Matharu M, Goadsby P Trigeminal autonomic cephalalgias: diagnosis and management, 8th edn. In: Silberstein S, Lipton R, Dodick D New York: Oxford University Press; 2007
Bahra A, May A, Goadsby PJ Cluster headache: a prospective clinical study with diagnostic implications. Neurology. 2002; 58:(3)354-361
Russell MB Epidemiology and genetics of cluster headache. Lancet Neurol. 2004; 3:(5)279-283
Leone M, Russell MB, Rigamonti A Increased familial risk of cluster headache. Neurology. 2001; 56:(9)1233-1236
Cittadini E, Matharu MS, Goadsby PJ Paroxysmal hemicrania: a prospective clinical study of 31 cases. Brain. 2008; 131:(4)1142-1155
Goadsby PJ, Lipton RB A review of paroxysmal hemicranias, SUNCT syndrome and other short-lasting headaches with autonomic feature, including new cases. Brain. 1997; 120:(1)193-209
Benoliel R, Elishoov H, Sharav Y Orofacial pain with vascular-type features. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 84:(5)506-512
Antonaci F, Sjaastad O Chronic paroxysmal hemicrania (CPH): a review of the clinical manifestations. Headache. 1989; 29:(10)648-656
Matharu MS, Boes CJ, Goadsby PJ Management of trigeminal autonomic cephalalgias and hemicrania continua. Drugs. 2003; 63:(16)1637-1677
Cohen AS, Matharu MS, Goadsby PJ Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT) or cranial autonomic features (SUNA) – a prospective clinical study of SUNCT and SUNA. Brain. 2006; 129:(10)2746-2760
Matharu MS, Cohen AS, Boes CJ, Goadsby PJ Short-lasting unilateral neuralgiform headache with conjunctival injection and tearing syndrome: a review. Curr Pain Headache Rep. 2003; 7:(4)308-318
May A, Goadsby PJ The trigeminovascular system in humans: pathophysiologic implications for primary headache syndromes of the neural influences on the cerebral circulation. J Cereb Blood Flow Metab. 1999; 19:(2)115-127
Benoliel R, Sharav Y Trigeminal neuralgia with lacrimation or SUNCT syndrome?. Cephalalgia. 1998; 18:(2)85-90
Goadsby PJ, Matharu MS, Boes CJ SUNCT syndrome or trigeminal neuralgia with lacrimation. Cephalalgia. 2001; 21:82-83
Goadsby PJ Trigeminal autonomic cephalalgias: fancy term or constructive change to the IHS classification?. J Neurol Neurosurg Psych. 2005; 76:(3)301-305
Leone M, Bussone G Pathophysiology of trigeminal autonomic cephalalgias. Lancet Neurol. 2009; 8:(8)755-764
May A, Bahra A, Buchel C Hypothalamic activation in cluster headache attacks. Lancet. 1998; 352:(9124)275-278
Matharu MS, Cohen AS, McGonigle DJ Posterior hypothalamic activation in paroxysmal hemicrania. Ann Neurol. 2006; 59:(3)535-545
May A, Bahra A, Büchel C Functional magnetic resonance imaging in spontaneous attacks of SUNCT: short-lasting neuralgiform headache with conjunctival injection and tearing. Ann Neurol. 1999; 46:(5)791-794
Cohen A Functional MRI in SUNCT shows differential hypothalamic activation with increasing pain. Cephalalgia. 2004; 24:1098-1099
Sprenger T, Valet M, Platzer S SUNCT: bilateral hypothalamic activation during headache attacks and resolving of symptoms after trigeminal decompression. Pain. 2005; 113:(3)422-426
May A, Kaube H, Buchel C Experimental cranial pain elicited by capsaicin: a PET study. Pain. 1998; 74:(1)61-66
Malick A, Burstein R Cells of origin of the trigeminohypothalamic tract in the rat. J Comp Neurol. 1998; 400:(1)125-144
Wang Q, Mao LM, Han JS Naloxone-reversible analgesia produced by microstimulation of the arcuate nucleus of the hypothalamus in pentobarbital-anesthetized rats. Exp Brain Res. 1990; 80:(1)201-204
Dafny N, Dong WQ, Prieto-Gomez C Lateral hypothalamus: site involved in pain modulation. Neuroscience. 1996; 70:(2)449-460
Lumb BM, Lovick TA The rostral hypothalamus: an area for the integration of autonomic and sensory responsiveness. J Neurophysiol. 1993; 70:(4)1570-1577
Benjamin LA, Levy MJ, Lasa MP, Goadsby PJ Hypothalamic activation after stimulation of the superior sagittal sinus in the cat: a Fos study. Neurobiol Dis. 2004; 16:(3)500-505
Bartsch T, Levy MJ, Knight Y, Goadsby PJ Differential modulation of dural nociception to Orexin A and B receptor activation in the posterior hypothalamic area. Pain. 2004; 109:(3)367-378
Holle D, Katsarava Z, Obermann M The hypothalamus: specific or nonspecific role in the pathophysiology of trigeminal autonomic cephalalgias?. Curr Pain Headache Rep. 2011; 15:(2)101-107
Denuelle M, Fabre N, Payoux P Hypothalamic activation in spontaneous migraine attacks. Headache. 2007; 47:(10)1418-1426
Matharu MS, Cohen AS, McGonigle DJ Posterior hypothalamic and brainstem activation in hemicrania continua. Headache. 2004; 44:(8)747-761
Holle D, Naegel S, Krebs S Hypothalamic gray matter volume loss in hypnic headache. Ann Neurol. 2011; 69:(3)533-539
Bittar G, Graff-Radford SB A retrospective study of patients with cluster headaches. Oral Surg Oral Med Oral Pathol. 1992; 73:(5)519-525
Brooke RI Periodic migrainous neuralgia: a cause of dental pain. Oral Surg Oral Med Oral Pathol. 1978; 46:(4)511-516
Bahra A, Goadsby PJ Diagnostic delays and mis-management in cluster headache. Acta Neurol Scand. 2004; 109:(3)175-179
D'Andrea G, Granella F, Ghiotto N, Nappi G Lamotrigine in the treatment of SUNCT syndrome. Neurology. 2001; 57:(9)1723-1725
Matharu MS, Boes CJ, Goadsby PJ SUNCT syndrome: prolonged attacks, refractoriness and response to topiramate. Neurology. 2002; 58:(8)
Graff-Radford SB SUNCT syndrome responsive to gabapentin. Cephalalgia. 2000; 20:(5)515-517
Pain part 9: trigeminal autonomic cephalalgias Norazah Abu Bakar Manjit Matharu Tara Renton Dental Update 2024 43:4, 707-709.
Authors
NorazahAbu Bakar
BDS, MFDS RCSEd, MSurgDent RCSEd, PhD, FDS RCSEd
Dental Institute, King's College London, Denmark Hill, London SE5 9RS and Headache Group, Institute of Neurology, The National Hospital for Neurology and Neurosurgery
Senior Lecturer and Honorary Consultant Neurologist, Headache Group, Institute of Neurology, The National Hospital for Neurology and Neurosurgery, Queen Square, London WC1N 3BG
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
The trigeminal autonomic cephalalgias are a group of rare, highly disabling, primary headache syndromes distinctly characterized by the unilaterality of their attacks and presence of cranial autonomic symptoms. Although pain is often localized to the peri-orbital and temporal regions, it is not uncommon for pain to radiate to tooth-bearing areas and mimic toothache or jaw pain. Hence, dental practitioners should be aware of these syndromes to enable appropriate referral and avoid unnecessary, and often irreversible, dental treatments. Many dentists will not have heard of these conditions but must remain vigilant, and ensure that they are not confused with trigeminal neuralgia, so that their patients are appropriately advised and referred.
CPD/Clinical Relevance: The dental practitioners may be the first line of healthcare providers consulted by these patients in the hope of obtaining pain relief. Lack of familiarity with an uncommon condition may lead to poor patient management.
Article
The trigeminal autonomic cephalalgias (TACs) are a group of rare, short-lasting primary headache disorders that are characterized by strictly unilateral attacks of pain occurring in association with cranial autonomic symptoms. This group comprises cluster headache, paroxysmal hemicrania and short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT). Although these disorders are rare, patients may nonetheless present to their dental practitioners seeking possible treatment, especially since the pain may mimic dental pain or other orofacial pain conditions. It is therefore important that dental professionals are aware of these syndromes to enable better patient management and avoid unnecessary dental treatments.
Cluster headache
The revised International Classification of Headache Disorders (ICHD-II) describes cluster headache (CH) as a rare primary headache characterized by attacks of severe, strictly unilateral pain which is orbital, supra-orbital or temporal (Table 1).1
Diagnostic Criteria
At least 5 attacks fulfilling B-D.
Severe or very severe unilateral orbital, supra-orbital and/or temporal pain lasting 15 to 180 minutes if untreated.
Headache is accompanied by at least one of the following:
Attacks have a frequency from 1 every other day to 8 per day.
Not attributed to another disorder.
Each cluster headache attack is excruciating, typically described by patients as the worst pain they have ever felt (even worse than trigeminal neuralgia!), resulting in patients being unable to cope with the recurrent attacks. Female patients invariably report that each attack is worse than childbirth. Patients are known to develop suicidal ideations, hence it is sometimes known as ‘suicide headaches’. Pain is often described as thermal or punctate in character, like ‘a hot red poker in the eye’.2 Alcohol, nitroglycerin, heat and the smell of volatile substances such as perfumes, solvents and varnish are known to be potent triggers for the headaches during a cluster period.2,3
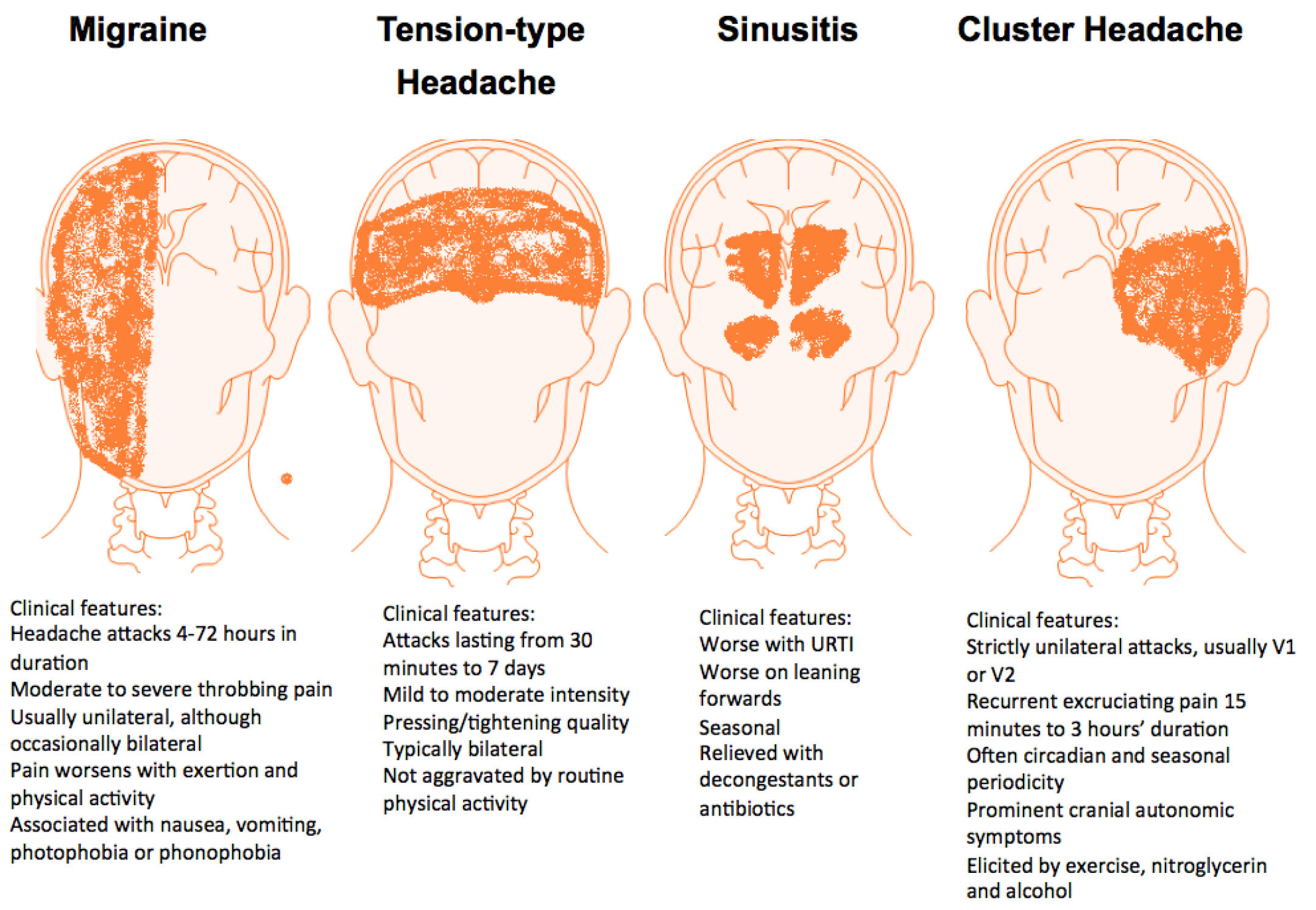
Up to 15% of patients may experience side-shifting of their headaches between attacks, while each individual attack remains strictly unilateral.3 It is of interest to note that, in a prospective clinical study of 230 cluster headache patients, 50% experienced pain in their upper teeth and 32% in the lower teeth, while 45% had jaw pain associated with the attacks.4 Each attack typically lasts 15–180 minutes and may occur from once every other day to 8 times daily. The attacks are associated with marked ipsilateral cranial autonomic symptoms, including lacrimation, conjunctival injection, nasal congestion, rhinorrhoea, forehead and facial sweating, miosis, ptosis or eyelid oedema. Patients may also experience migrainous symptoms such as nausea, vomiting, photophobia and phonophobia. Most patients are restless or agitated during an attack and may describe banging their head against the wall or floor (Figure 1).
Figure 1. Diagram of key features of cluster headache compared with other headaches.
Cluster headache typically occurs in bouts, which last for weeks or months. This is separated by remission periods usually lasting months or years and, on average, patients will experience 1–2 cluster bouts per annum, with each bout lasting 1–2 months. However, about 10% of patients have chronic symptoms, with no remission periods for one year, or remission periods lasting less than a month.1
A striking feature of cluster headache is its diurnal and seasonal periodicity. The attacks have a tendency to occur at specific times of the day and patients are often woken up shortly after falling asleep at night, during the first rapid eye movement (REM) sleep phase, hence its name ‘alarm-clock headaches’. Similarly, the cluster periods or bouts often start in the same month, with a preponderance for onset in spring or autumn.
The prevalence of cluster headache was estimated to be about 1 per 1000 population but recent studies have indicated that it may be as high as 1 per 500 of the adult population.5 The disorder is more common in males, with a male: female ratio of 2.5–7.2:1.3 The age of onset is usually 20–30 years, although it may present at any age.
Cluster headache was previously thought to be a sporadic disorder, but recent studies suggest that there is a genetic component associated with this headache. There is a positive family history in 20% of families, with up to a 39-fold increased risk of cluster headache in first-degree relatives and an 8-fold increased risk in second-degree relatives.6 The actual aetiology is unknown but assumed to be predominantly genetic in basis. The neurological pathways involved are presumed to be the trigeminal, C2 and C3 sensory nerves and the parasympathetic system routed mainly via the otic, ciliary and pterygopalatine ganglia (via ninth, third and fifth cranial nerves, respectively) (Figure 2).
Figure 2.
(a) Summary of autonomic supply to head and neck and (b) chart illustrating neural pathways involved in TACs.
Paroxysmal hemicrania
Paroxysmal hemicrania have similar characteristics of pain to cluster headaches but vary in their duration and frequency (Table 2). The attacks tend to be shorter-lasting, around 2–30 minutes, with an attack frequency of more than 5 per day for more than half of the time, though it can range from 1–40 attacks daily.1 As in cluster headache, patients with paroxysmal hemicrania can demonstrate circadian periodicity, though it tends to be less prominent.7 Initially, the pain may be throbbing as it intensifies, although it is typically sharp or boring, and may be followed by an interictal background pain.8 The attacks are associated with the same autonomic symptoms and signs as cluster headaches. In some patients, attacks may be triggered by head or neck movements. Interestingly, it has been reported that, in up to 15% of cases, the pain may be referred intra-orally.9,10
Diagnostic Criteria
At least 20 attacks fulfilling B-D.
Severe unilateral orbital, supra-orbital, or temporal pain lasting 2-30 minutes.
Headache is accompanied by at least one of the following:
Attacks have a frequency above 5 per day for more than half the time, although periods with lower frequency may occur.
Attacks are prevented completely by therapeutic doses of indometacin*
*To rule out an incomplete response, indometacin should be used in a dose of ≥150 mg daily orally or rectally, or ≥100 mg by injection. Smaller doses are often sufficient for maintenance.
A remarkable feature of this headache is its dramatic and absolute response to therapeutic doses of indometacin.1 Indometacin is given up to a dose of 150 mg/day orally and complete resolution of the headache is prompt, usually occurring within 1–2 days of initiating the effective dose, though in some cases there can be a longer delay of 7–10 days.3,11
The incidence and prevalence of paroxysmal hemicrania is not known, but the relationship compared to cluster headache is reported to be approximately 1–3%.10 Given that the prevalence of cluster headache is approximately 1 per 1000,5 the prevalence of paroxysmal hemicrania would be approximately 1 per 50,000. Unlike cluster headache, paroxysmal hemicrania seems to occur equally in males and females.7 The typical age of onset is usually around 30–40 years, although it may present at any age.
Short-lasting unilateral neuralgiform headache attacks with conjunctival injection and tearing (SUNCT)
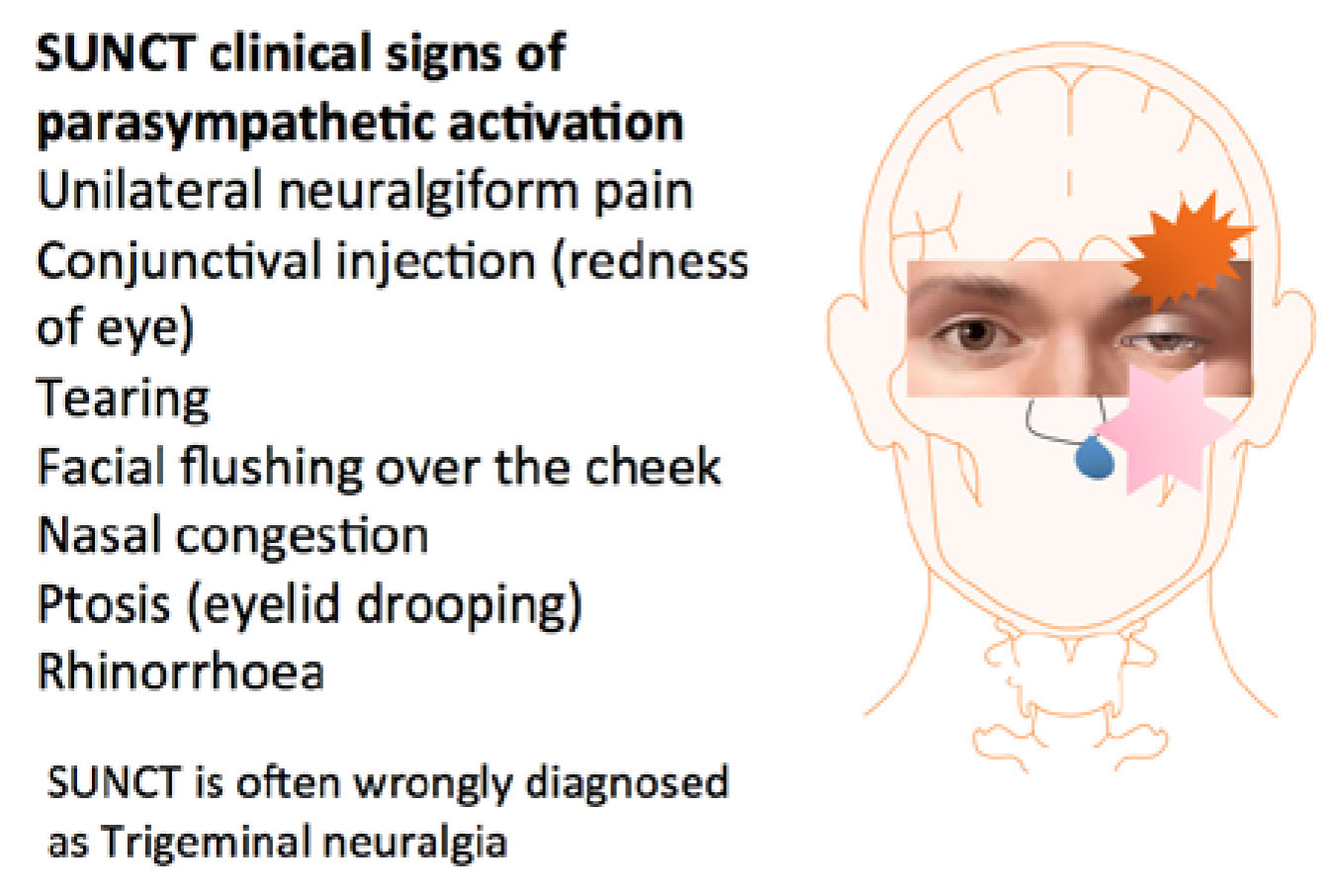
SUNCT is characterized by attacks that are much briefer than cluster headache and paroxysmal hemicrania. Attacks are usually described as stabbing, electric-shock like or pulsating in character, and last 5–240 seconds, with an average duration of 10–60 seconds (Table 3). The attacks occur at a high frequency, ranging from 3–200 per day.1 Attacks may take different forms, being either single stabs, a group of stabs or follow a ‘saw-tooth’ pattern, whereby pain does not return to baseline between the stabs.12 This may create the illusion of a single long attack, rather than multiple short attacks, hence the importance of obtaining a good history. By definition, the pain is accompanied by ipsilateral conjunctival injection and lacrimation, with the other autonomic features being less prominent (Figure 3).2
Diagnostic Criteria
At least 20 attacks fulfilling criteria B-E.
Attacks of unilateral orbital, supra-orbital or temporal stabbing or pulsating pain lasting 5-240 seconds.
Pain is accompanied by ipsilateral conjunctival injection and lacrimation.
Attacks occur with a frequency from 3 to 200 per day.
Not attributed to another disorder.
Figure 3. Diagrammatic illustration of SUNCT clinical signs including, conjunctival injection and tearing, facial swelling and redness, rhinorrhoea and nasal congestion (all associated with autonomic neural activity). It is often wrongly diagnosed as trigeminal neuralgia.
Attacks may be triggered cutaneously, by touching or washing the face, eating, chewing, brushing the teeth, talking or by wind blowing on the face.12 In this respect, SUNCT displays certain similarities to trigeminal neuralgia. However, in trigeminal neuralgia, the attacks are usually of shorter duration, ranging from a fraction of a second to two minutes.13 Moreover, trigeminal neuralgia presents mainly in the maxillary or mandibular divisions of the trigeminal nerve, whereas SUNCT presents predominantly in the ophthalmic division. Most trigeminal neuralgia patients have a refractory period, whereby they are unable to trigger an attack immediately following the previous one. This is not seen in SUNCT and is a useful feature to note when comparing these two disorders (Table 4).8,12
Feature
SUNCT
Trigeminal Neuralgia
Male:female ratio
1.5:1
1:2
Site of pain
V1
V2/3
Duration
5-240 (secs)
<5 secs - 2 mins
Autonomic features
Prominent
Sparse or none
Refractory period
Absent
Present
SUNCT tends to present at a later age in comparison to the other TACs, with typical age of onset around 40–70 years. There is a male predilection for the syndrome with male:female ratio of 1.5:1.12 SUNCT must be considered an important differential diagnosis to trigeminal neuralgia and may explain that, if misdiagnosed, the ‘TN’ patient responds to neither tegretol nor microvascular decompression.
Pathophysiology
Any pathophysiological construct for TACs must account for the three major clinical features characteristic of the various conditions that comprise this group:
Trigeminal distribution of pain;
Ipsilateral cranial autonomic features; and
The distinct circadian and circannual periodicity, especially in cluster headache.
The pain-producing innervation of the cranium projects through branches of the trigeminal and upper cervical nerves to the trigeminocervical complex from whence nociceptive pathways project to higher centres (Figure 2). This implies an integral role for the ipsilateral trigeminal nociceptive pathways in TACs. The ipsilateral autonomic features suggest cranial parasympathetic activation (lacrimation, rhinorrhoea, nasal congestion and eyelid oedema) and sympathetic hypofunction (ptosis and miosis). It has been suggested that the pathophysiology of the TACs revolves around the trigeminal-autonomic reflex.8 There is considerable experimental animal literature to document that stimulation of trigeminal afferents can result in cranial autonomic outflow; the trigeminal-autonomic reflex.14 In fact, some degree of cranial autonomic symptomatology is a normal physiologic response to cranial nociceptive input and patients with other headache syndromes often report these symptoms.15 The distinction between the TACs and other headache syndromes is the degree of cranial autonomic activation and not its presence.16,17
The cranial autonomic symptoms may be prominent in the TACs due to a central disinhibition of the trigeminal-autonomic reflex.18 Supporting evidence is emerging from functional imaging studies: positron emission tomography studies in cluster headache19 and paroxysmal hemicrania,20 and functional MRI studies in SUNCT syndrome21,22,23 have demonstrated hypothalamic activation. Importantly, the involvement of posterior hypothalamic structures may account for the rhythmicity or periodicity that is such a hallmark of cluster headache. Hypothalamic activation is not seen in experimental trigeminal distribution head pain.24 There are direct hypothalamic-trigeminal connections.25 There is abundant evidence for a role of the hypothalamus in mediating anti-nociceptive26,27 and autonomic responses.28 In fact, there is direct evidence from animal experimental studies for hypothalamic activation when intracranial pain structures are activated.29 Moreover, the hypothalamic peptides Orexin A and B can elicit pronociceptive and anti-nociceptive effects in the trigeminal system.30 These data have led to the suggestion that the TACs are probably due to an abnormality in the hypothalamus with subsequent trigeminovascular and cranial autonomic activation.
An important consideration is that the studies outlined above are unable to resolve the paramount question of whether the detected hypothalamic alterations are pathognomonic for TAC, or whether they merely represent an epiphenomenon of different pain conditions in general. It has recently been argued that hypothalamic derangements may not be specific to TACs.31 Hypothalamic activation and structural alterations are not exclusively observed in TAC but can also be found in other primary headache disorders, including migraine,32 hemicrania continua,33 and hypnic headache.34 Further research is certainly needed to ascertain definitively the pathophysiological basis of the TACs.
Diagnosis
The clinical features of the TAC syndromes are relatively stereotyped and thus, as with all pain conditions, the key to diagnosing them is a detailed and systematic patient history. Information regarding the site, laterality, quality and severity of the attacks must be elicited. Emphasis should be given to determining the duration and frequency of each attack, as well as the duration and frequency of the bouts and remission periods. As mentioned previously, in SUNCT, attacks may present in various clinical forms, thus it is important to ascertain this through the history, to arrive at a correct diagnosis. Other diagnostic features of the TAC syndromes that distinguish them from other pain disorders are the circadian and circannual periodicity, the predilection for nocturnal attacks in cluster headaches and the presence of prominent cranial autonomic symptoms ipsilateral to the pain. There may be trigger factors present, especially in SUNCT, which should also be noted. A summary of the clinical characteristics of the TAC syndromes is provided in Table 5.
Sumatriptan injection Sumatriptan or Zolmitriptan nasal spray Oxygen
Nil
Nil
Prophylactic treatment
VerapamilMethysergideLithiumTopiramate
Indometacin
LamotrigineTopiramateGabapentin
Transitional treatment
CorticosteroidsGONB
GONB
GONB
Key: +, ++ indicates the degree of response;
prominent conjunctival injection and lacrimation by definition; SUNCT, Short-lasting Unilateral Neuralgiform headache attacks with Conjunctival injection and Tearing; IV, intravenous; GONB, Greater Occipital Nerve Block.
Although the dental practitioner is not expected to manage these rare conditions, they are expected to at least have knowledge of them, so that any patient who presents with orofacial pain of doubtful diagnosis can be referred accordingly. Pain perceived in the teeth or jaws may actually arise or radiate from elsewhere, and this should always be kept in mind when dental examination is unremarkable and there is no radiographic evidence of periapical or periodontal lesions.35 These syndromes may also masquerade as temporomandibular disorders, thus it is vital to establish a correct diagnosis prior to implementing treatment for myofascial pain.36 It is of interest to note that several studies have actually reported misdiagnosis and mismanagement of these syndromes by dental practitioners. Bahra and Goadsby directly interviewed 230 cluster headache patients and found that 45% consulted a dentist prior to neurologic referral.37 Of these, 18% had unnecessary dental treatment instituted in an attempt to alleviate pain. Treatments received included tooth fillings and extractions, splint therapy, orthodontic treatment and maxillofacial surgery. Also noteworthy from this study is the time it takes for a cluster headache patient to receive a correct diagnosis. The mean time to diagnosis within the past decade was 2.6 years, with 70% of patients having seen another specialist, of which one may be a dentist. Similarly, Bittar and Graff-Radford performed a retrospective study of 33 cluster headache patients and reported that 42% of these patients were seen by dentists prior to referral to the pain management centre and underwent some form of dental treatment, without favourable outcome.35 An oral appliance was constructed for six (42%) of these patients, aimed to treat temporomandibular myofascial pain dysfunction syndrome. Four patients had teeth extracted, three underwent coronoplasty (tooth grinding) procedures, and two had endodontic treatment.
Regarding descriptors and presentation of pain, a clinical review of 35 cluster headache patients found that 57% of the patients described their pain as ‘toothache’, whilst 43% thought it was jaw pain. Dental extractions and root canal therapy was carried out in one or more teeth in 46% of these patients to eliminate a dental cause for their pain.36 These studies clearly illustrate that the TAC syndromes can often mimic and be mistaken for odontogenic or temporomandibular pain disorders, hence the need for dental practitioners to be aware of them to avoid unnecessary and inappropriate dental treatment, and expedite neurologic referral.
Treatment
The excruciating and highly disabling nature of the TAC syndromes warrants immediate and effective treatment. Since the dental practitioner would not be expected to treat patients with the TAC syndromes, a brief overview of the treatment strategies will suffice. Currently there are both medical and surgical interventions available for these patients. Medical management may fall into one of three categories; acute, preventive or transitional therapies. Acute or abortive treatment is given at the onset of an attack and is aimed at aborting the attack itself, whilst the aim of preventive medication is to produce a rapid suppression of attacks and maintain that remission while the patient is still in a bout. However, preventive treatments generally need to be titrated to an optimum dose and therefore there can be a delay of a few days to weeks before their beneficial effect emerges. Transitional treatments are therapies that can be used to suppress the attacks rapidly, but are only effective for a few days to weeks, and can therefore be helpful while waiting for the preventive treatments to work. Surgical treatments are generally avoided until the medical treatments are exhausted and, therefore, have not been described here.
Cluster headache
Acute treatments include inhalation of 100% oxygen via a non rebreather face mask at 7–15 L/min, subcutaneous sumatriptan injection or intranasal triptans (sumatriptan or zolmitriptan). These acute treatments can usually abort an attack within 15–30 minutes. The preventive strategies include use of verapamil, lithium, topiramate and methysergide, amongst others.3,11 The transitional treatment options in cluster headache include greater occipital nerve blocks and a course of corticosteroids.
Paroxysmal hemicrania
By definition, paroxysmal hemicrania is totally responsive to indometacin. A therapeutic dose of indometacin, generally up to 150 mg daily, must be instituted if a diagnosis of paroxysmal hemicrania is suspected. Complete resolution of the headache is prompt, usually occurring within 1–2 days of initiating the effective dose. Patients then need to be maintained on indometacin to suppress the headaches completely. However, some patients may not tolerate indometacin; the treatment options then include cyclooxygenase-2 inhibitors, calcium channel antagonists (verapamil, Flunarizine), topiramate or greater occipital nerve blocks.3,11
SUNCT
In view of its short duration per attack, the use of abortive treatment is not warranted in SUNCT. The syndrome was, until recently, considered to be relatively refractory to medical treatments, including indometacin, sumatriptan, methysergide, verapamil, valproate, lithium, amitryptiline and carbamazepine.8 Open-label studies have recently reported that lamotrigine, topiramate and gabapentin may be promising options.38,39,40 Our experience is that greater occipital nerve blocks can be beneficial in SUNCT.
Conclusion
The TAC syndromes are rare but highly disabling. Patients may seek treatment from their dental practitioners for pain that they consider to be of dental or jaw origin. The dental practitioners may be the first line of healthcare providers consulted for this pain disorder. Hence, it is vital that they are aware of these syndromes, so that any doubt or inkling of suspicion will trigger the necessary neurological referral rather than the instigation of inappropriate and often irreversible dental treatment.