Stovner L, Hagen K, Jensen R The global burden of headache: a documentation of headache prevalence and disability worldwide. Cephalalgia. 2007; 27:(3)193-210
Stovner LJ, Andree C Impact of headache in Europe: a review for the Eurolight project. J Headache Pain. 2008; 9:(3)139-146
National Institute for Health and Care Excellence: technology appraisal guidelines, N. 2012.
British Association for The Study of Headache, B 2007.
The International Classification of Headache Disorders 3rd edition (beta version). Cephalalgia. 2013; 33:(9)629-8086
National Institute for Health and Care Excellence: technology appraisal guidelines, N. 2012.
Cohen AS, Matharu MS, Goadsby PJ Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) or cranial autonomic features (SUNA) – a prospective clinical study of SUNCT and SUNA. Brain. 2006; 129:(10)2746-2760
Abrams BM Medication overuse headaches. Med Clin North Am. 2013; 97:(2)337-352
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
This last in a series of 10 papers aims to provide the dental and medical teams with an update in headache conditions relevant to dentistry and medicine. Headache is the most common presenting symptom for patients presenting to A&E departments.
CPD/Clinical Relevance: Most of the dental team take for granted their knowledge and ability to manage acute dental pain. However, the education and preparation in managing patients with headache conditions remains poor. Dentists are in a privileged position to be able to advise their patients about common conditions including headaches.
Article
Headache is a common symptom with numerous aetiologies (Table 1). It is estimated that one in every five consultations with a neurologist is because of headache. Globally, it is estimated that 46% of the worldwide population have an active headache disorder. The World Health Organization has ranked headache as one of the top 10 most disabling disorders for both genders.1
Acute/sudden onset
‘Thunderclap’ headache, including ‘effort’ and coital headache
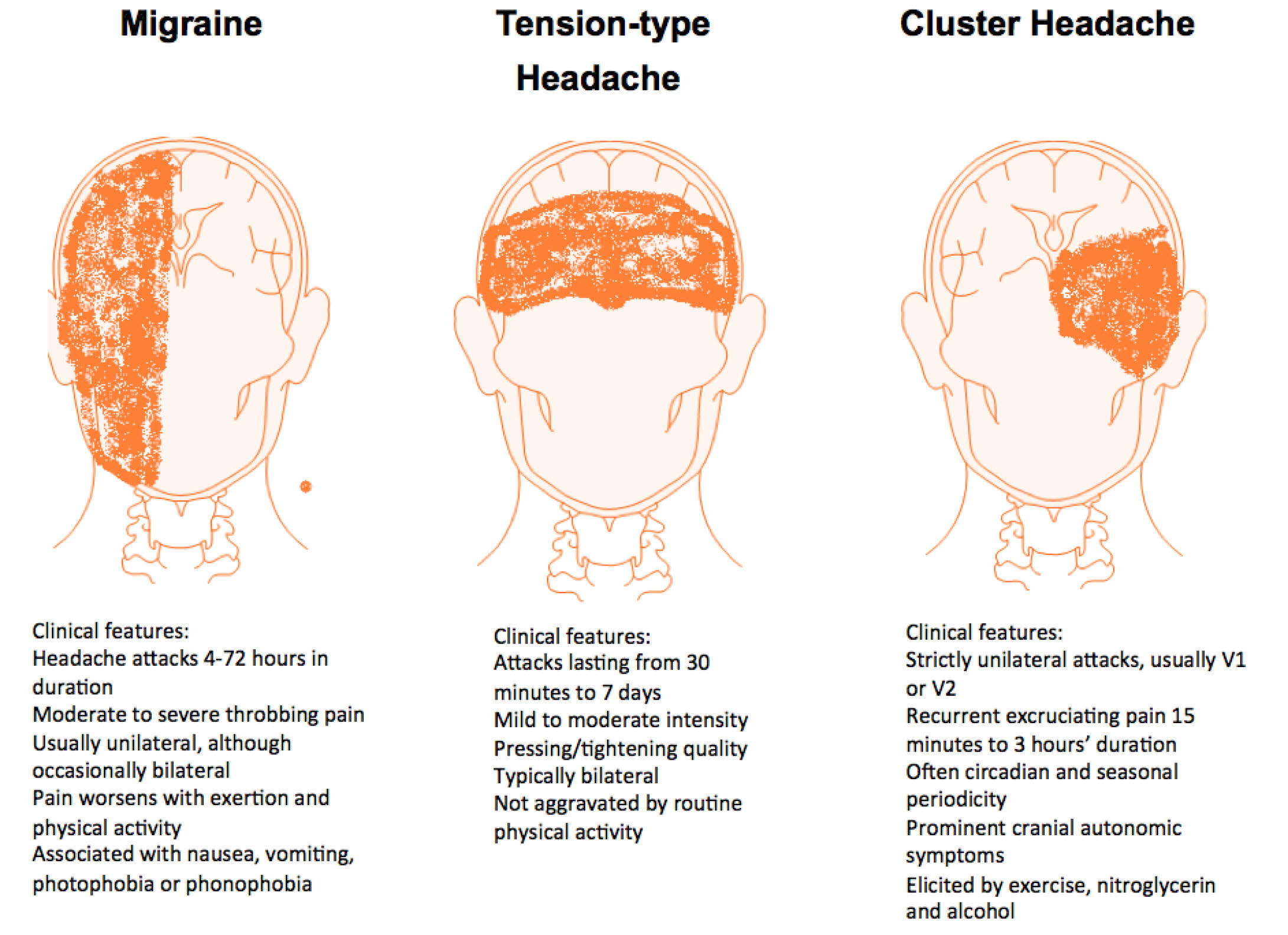
As these conditions are so common and will often be a co-presenting factor in dental patients presenting with orofacial pain, it is important for dentists to be able to identify the three main groups of common headaches (migraine, cluster and tension headaches) (Figure 1). Dentists can also play an important role in identifying possible sinister headaches and appropriately refer their patients for urgent care. Table 2 offers a summary for differentiating between these different headaches.
Figure 1. Diagrammatic representation of various sites for common primary headaches.
Headache feature
Tension-type headache
Migraine (with or without aura)
Cluster headache
Pain location
Bilateral
Unilateral or bilateral
Unilateral (around the eye, above the eye and along the side of the head/face
Pain quality
Pressing/tightening (non-pulsating)
Pulsating (throbbing or banging in young people aged 12-17 years)
Variable (can be sharp, boring, burning, throbbing or tightening)
Pain intensity
Mild or moderate
Moderate or severe
Severe or very severe
Effect on activities
Not aggravated by routine activities of daily living
Aggravated by, or causes avoidance of, routine activities of daily living
Restlessness or agitation
Other symptoms
None
Unusual sensitivity to light and/or sound or nausea and/or vomitingAuraSymptoms can occur with or without headache and:
– are fully reversible
– develop over at least 5 minutes
– last 5-60 minutes
Typical aura symptoms include visual symptoms such as flickering lights, spots or lines and/or partial loss of vision; sensory symptoms such as numbness and/or pins and needles; and/or speech disturbance
On the same side as the headache:
– red and/or watery eye
– nasal congestion and/or runny nose
– swollen eyelid
– forehead and facial sweating
– constricted pupil and/or drooping eyelid
Duration of headache
30 minutes-continuous
4-72 hours in adults 1-72 hours in young people aged 12-17 years
15-180 minutes
Frequency of headache
<15 days per month
≥15 days per month for more than 3 months
<15 days per month
≥15 days per month for more than 3 months
1 every other day to 8 per day, with remission >1 month
1 every other day to 8 per day, with a continuous remission <1 month in a 12− month period
Diagnosis
Episodic tension-type headache
Chronic tension-type headache
Episodic migraine
Chronic migraine
Episodic cluster headache
Chronic cluster headache
The impact of headache disorders is considerable, mainly because it is so common. It is estimated that, in EU countries, direct and indirect cost amounts to €27 billion per year.2 One study in England has reported that 0.5% of all working days are lost due to absenteeism but, in 2% of all working days, workers struggle with reduced capacity from headaches. In a combined study of nearly 400 migraineurs in the UK and US, there were similar rates of family disruption. Eighty-five per cent of patients reported that their headache reduced their ability to perform household chores and 36% said it affected their parenting abilities. Of the 100 partner and spouses of these patients who were interviewed, 29% stated that arguments were more common because of their partner's migraine.
The severity or duration of the headache is usually unhelpful for determining aetiology. Paradoxically, recent onset headaches are more likely to signal a sinister pathology than one that is chronic. The speed of headache onset and other associated features are more helpful for making a diagnosis.
Sudden-onset headache
Sudden-onset headaches are defined as headaches that reach maximum severity within minutes of onset. This type of headache may be the presenting symptom of a number of potentially serious pathologies (Table 1). Physical examination may not be informative. Neuroimaging, usually a CT brain scan, and measurement of cerebrospinal fluid pressure and constituents may be necessary. Depending on the history of presentation, some form of intracranial angiography may also be needed. The majority of investigations are normal and these episodes are termed ‘thunderclap’ headaches.
Other headaches
Most other headaches are subacute or of gradual onset. Careful analysis of the symptoms of the headache is crucial for a correct diagnosis. Two or more types of headache may co-exist or even merge into each other. Where possible, the duration, site, radiation, pattern of onset, character of pain and exacerbating or relieving factors should be noted for every single type of headache. Each of these headaches must then be addressed for the complete alleviation of symptoms.
Headache syndromes
Primary headache syndromes
Headache management is dependent on getting a correct diagnosis. Eliciting a comprehensive history is vital because there are no confirmatory tests for the different primary headache disorders (Figure 1).
Tension-type headache
This is the most common headache. It is difficult to define and the pathogenesis is unclear, although virtually everyone has experienced it. For episodic attacks, simple analgesics are often used.3 It is important to avoid the use of opioids for symptomatic relief of tension headaches. In general, non-pharmacological methods are the preferred initial treatment to reduce the risk of medication overuse.
Behavioural therapy, massage, exercises, hot and cold application, acupuncture and even distraction can be effective. The results from placebo-controlled studies assessing the efficacy of pharmacotherapy are inconclusive. However, where the headache is prolonged, daily prophylactic treatment with a tricyclic, mirtazapine or beta-blocker is preferable to increasing use of NSAIDs or opioids.4
Migraine
Migraine is a recurrent episodic syndrome associated with at least one of the following: nausea/vomiting, photophobia or phonophobia. Osmophobia, neck stiffness, diarrhoea, waterbrash and dizziness are also known associations. Migraine can be divided into attacks with or without aura. Attacks with aura affect about one-fifth of all patients.
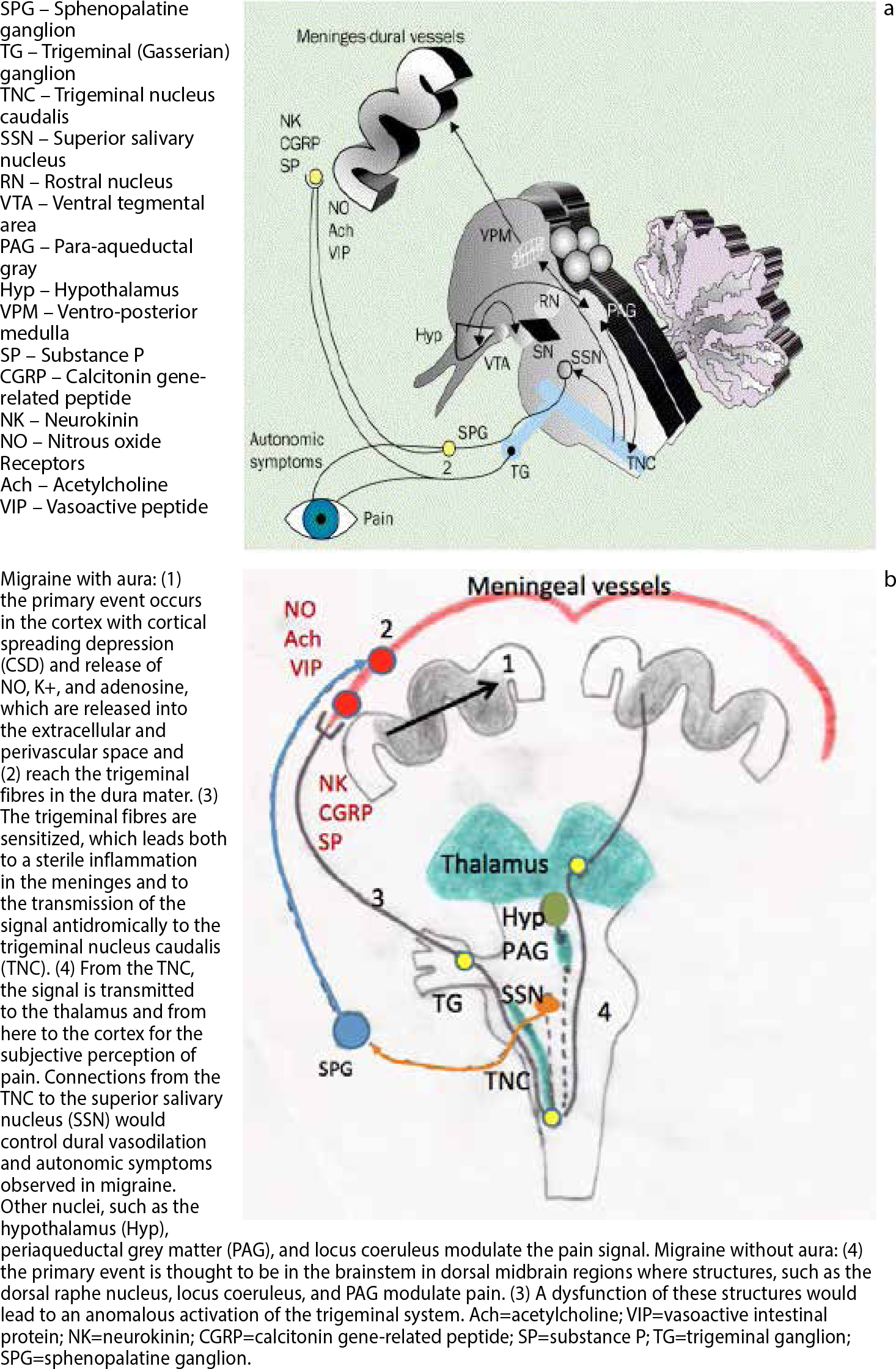
The pathogenesis of migraine is complex but is primarily a neurological event originating from the brainstem followed by the trigemino-cervical complex. The thalamus and cerebral cortex is then involved with secondary vascular changes. Cortical spreading depolarization (CSD), a wave of oligaemia travelling at 2–3 mm/minute is thought to be the mechanism for migrainous auras (Figure 2).
Figure 2.
(a) Neurological basis for migraine involving the trigeminal and cervical nerve (C2 and C3) sensory nerves. The autonomic system is not shown but is also involved. (b) Pathogenetic theory of migraine with and without aura.
The International Headache Society5 definition for migraine without aura is outlined in Table 3. Migraine with aura is defined as the presence of headache with neurological symptoms that last less than 60 minutes and may precede the headache. Visual auras consisting of transient hemianopia, scintillating scotoma or fortification spectra are the most common. Other types of aura include hemisensory loss and hemiparesis, but they are rare.
Headache attacks lasting 4–72 hours (untreated or unsuccessfully treated).2,3
Headache has at least two of the following four characteristics:
Unilateral location;
Pulsating quality;
Moderate or severe pain intensity;
Aggravation by or causing avoidance of routine physical activity (eg walking or climbing stairs).
During headache at least one of the following:
Nausea and/or vomiting;
Photophobia and phonophobia.
Not better accounted for by another ICHD-3 diagnosis.
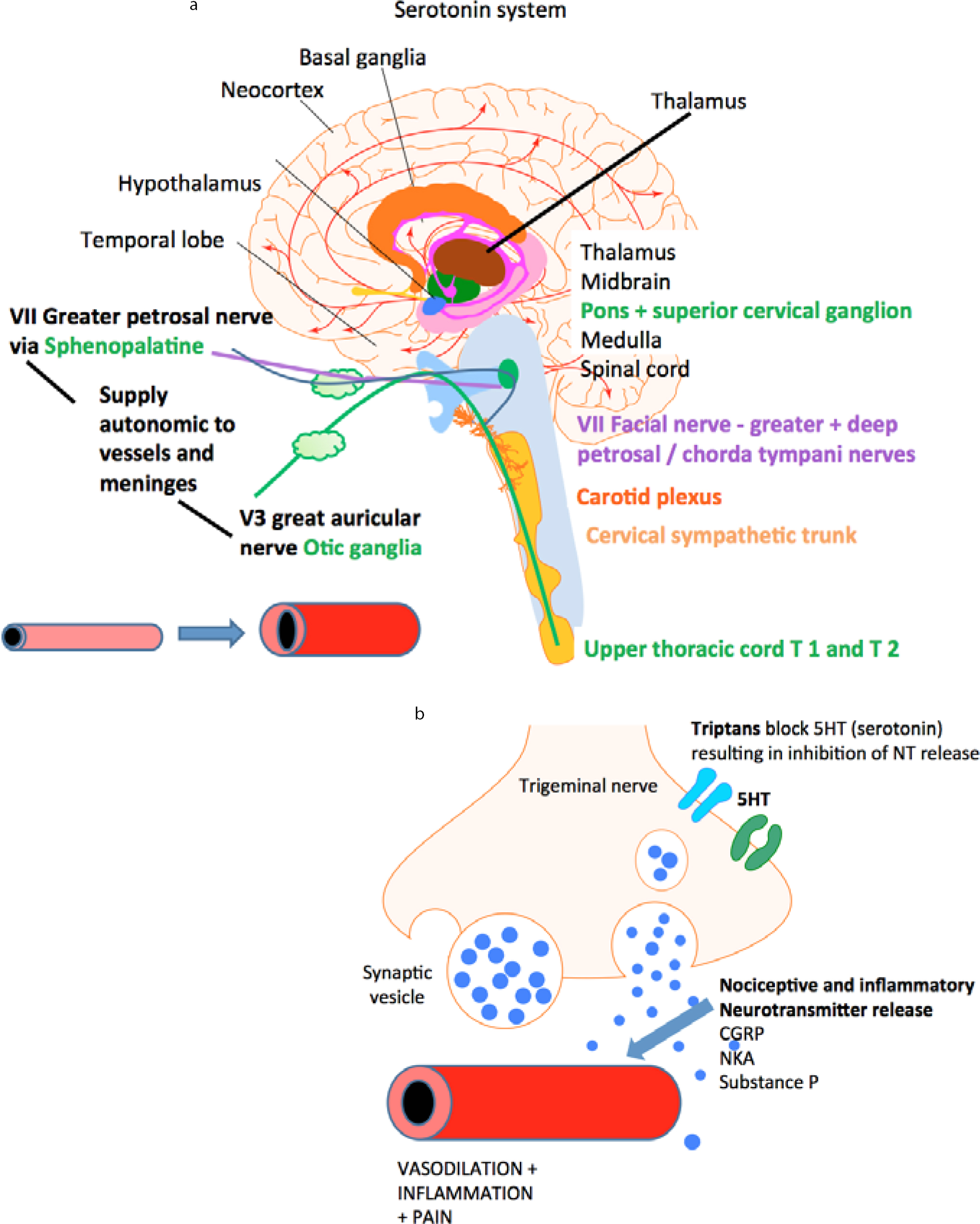
Patients often report sensations of unsteadiness, dizziness and even ataxia. These migraine variants of vestibular disorders and basilar migraine often provoke a lot of anxiety but can be successfully managed with clear explanations and strategies similar to that for other types of migraine. Some patients may have an aura without headache (see below). The vascular basis for migraines is displayed in Figure 3.
Figure 3.
(a) The vascular basis for migraines: secondary vascular changes and ‘sterile inflammation’ in migraine. (b) The proposed mechanism of triptans preventing migraine.
Migraine morbidity: There is evidence that migraine, especially with frequent auras, increases the risk of cardiovascular and cerebrovascular disease. The management of these patients should include advice on modifying other arteriosclerotic risk factors. Oestrogen-containing drugs should be avoided in women with frequent or prolonged migrainous aura. They should also be educated about healthy lifestyle changes and to stop smoking.
Management of migraine: Making the correct diagnosis is crucial, but it is also important to remember that some migraine attacks are secondary to other systemic illnesses, like mitochondrial cytopathies, systemic lupus erthythematosus (SLE), cerebral vasculitis and may be mimicked by others, such as a subarachnoid haemorrhage. For primary migraine attacks a holistic approach is the best way of managing the symptoms.
The following hierarchy of management options is summarized in Table 4. Most patients who have migraine without aura or with visual aura only do not need investigations.
Avoid trigger factors:
Diet: certain foodstuffs like citrus fruits, red wine, cheese, chocolate and nitrites in preserved meat. Missed meals or dehydration;
Disturbed diurnal rhythm: too much or too little sleep, jet lag;
Another headache: eg tension-type, referred pain from neck.
Analgesic and antiemetic combination, eg soluble aspirin 900 mg with domperidone.
Specific treatment: triptan or ergot.
Prophylaxis.
Avoid trigger factors: Numerous internal and external triggers can set off migraine attacks. Hormonal factors are important and the menstrual cycle is a potent trigger in many women. The combined oral contraceptive pill or HRT may prevent as well as exacerbate migraine attacks. Oestrogen supplementation can help but must be weighed against the increased risk of breast neoplasms and venous thrombosis.
External triggers include certain foods, alcohol, stress, strong smells and bright light. Many triggers are relative rather than absolute and a number may combine to precipitate an attack. Avoiding this situation is obviously important.
Acute attacks: For acute attacks, the mixture of an NSAID and an antiemetic is the first-choice treatment. NSAIDs proven to be effective include aspirin, ibuprofen, tolfenamic acid and naproxen. For the antiemetic, domperidone may be preferable to prochlorperazine because it rarely causes oculogyric crises. However, metoclopramide monotherapy has been reported to be effective in alleviating acute migraine attacks in placebo controlled studies. Intravenous chlorpromazine is also reported to be effective in acute attacks.
If the analgesic–antiemetic combination fails to work, more specific treatment may be necessary. Currently seven triptan drugs are licensed in the UK – zolmitriptan, naratriptan, rizatriptan, almotriptan, eletriptan, sumatriptan and frovatriptan. The triptans are usually well tolerated – almotriptan, naratriptan and frovatriptan especially.
Subcutaneous sumatriptan injection has been reported to precipitate coronary artery vasospasm. This is very rare, but a reminder that ischaemic heart disease and/or heavy smoking are relative contra-indications. Triptans should also be used with caution in those who experience prolonged non-visual auras.
The triptans have superseded ergots and isometheptene for treating acute migraine because of reduced risks of side-effects and rebound headaches. However, excessive use of triptans is a common cause of MOH. For the distinguishing features of individual triptans see Table 5.
Drug
Distinguishing characteristic
Almotriptan
One of the more potent triptans
Eletriptan
Higher doses show good efficacy in trials, but have more side-effects
Frovatriptan
Longer half-life may reduce the risk of rebound headaches
Naratriptan
Low incidence of side-effects, but may take longer to work
Rizatriptan
One of the most potent triptans; available as a melt Tablet Clearance may be reduced by propranolol
Sumatriptan
First drug of this class. Can be administered orally, as a nasal spray or via subcutaneous injection. Now available in generic form
Zolmitriptan
Also available as a melt Tablet and nasal spray
There is also evidence that the combination of a triptan taken together with paracetamol or NSAIDs are more effective than one or the other medication on its own. Sometimes, all 3 classes of medications: triptan, NSAID and antiemetic may be taken together to alleviate a migraine attack.
Prophylaxis: Disabling and frequent migraine attacks can be treated with prophylactic medications, but this is dependent on patient choice. The choice of prophylactic treatment and daily dosage is shown in Table 6. The National Institute for Health Care Excellence guideline CG150.5,6 has recommended topiramate or propranolol as the drugs of first choice. Gabapentin is also recommended but the evidence is still controversial.6 Botulinum toxin (Botox®) injections have been recently licensed as a prophylaxis for chronic migraine following results of the PRE-EMPT trials. There are controversies regarding its efficacy because a number of previous studies of episodic migraine have shown that it is ineffective. Many of the patients in the PREEMPT studies also have medication overuse headache. In a separate Health Technology Assessment, NICE has recommended the use of Botulinum toxin in appropriate patients with chronic migraine (NICE 2012 ii).6
Clinically efficacious drugs based on consensus with little evidence from clinical trials: nortriptyline, doxepin, imipramine, sertraline, diltiazem, venlafaxine and mirtazapine
Drugs with proven efficacy, but with concerns over side-effects: methysergide, flunarizine
Drugs shown to be effective with acceptable side-effects: occipital nerve blocks and/or stimulation
Specific migraine types
Hemiplegic migraine
This may be part of the syndrome of familial hemiplegic migraine. There are many other causes of migraine with persistent neurological deficit lasting longer than 60 minutes (migraine with prolonged aura).
Mitochondrial cytopathy and cerebral autosomal dominant arteriopathy with subcortical infarcts with leukoencephalopathy (CADASIL) are examples and these patients need neurological assessment. Patients with hemiplegic migraine should also avoid oestrogen.
Migraine aura without headache
This is defined as absence of headache within one hour of aura. Prophylaxis using aspirin would be appropriate for patients with neurological symptoms but no headaches. Triptans are theoretically contra-indicated but there is little evidence of harm in practice. There is some evidence that antiepileptic drugs, such as lamotrigine and sodium valproate, can be effective as prophylaxis for prolonged migrainous auras.
Status migrainosus
This is defined as migraine that lasts for over three days without remission or where the headache-free interval is less than four hours. Typically, patients are dehydrated with abnormal electrolytes and acid–base balance, usually from prolonged vomiting. Correcting these parameters using IV therapy and pain relief is important. Where available, IV dihydroergotamine may be useful. Otherwise, use subcutaneous sumatriptan. Intravenous lidocaine infusions are sometimes used to terminate a bout of status migrainosus, although firm evidence is not available.
Chronic migraine
Chronic migraine is defined as headaches for more than 15 days a month for which at least 8 days are typical migraine for more than 3 months. In the two PRE-EMPT trials, nearly 1,400 patients were studied and the results demonstrated the benefit of Botox® injections for the prophylaxis of chronic migraine. NICE has recommended the use of Botox® as prophylaxis for chronic migraine in appropriate patients.
Migraine in children
In children, migraine attacks may last for only one hour. Regular eating habits and a snack before physical activities or before bed can be effective. Aspirin is contra-indicated in children and paracetamol or ibuprofen preparations are the treatment of choice.
Sumatriptan tablets are not licensed for children under the age of 18. Use of the nasal spray in adolescents (12–17 years) is recommended by NICE for treating migraine.3 This is a fast-acting effective and well-tolerated method of alleviating acute migraine attacks in youngsters where migraine normally last for less than 4 hours.
Migraine in pregnancy and lactating mothers
Migraine in most women improves with pregnancy. However, some may experience migraine for the first time while pregnant. Migraine tends to be more frequent in the first trimester.
For acute attacks of migraine, paracetamol, codeine and NSAIDs can be used. Triptans are relatively contra-indicated in pregnant women, although drug registers kept by some drug companies appear to show that it is effective and safe. For lactating mothers, it is recommended that they refrain from breast-feeding for 12 hours after taking a dose of triptan.
The safety of tricyclic drugs during pregnancy is unclear and should only be undertaken by experts with careful monitoring. The beta-blockers such as propranolol and nadolol can cause intrauterine growth retardation. In general, pregnant women with frequent and severe migraine should be referred for specialist care.
Where nausea and vomiting is severe, the short-term use of metoclopramide or prochlorperazine in small doses should be helpful. A short course of steroids may also avert severe migraine attacks during pregnancy.
Migraine in the elderly
First onset of migraine in people over the age of 65 years is not as rare as previously thought. However, it is important to rule out other causes of headache in this population.
Apart from temporal arteritis, glaucoma and intracranial mass lesions, a variety of medications may also induce headaches in the elderly. Well-known examples include nitrates and calcium-channel blockers, but aminophylline, sildenafil, dipyridamole and levodopa can also cause cephalalgias. Switching to alternative medications may stop the headaches.
Migraine mimics
There are a number of conditions that can mimic migraine attacks with aura. Two important conditions, which are probably inter-related, are reversible cerebral vasoconstriction syndrome or the Call-Fleming syndrome and HaNDL. The headache in Call-Fleming syndrome is typically of faster onset than migraine and there may be neurological deficits very similar to migrainous auras. The diagnosis is made by intra-cerebral arteriography that may show vascular beading and narrowing. Steroids and nimodipine have been used for treating this condition but there is little published evidence for this.
In HaNDL or Headache with Neurological Deficit and cerebrospinal Lymphocytosis, patients present as migraine with aura attacks or even as someone having a stroke. Simultaneous hypoperfusion in multiple arterial territories in a patient with few vascular risk factors should alert the clinician to this possibility. The lumbar puncture is also abnormal with raised cells and commonly protein as well. It is important to differentiate between HaNDL and stroke to avoid unnecessary thrombolysis.
Cluster headache
This is less common than migraine and is characterized by unilateral, severe boring pain centred around one eye that lasts for around 20–60 minutes. Nasal congestion and tearing are commonly associated symptoms. Horner's syndrome with conjunctival hyperaemia may also be present (Table 2).
Repeated attacks come on at the same time of the day and bouts are more common during the winter equinox and summer solstice. Risk factors are heavy tobacco, alcohol and coffee consumption in middle-aged men with a family history of cluster headaches.
For acute attacks, subcutaneous sumatriptan is the treatment of choice. Intranasal zolmitriptan has been shown to be effective and breathing 100% oxygen via a high-flow mask is an alternative. Prophylactic treatment with verapamil, lithium, ergot and melatonin are effective, although a course of oral steroids will also shorten a cluster bout. Ipsilateral occipital nerve blocks using a mixture of local anaesthetics and steroids may also work.3
Paroxysmal hemicrania
This is another unilateral headache syndrome with some features similar to cluster headaches. It is more prevalent in females with shorter and more frequent attacks. Prompt relief with indometacin in doses of 75–225 mg/day can also help with the diagnosis.
SUNCT and SUNA (article 9)
Short lasting Unilateral Neuralgiform pain with Conjunctival Injection (SUNCT) and Short lasting Unilateral Neuralgiform pain with cranial Autonomic features (SUNA) are two related disorders.6,7 There may also be a link with trigeminal neuralgia. The attacks tend to be short-lasting, 1–2 minutes in duration, but may have a frequency of over 60 attacks a day. The pain is strictly unilateral and there may be background aching pain superimposed on the stabs. The autonomic features help in making this diagnosis. Lamotrigine is the treatment of choice, although gabapentin, topiramate and occipital nerve blocks have also been reported to be effective.
Primary stabbing headache
Also called ‘ice-pick’ headaches, these are sharp, stabbing pains that last for seconds with multiple recurrences. There may also be a background continuous headache. Unlike the trigeminovascular headaches (cluster headache, paroxysmal hemicrania, SUNCT and SUNA), the area involved may change and spread to the opposite side is common. This type of headache is not associated with autonomic features, but may still respond to treatment with indometacin.
Secondary headache syndromes
Giant cell arteritis (GCA)
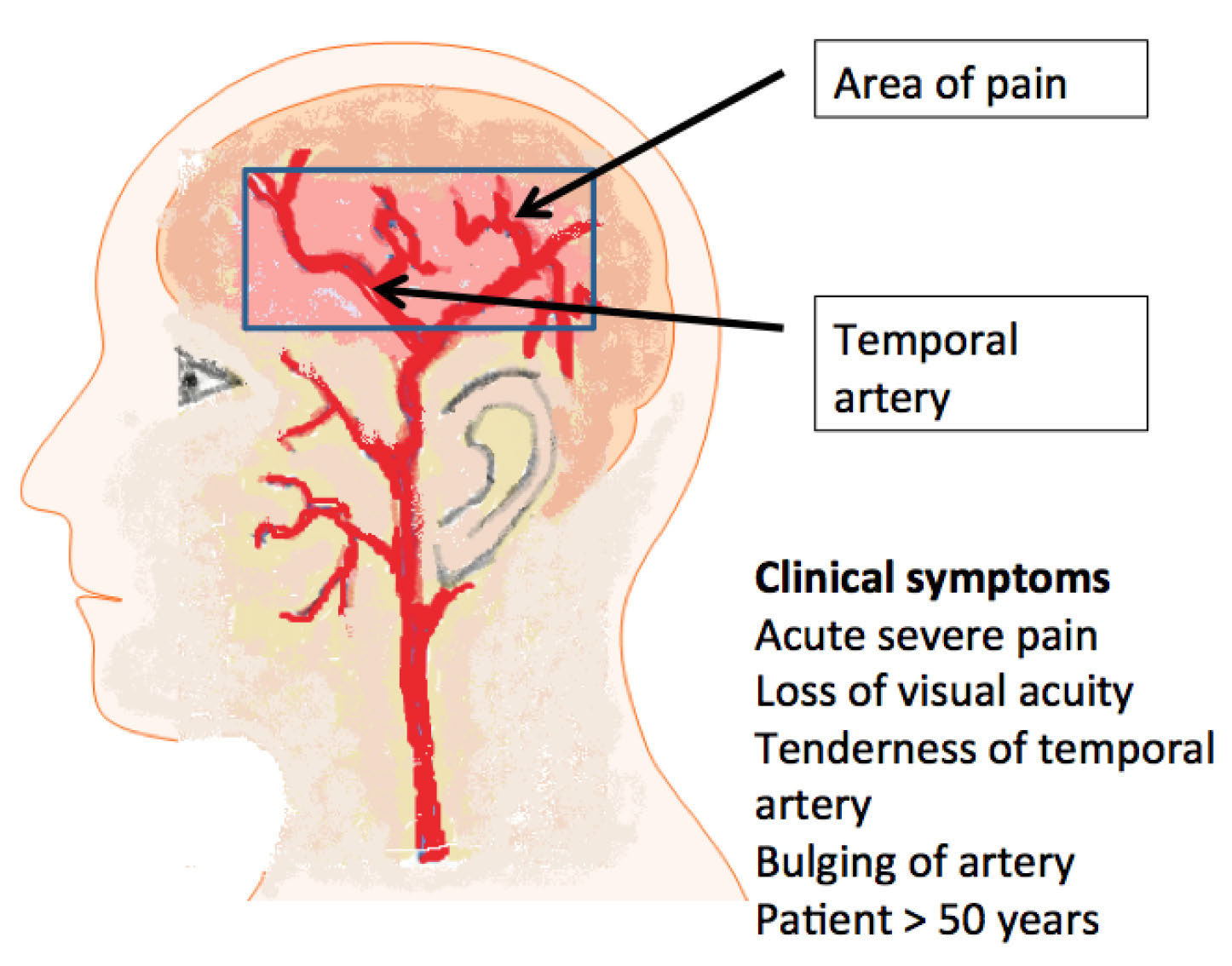
Also known as temporal arteritis, this is a rare secondary headache syndrome that is difficult to diagnose, but uncommon in those under the age of 60 years. Headaches in GCA are usually persistent and chronic, but patients may also have intermittent attacks. Associated features are jaw claudication and tender, non-pulsatile temporal arteries. Polymyalgia often co-exists with GCA and the symptoms can be so insidious that patients may be misdiagnosed with depression. The risk of optic nerve head infarction causing blindness means that early diagnosis and treatment with steroids are crucial. The erythrocyte sedimentation rate is usually raised but there are rare cases where it can be within the normal range. Temporal artery biopsy to confirm GCA is essential but this should not delay steroid therapy, as biopsies may still be positive up to one week after starting treatment (Figure 4).
Figure 4. Diagrammatic representation of the clinical picture of temporal arteritis.
Pseudotumour cerebri
Also known as benign intracranial hypertension (BIH). However, the risk of blindness from optic nerve and macular damage means that the condition is not, in fact, benign. It commonly affects young women who are overweight and have menstrual irregularities. The oral contraceptive pill, retinoids and tetracyclines are drugs associated with the development of BIH. Papilloedema may be the only sign on examination but an enlarged blind spot and constricted peripheral visual fields form specific parts of the diagnosis. Investigations are important to rule out sinus venous thrombosis or an intracranial space-occupying lesion. Ophthalmological assessment with visual field charting and fundoscopy or slit lamp examination is crucial to monitor this condition.
Intracranial hypotension
Spontaneous intracranial hypotension is increasingly recognized as a cause of chronic headache. The diagnostic feature of this condition is headache exacerbation within minutes of being upright and near resolution with recumbency. Nausea, vomiting, dizziness are commonly associated features. MRI scans may show tonsillar herniation, dural enhancement with gadolinium or even reactive subdural haemorrhage. Symptom alleviation with analgesics, good hydration and strict bed rest will help. The role of epidural blood patch is controversial. There is little published evidence that caffeine works, even though it is commonly used. Symptoms can persist for months and it is important to inform patients about this.
Medication overuse headache (MOH)
The definition of medication overuse is someone taking simple analgesics more than 15 days a month, or opioids, triptans, ergot or combination medications more than 10 days a month. Population studies have reported the prevalence of MOH to be around 1–1.5% and up to 2.6% in women only.8
Withdrawal from medication overuse has been shown to be successful, but there is a high risk of relapse, with an estimated incidence of nearly 50% in five years. Structural and functional imaging changes have been reported with MOH and these reverted back to normal with successful withdrawal.
Patient education is crucial for managing MOH and it is important to remove the triggers for headache as well as exploring non-pharmacological options for these patients. Prophylactic medications may only be necessary in 50% of patients if they successfully withdraw from the offending analgesic.
Who to investigate?
Investigations of headache patients should be confined to those with specific indications (Table 7). Otherwise, careful clinical assessment leading to the correct diagnosis and reassurance with advice is all that is necessary in most patients.
History suggestive of focal neurological dysfunction
Previous history of malignant neoplasm
Previous history of chronic infection, including HIV
Examination revealed neurological abnormality
Patient has altered sensorium
Headache is of sudden onset
Headache is associated with other symptoms, eg fever and weight loss, neck stiffness
Course of headache not corresponding to the presumed diagnosis
Repeat attendances with the same symptoms
Failure to assure patient that headache is benign in nature
Headache as the sole presenting symptom for brain tumours is rare. However, some features, such as morning predominance and pain worsening with coughing, sneezing or straining, may indicate raised intracranial pressure and help to refine the diagnostic process.
Neuroimaging with CT or MRI is not a cost-effective way of making a diagnosis for headaches. These investigations have poor specificity and sensitivity, especially in certain important syndromes like pseudotumour cerebri. The pragmatic clinician must also recognize that the reassurance of a normal brain scan can itself be therapeutic. However, this is only useful if all other avenues have been exhausted and performing one test does not lead to demands for other investigations.3