building a Resilient Organization; 2010
Hoffman RR, Crandall B, Shadbolt N Use of the critical decision method to elicit expert knowledge: a case study in the methodology of cognitive task analysis. Hum Factors. 1998; 40:254-276
Holden RJ, Carayon P, Gurses AP SEIPS 2.0: A human factors framework for studying and improving the work of healthcare professionals and patients. Ergonomics. 2013; 56:(11)1669-1686
Sujan MP, Spurgeon P, Cooke M Translating tensions into safe practices through dynamic trade-offs: the secret second handover. In: Wears RL, Hollnagel E, Braithwaite J Kent: Ashgate; 2014
Ross AJ, Anderson JE, Kodate N, Thompson K, Cox A, Malik R Inpatient diabetes care: complexity, resilience and quality of care. Cogn Technol Work. 2014; 16:91-102
Klein GNew York: Doubleday; 2003
Nemeth CWR, Woods D, Hollnagel E, Cook R Minding the gaps: creating resilience in health care. In: Henriksen KBJ, Keyes MA, Grady ML Rockville MD: AHRQ; 2008
Catchpole K Spreading human factors expertise in healthcare: untangling the knots in people and systems. BMJ Qual Saf. 2013; 22:793-797
This paper proposes that the science of Human Factors and Ergonomics (HFE) is suitable for wide application in dental education, training and practice to improve safety, quality and efficiency. Three areas of interest are highlighted. First it is proposed that individual and team Non-Technical Skills (NTS), such as communication, leadership and stress management can improve error rates and efficiency of procedures. Secondly, in a physically and technically challenging environment, staff can benefit from ergonomic principles which examine design in supporting safe work. Finally, examination of organizational human factors can help anticipate stressors and plan for flexible responses to multiple, variable demands, and fluctuating resources.
CPD/Clinical Relevance: HFE is an evidence-based approach to reducing error rates and procedural complications, and avoiding problems associated with stress and fatigue. Improved teamwork and organizational planning and efficiency can impact directly on patient outcomes.
Article
Quality and safety in dentistry
Dental practitioners are required to have in place effective ways of ensuring safety and quality, encompassing a whole range of issues including staffing, procurement, infection control, and complaint handling. The Care Quality Commission (CQC) aims to ensure that dental professionals provide ‘safe, effective, compassionate, high-quality care [and] meet fundamental standards of quality and safety',1 and there are similar standards for quality, efficiency and safety in Scotland and Northern Ireland.2,3
Clinical audit in particular has been applied with some success.4,5 However, it has been noted that systematic safety programmes are still lacking6 and there have been recent calls to apply ideas and initiatives in patient safety further, whether in primary care dentistry,7 or in dental hospitals and oral/maxillofacial surgery departments.8
The purpose of this paper is to suggest that the established science of Human Factors and Ergonomics provides an integrated approach for practitioners seeking to improve safety, quality and efficiency.
Human Factors and Ergonomics
The International Ergonomics Association defines Human Factors and Ergonomics (HFE) as:
‘the scientific discipline concerned with the understanding of interactions among humans and other elements of a system, and the profession that applies theory, principles, data and methods to design in order to optimize human well-being and overall system performance.'9 (Figure 1)
Figure 1. Human Factors and Ergonomics is the science which studies interactions between people, tasks and other elements of work systems (With permission of the Chartered Institute of Ergonomics and Human Factors – www.ergonomics.org.uk).
NHS England's National Quality Board, in response to the Mid Staffordshire NHS Foundation Trust Public Inquiry,10 is committed to embedding HFE (in national organizations, provider, and commissioning organizations) to improve quality and productivity.11
There have been similar calls for applying HFE principles through NHS Scotland.12
Importantly, the CQC (along with The National Institute for Health and Care Excellence, the General Medical Council, the Nursing and Midwifery Council and many others) recently signed a joint undertaking to build a ‘high performing, resilient and efficient healthcare system' through HFE principles which can ‘contribute significantly to improving the quality (effectiveness, experience and safety) of care for patients' by providing ‘an integrated, evidenced and coherent approach to patient safety, quality improvement and clinical excellence.'13
‘Not an optional extra’
This coherence in part derives from the applicability of HFE at all levels of safety and quality.14 There are benefits at:
The individual/cognitive level (eg ways of coping with fatigue and avoiding human error);
Team level (eg improved communication and co-ordination);
Environmental level (eg better design of physical resources and use of technology); and
The system level (through understanding of organizational processes).
HFE in healthcare aims both to minimize error and improve quality by optimizing behaviours and processes, and addressing issues in design. It also provides a sound theoretical basis for non-clinical education and training. Sir Stephen Moss, Chair of the Department of Health Human Factors Reference Group, thus argues that:
‘embedding this knowledge and understanding is not an optional extra. […] The time feels right to re-energise the focus on our approach to embed human factors knowledge into practice, education and regulation […].15
Human factors and ergonomics for dental teams
The scope for engaging with the applied science of HFE and harnessing potential benefits for dentistry and its associated professions is broad. However, a few suggestions are put forward here.
Application 1: Non-technical skills for the dental team
Many patient safety tools, such as pre-surgical checklists, have their roots in Crew Resource Management (CRM) techniques developed in aviation to improve cockpit performance.16 There is evidence that error and harm can be prevented17 through paying close attention to a set of interrelated cognitive and social abilities now widely referred to as Non-Technical Skills (NTS) which are:
‘general cognitive and social skills that allow [healthcare professionals] to […] monitor the situation, make decisions, take a leadership role, [and] communicate and co-ordinate their actions within a team, in order to achieve high levels of safety and efficiency.'18
Table 1 shows elements within the main NTS categories.19
Core Non-Technical Skills Categories
Elements
Situation awareness
Gathering information
Interpreting information
Anticipating future states
Decision-making
Defining the problem
Considering options
Selecting and implementing option
Outcome review
Communication
Sending information clearly and concisely
Including context and intent during information exchange
Receiving information, especially by listening
Identifying and addressing barriers to communication
Team-working
Supporting others
Solving conflicts
Exchanging information
Co-ordinating activities
Leadership
Using authority
Maintaining standards
Planning and prioritizing
Managing workload and resources
Stress management
Identifying symptoms of stress
Recognizing effects of stress
Implementing coping strategies
Fatigue management
Identifying symptoms of fatigue
Recognizing effects of fatigue
Implementing coping strategies
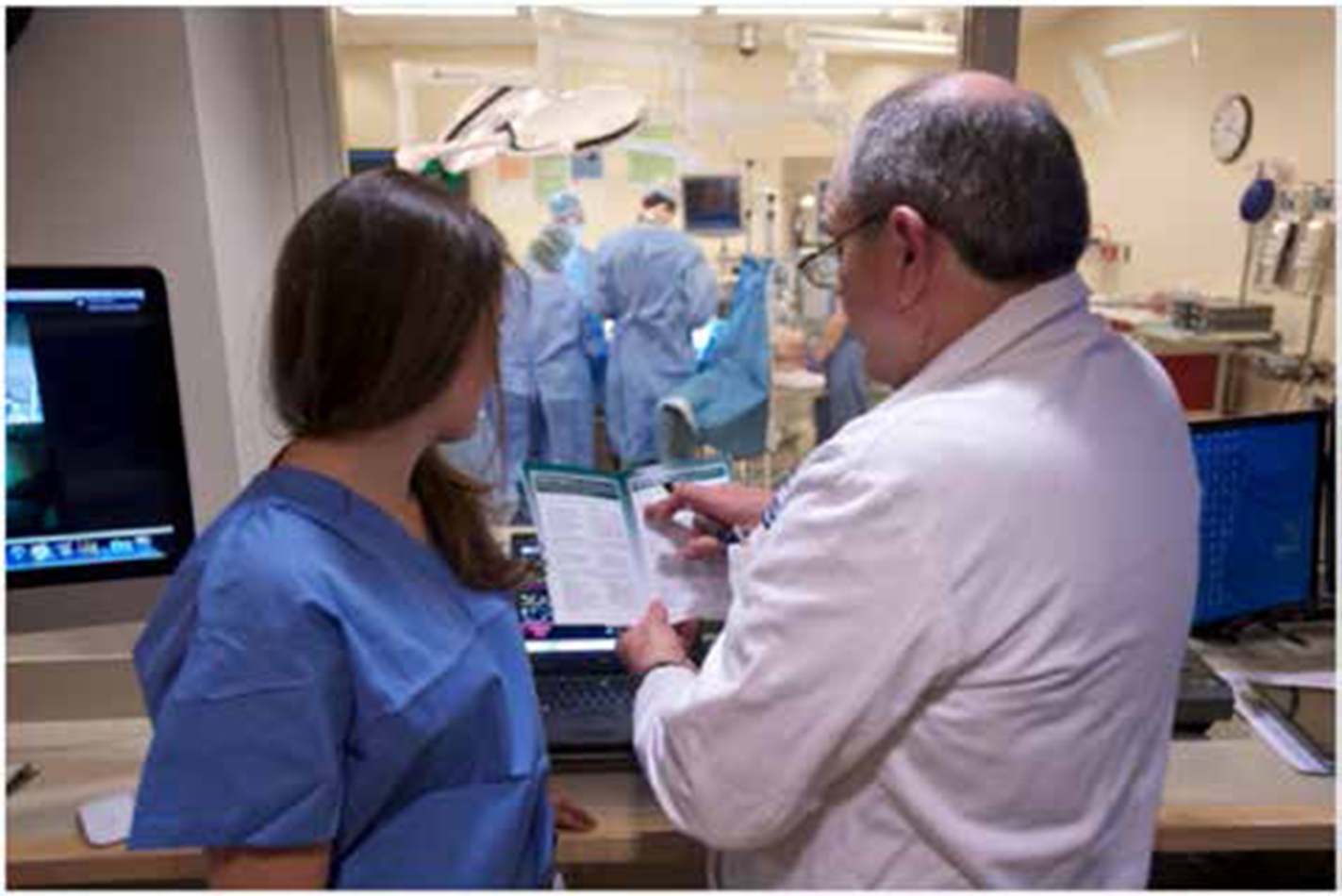
There is now a wide range of activity in healthcare around training and assessing these NTS, measuring associations with clinical outcomes (Figure 2).20,21 For example, procedural problems and increased operative times have both been related to poor leadership and management skills,22 and the ability to make predictive judgements from observation is inversely related to error rates.23
Figure 2. Many surgical specialties now train and assess teams in ‘Non-Technical Skills’ such as communication, leadership and management of stress and fatigue. (With permission from Neil and Elise Wallace STRATUS Center for Simulation, Brigham and Women's Hospital, Boston, MA – www.notss.org
A report in the American Journal of Surgery showed that teams displaying NTS markers such as pre-briefing, mutual respect, asking for input, and ongoing reflection to avoid ‘tunnel vision’, had a lowered risk of surgical deaths and complications.24 It would be interesting to study whether any of these or similar markers could be reliably observed in dental teams, and what the associated outcomes might be.
The General Dental Council is clear that dental education aims to produce rounded individuals with a range of professional and team-working skills, recognizing that a good team will have:
Good leadership;
Different roles and responsibilities;
An understanding of those roles and responsibilities;
Clear, shared aims; and
An ability to work together to achieve these aims.25
It is apparent that there is clear alignment between the aims of the GDC and the body of evidence for promoting key NTS and associated behavioural markers (see also the World Health Organization curriculum with respect to effective teams).26
Bringing these non-clinical aspects in dental education and practice into alignment with the strategically-supported NTS frameworks, particularly relating to surgical procedures,27,28 offers a chance to:
Learn from good practice across other areas of primary and secondary care;
Observe, assess and improve key NTS in the dental context;
Design improvement interventions that are built on work already done in NTS across healthcare;
Embed NTS principles and understanding into undergraduate education and postgraduate training/Continuing Professional Development.
There are specialty-specific NTS taxonomies, including for Anaesthetists' Non-Technical Skills (ANTS29) and Non-Technical Skills for Surgeons (NOTSS30). Our own work to identify, develop and test educational tools for Dental Non-Technical Skills (the ‘DENTS’ project) is underway.
Further initiatives include a preliminary standardized safety checklist for dental implant surgeries31 and an outpatient checklist directly derived from CRM/aviation safety principles.32 The aim of both is to reduce error through maintaining situational awareness. The latter has five stages: ‘appointment review’ ‘before procedure’, ‘procedure’, ‘before dismissal’ and ‘after dismissal’. Checklist items include but are not limited to: verbalize medical history; review medications; review notes from other health care providers, including specialists; review postoperative instructions and care with patient; inform team members of necessary follow-up items, etc. Feasibility and effectiveness trials of these or similar tools would seem worthy of further investigation.
Application 2: Dental ergonomics
It is also a strength of HFE approaches to healthcare that the safety and wellbeing of the practitioner, as well as the patient, is prioritized; in fact the one area within HFE that is relatively well established in dentistry centres on ergonomic issues affecting the profession.33
Lack of attention to the physical workspace (seating, instruments, lighting, etc) increases stress and fatigue and is associated with a range of unwanted outcomes for patients and clinicians alike.34 Musculoskeletal disorders are a significant issue for professionals in dentistry and dental hygiene35 and problems are known to develop as early as the undergraduate stage.36 Studies have identified specific biomechanical issues such as prolonged cervical flexion and upper arm abduction which arise from non-neutral or ‘deviated’ postures.37 Various painful and debilitating inflammations can also arise from repetitive tasks and static force problems, eg in pinch gripping.38
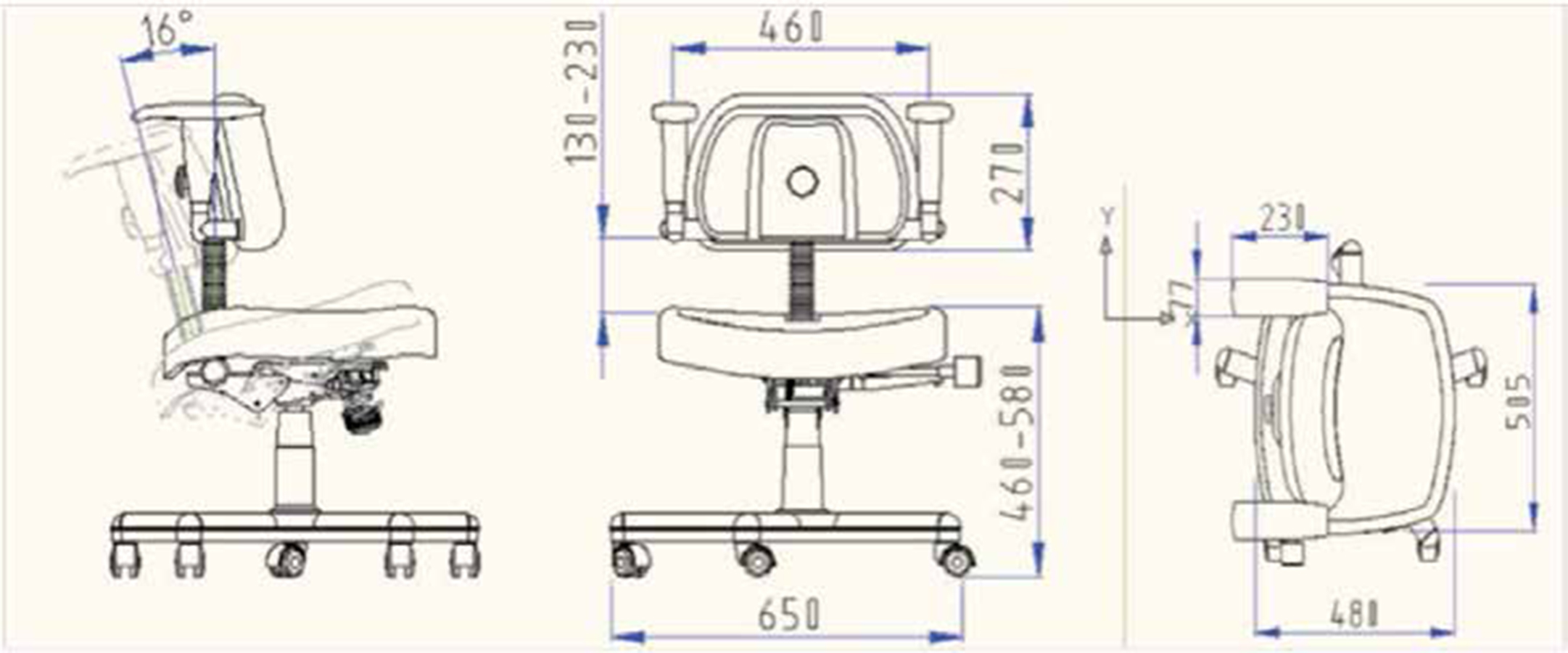
With the recent bestowing of the Royal Charter on the Institute of Ergonomics and Human Factors (CIEHF), there are renewed opportunities to link more closely with recognized professionals in HFE practice, and to embed evidence-based HFE principles into all aspects of the physical and technical dental workspace, including health technology design, human-device interactions, etc. Gupta et al33 outline a range of practical recommendations including training in dental schools to promote ‘ergonomic culture’. They also recommend the integration of design interventions (eg in chair technology (Figure 3), magnification, lighting, ergonomic instruments), with behavioural interventions targeting postural and other fatigue-related problems (exercises, resting periods, procedural list rotation, etc). Good quality research is vital in this area, and any interventions need to be interdisciplinary, but lead by the profession. A systematic programme of work can be useful in:
Providing information on risks and preventive interventions;
Understanding the impact of new technology and procedures; and
Ensuring regulations and standards are informed by sufficient understanding of ergonomic considerations.
Figure 3. Sketch of dentistry chair ergonomically designed for posture support. (Permission from IJOEM.)39
Application 3: Organizational human factors
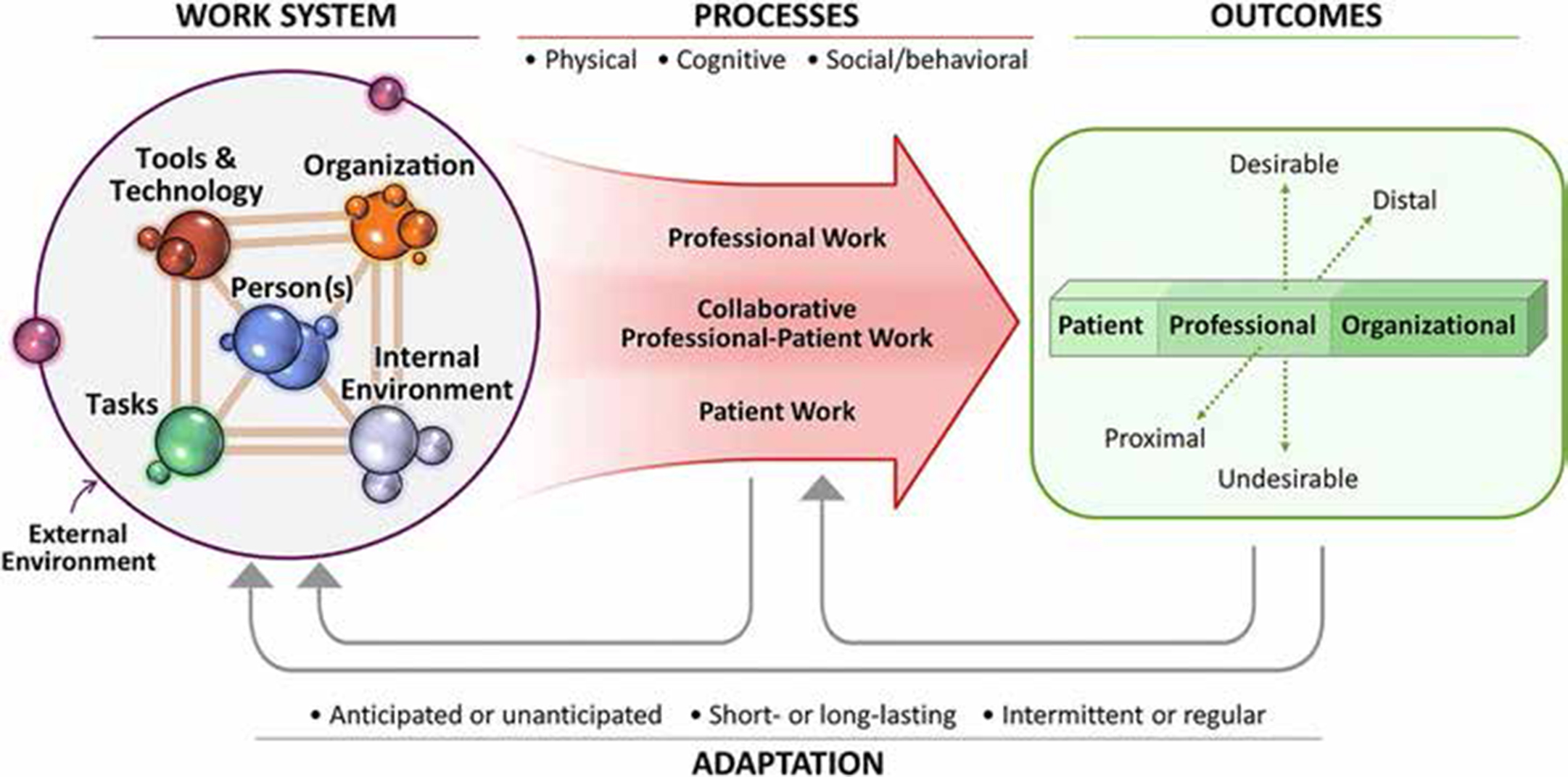
Finally, there is now widespread recognition that patient and organizational outcomes in healthcare emerge from a combination of multiple individual, team, technological and environmental factors and processes (Figure 4).
Figure 4. Model looking at safety from an organizational human factors perspective. (Permission from Taylor and Francis).43
This ‘systems thinking’ means that improvement attempts focused on single components or issues are often unsuccessful over the longer term.40 Faced with this need to deal with a complex set of circumstances, professionals in a range of disciplines across the NHS have begun to look to HFE for tools and techniques to help them explore, understand and evaluate work systems and processes more holistically.41,42
Dental care involves multiple interacting factors. People make decisions that are affected by:
Fluctuating demand;
Patient information, including how this is assessed and recorded;
Clinical aims;
Staffing issues;
Technical resource and equipment issues; and
Regulatory demands and requirements.
There are multiple members of the multidisciplinary team all balancing their own capacities against the demands placed upon them; and this all takes place in a physical environment that offers various environmental conditions within which fatigue and stress has to be managed.
Resilient healthcare
The systems-level discipline of Resilient Health Care (RHC)44 is concerned with the inherent difficulties in practice and the ways in which people and organizations overcome these. This involves paying close attention to work ‘as it is actually achieved' in the face of difficulty, rather than assuming that a set of ideal conditions can always be maintained. No matter that we may attempt to put protocols and guidelines in place, there will always be some need to adapt or adjust in response to fluctuating conditions; to paraphrase Einstein, ‘the difference between theory and practice is bigger in practice than in theory'! To put it another way, there is a tension between ‘work-as-imagined’ and ‘work-as-done’:
In work-as-imagined, it is assumed that we can align demand (eg patients, treatment plans, targets) with capacity to meet that demand (eg staffing, equipment, procedures);
In work-as-done, this alignment is never 100%, thus everyday clinical work is characterized by adaptations and adjustments that people constantly have to make to reconcile gaps between goals, procedures and resources.45
Success/failure is dependent upon the ability to make successful adjustments and adaptations to fluctuating demand and capacity, and then to learn from this and anticipate the next potential bottleneck or stressor. By focusing on these tensions in everyday practice46 and, in particular, on the ways in which organizations and individuals bridge these potential gaps in care,47 we can learn from work that is accomplished dynamically and successfully under variable conditions.
Resilient organizations have ways of finding ‘windows on the system’. One idea is to have ‘pre-mortems’ at team or department meetings, where imaginary (but possible) ‘patient safety incidents’ are described, then causes/reasons for the ‘failure’ are generated, and actions discussed.48 This embeds a collective mindfulness, and the actions generated are often better thought out than those ‘knee jerk’ responses to an actual event where harm has occurred and blame is assigned.
It is also desirable to assess resilience regularly, individually or in groups,41 through working through a set of questions designed to find the edge of the ‘safe operating envelope’ (ie when demand is outstripping capacity)48 and to adjust accordingly. The idea is that the system is able to ‘stretch’ before brittleness (inertia, inability to respond flexibly) sets in.49 Questions can include:
Do we know what to do if (x) problem arises; do we have the capacity; how did we decide on this response; are we training for such events; are there events we haven't imagined yet?
Are we measuring the right things; what about process as well as outcome indicators; what is the time lag between measurement and interpretation?
How do we achieve success; what do we learn from it; do we only act/redesign after failure?
Where is the edge of our safety envelope; are we close to the edge; how will we know?
Resilient Health Care is about the ways in which people and teams proactively create safety in their everyday work through processes like this, building in adaptive and reflexive capacities that equip them to respond better when circumstances change. Dental care seems a highly appropriate area for the application of these organizational models from HFE. Because the focus in not solely on avoiding harm, but on proactively maximizing success and opportunity as well, this can promote a positive culture, which empowers clinical staff to put safety, quality and efficiency at the forefront of patient-centred care.
Discussion
It has recently been claimed that ‘tremendous progress’ has been made in applying HFE to healthcare, thus moving ‘from a state in which clinicians had little exposure to HF work, and even fewer saw its value, to widespread acknowledgement of the value of human-centred systems thinking in healthcare’.50 Whilst this may be overstating the case somewhat, a number of strategic initiatives have recognized HFE as an evidence-based approach which can help in meeting the quality and safety goals of providers and regulators alike, and all dental professionals are encouraged to engage with the discipline.
Conclusion
Dentistry can benefit from applied HFE principles and approaches. HFE offers many advantages to dental professionals wanting to engage with an evidence-based approach to quality and safety.
Take away messages are:
Existing knowledge about how individuals and teams co-ordinate care can be adapted/applied to the dental setting. This understanding is vital in avoiding costly errors, promoting safe cultures of working, and learning from adverse events.
In a pressured physical workplace, with ongoing advances in dental technology, a good understanding of ergonomic principles can be fruitful for avoiding a range of work-related disorders which affect efficiency, productivity and safety.
It is important that those seeking to implement improvement initiatives understand the multiple demand/capacity issues facing practitioners and the important role of planning for flexible, adaptive responses in producing good care.
The challenge going forward will be to embed HFE in dental education and practice to support safe, efficient systems of care. Some in healthcare have misapprehended ‘human factors’ as simply a collection of things about humans. Dentistry has the opportunity to lead the way in realizing the full potential of HFE science. Dental professionals will be the key ingredient, as much of this potential relies on the ability and willingness of those at the sharp end to take this forward.