Kemp M, Edwards HLondon: British Dental Association; 2014
Taylor J Stress in dentistry – a study. Dentistry Mag. 2012; 2:(1)
Lange BM, Fung EY, Dunning DG Suicide rate in the dental profession: fact or myth and coping strategies. Dent Hypoth. 2012; 3:164-168
Myers H, Myers L It's difficult being a dentist: stress and health in the general dental practitioner. Br Dent J. 2004; 197:89-93
What's Happening?. Riskwise UK. 2014; 47:5-6
Charles SC, Warnecke RB, Nelson A, Pyskoty CE Appraisal of the event as a factor in coping with malpractice litigation. Behav Med. 1988; 14:(4)148-155
Jones JW, Barge BN, Steffy BD, Fay LM, Kunz LK, Wuebker LJ Stress and medical malpractice: organisational risk assessment and intervention. J Appl Psychol. 1988; 73:(4)727-735
O'Connor JLondon: Element; 2002
Lankton SUSA: Meta Publications; 1980
Kelly GANew York: Norton; 1963
Keller A, Litzelman K, Wisk LE, Maddox T, Cheng ER, Creswell PD, Witt WP Does the perception that stress affects health matter? The association with health and mortality. Hlth Psychol. 2012; 31:(5)677-684
Vernon MDHarmondsworth: Penguin Books; 1962
James T, Woodsmall WUSA: Meta Publications; 1988
Williams JTLondon: Methuen; 2000
Malim TLondon: MacMillan Press; 1997
James T, Flores L, Schober JWales: Crown House Publishing; 2000
O'Connor J, Seymour JLondon: Mandala; 1990
Korzybski AHSNew Jersey: The International Non-Aristotelian Library Publishing Company; 1933
How neurolinguistic psychotherapy (NLPt) could help to improve psychological wellbeing within the dental profession Joanna Taylor Dental Update 2024 43:3, 707-709.
Authors
JoannaTaylor
MHS(Acc), Psychotherapist (NLPt)
Accredited Member of the National Hypnotherapy Society, a Member of NLPtCA (Neurolinguistic Psychotherapy & Counselling Association) and a Member of INLPTA (International NLP Trainers Association)
This article is an exploration of some of the causes of stress within the dental profession and a discussion on how some of the models and philosophies of NLPt could help improve the levels of psychological wellbeing within the profession. Some of the fundamental concepts of NLPt are explored, with particular reference to their application in regard to stress. It is concluded that NLPt could provide a robust methodology for reducing psychological distress within the profession, by helping dentists to understand the concept of unuseful constructs, to improve behavioural choice and to discover the possibility of a more resourceful way of being.
CPD/Clinical Relevance: Dentists under stress do not perform well; judgement is impaired, motivation is reduced and poor decisions can be made which impact directly on patient care.
Article
Psychological wellbeing in the dental profession
A study was undertaken recently by the British Dental Association to assess levels of personal wellbeing among UK Dentists,1 the findings of which indicated that dentists reported lower levels of personal wellbeing when compared with the general UK population. The study found that:
‘All dentists [who responded in the two surveys] indicated lower levels of life satisfaction than adults in the general population; for example, dentists were between two and three times more likely than UK adults to indicate very low levels of life satisfaction.’
Levels of happiness amongst the profession were found to be significantly lower (38% of dentists reporting low levels, compared with 28% of UK adults) and anxiety higher (53% of dentists reporting high or very high levels compared with 39% of UK adults).
Dentistry, like every profession, has its own particular stressors; the comparative isolation of the practitioner, dealing with anxious and stressed patients, conflicts within the practice, missed appointments, running late and, increasingly, the concern over patient complaints and possible litigation are all factors which contribute towards heightened stress and, for some, can lead to more severe anxiety and depression.2
In a study on suicide rate within the dental profession,3 the authors also make the generalization that dentists can often display perfectionistic tendencies. This character facet may well contribute to higher stress levels; for example, if limitations on time factors compromise an individual's ability to perform to the best of his/her ability or, conversely, the desire to achieve perfection results in running behind schedule for the following patients. Work that is undertaken tends to be consistently underrated because the perfectionist dentist will focus on any perceived lack of perfection, so that nothing is ever good enough, even when the patient is manifestly happy with the result.
As Myers & Myers,4 in their 2004 study on stress and health in the general dental practitioner found:
‘Being a professional within healthcare has long been identified as a high-stress occupation due to the combination of difficult working circumstances, exposure to potentially hazardous diseases, human suffering and ability to affect human life.’
Their study findings indicated that work-related stress ‘explained nearly half of the overall stress in a GDP's life.' In their conclusion, they state that, ‘the next step should be to develop interventions to help dentists to reduce stress in the dental surgery.'
Dentists under stress do not perform well; judgement is impaired, motivation is reduced and poor decisions can be made which impact directly on patient care. In the current litigious environment, this can lead to increased levels of patient complaints and, ultimately, the potential for involvement of the General Dental Council.
According to Dental Protection's recently published figures,5 it would seem that regulatory complaints had risen from just over 5,500 in 2000 to around 10,000 in 2012. From January to April 2014, however, the number of cases was already at 17,433. The report states that, ‘too many cases are wrongly assessed, misunderstood and hopelessly ‘overworked’, and through all of this, too many registrants are having experiences that are unnecessarily stressful and tortuous.' Indeed, the experience of coping with malpractice litigation has been described by some as ‘the most stressful event of their entire lives.'6
An article published in the Journal of Applied Psychology in 19887 describes four studies which were undertaken to investigate the link between stress and medical malpractice and the impact of stress management programmes in reducing the risk of malpractice. It was found that high levels of workplace stress led to high levels of malpractice claims. However, the frequency of claims was significantly reduced in those organizations who chose to implement an organization-wide stress management programme.
The all too commonly adopted defence mechanism of ‘appearing strong’ can ultimately create the very issues it was seeking to avoid. The concern for individuals in the profession should no longer be the need to create a false appearance of strength, but instead to accept and own their vulnerabilities in order to build a firm foundation through the creation of genuine strength.
The concept of NLPt
NLPt is an holistic, outcome-focused model, based on constructivist principles and holding at its heart the basic presuppositions of Neuro-Linguistic Programming, as developed by John Grinder and Richard Bandler in the 1970s.19
It has a diverse history and an eclectic combination of therapeutic aspects which gives the NLPt therapist choice and behavioural flexibility when working with clients. For example, aspects of Gestalt, Transactional Analysis, Cognitive Behavioural Therapy, Hypnotherapy, Rogerian Therapy and Jungian Psychotherapy can all be accredited. It maintains the premise that positive change at an unconscious level can enable the individual to have greater behavioural choice.
The principles of constructivism
The philosophy of constructivism rests on the theory that, as man exists in his universe, he gives meaning to his world as perceived via his senses, through the filters of his own thoughts. Because an individual's experience of being in the world is unique, the meanings he infers about the world around him will also be unique. We each have our own memories, our own values and our own beliefs about the way in which the universe works, and we use these to make sense of our reality, as it happens around us. Our sensory information is selectively deleted, distorted and generalized by our filters in order to make it fit our own individual model of the world; we see what we believe, and we believe what we see; if it doesn't fit with our model of reality then we will disregard it, or delete it. We are effectively constructing a reality which is unique to ourselves, through our unconscious mental processes.
Lankton9 writes, ‘What choices clients are able to make in the structuring of their own experience will profoundly affect their entire lives.' As individuals construct their own reality through the way they filter their experience, those constructs may be either empowering or limiting, depending on that individual's filters. If the constructs are currently unuseful, how might they be enabled to create alternative constructs which help them to achieve a greater sense of psychological wellbeing? As Kelly10 states, ‘Because he can represent his environment, he can place alternative constructions upon it and, indeed, do something about it if it doesn't suit him.'
In order to achieve an outcome of facilitating change towards increasing levels of wellbeing within the dental profession, it is necessary to understand the problem by exploring the patterns that are maintaining the current status quo.
The construct of stress
Consider the construct of stress. Stress is a subjective response to a given situation; events in themselves are not stressful, it is the individual's perception of the event which creates their response. A perceived stressful situation can be described as one in which, ‘environmental demands, internal demands, or both, tax or exceed the adaptive resources of an individual, social system or tissue system.'11
An individual's reaction to stress (ie his/her behaviour and physiology) depends upon the perception of the stressor. Perception of an event varies according to an individual's previous experience; ie his/her cognition of the stressor based on an understanding of the situation, as perceived through the senses and the internal filters of memory, values and beliefs. His or her perception will also depend on the individual's current affective state at the time12,13 and by fundamental aspects and tendencies of personality, known as Meta-Programmes,12,13 which are based on the work of Carl Jung; for example, whether an individual considers him/herself to be introverted or extroverted.
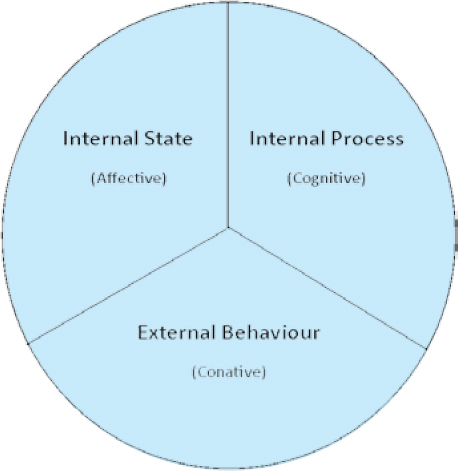
In NLPt, this is reflected in the NLP Model for Change12,13 (Figure 1).
Figure 1. The NLP Model for Change.
When an individual creates congruent change, all three areas of this system are affected. A change in the way an individual is constructing the current model of the world (internal process) will affect the individual's internal state, and therefore his/her external behaviour.
For example, dentists with work-related stress feel anxiety (internal state) at the prospect of going in to the surgery (external behaviour). They are running internal thought processes which involve highly negative representations of their work day and will be displaying external behaviour congruent with feelings of anxiety and stress, such as irritability or social withdrawal.
According to Festinger's Theory of Cognitive Dissonance and Heider's Balance Theory, an individual will feel dissonant (ie stressed) if there is inconsistency or incongruity between contextual cognitions, or with perceived facts.14,15 Therefore, if the individual makes a congruent change in his/her cognitive constructs around work (for example, changing a negative or limiting belief), then the same pattern can no longer run. The internal thought processes no longer induce the negative affective state and this will be reflected in a change in external behaviour. This is also evidenced by Milton Erickson's theories of conscious-unconscious integration.16
Individuals, therefore, create different realities for themselves even when faced with the same situations; their happiness, or their stress, is a construct. What might be considered a stressful practising environment by one individual may actually be somewhere another individual might thrive. The models of NLPt allow us to explore the unconscious processes behind the creation of the individual's reality. What is present, or absent, for example, in the psyche of those individuals who create a useful reality for themselves, and how might this knowledge be helpful to those who are creating a reality that is less than useful? For individuals, understanding what is behind their construct; ie the ‘why’ behind their feelings and responses, can be a liberating experience, creating greater behavioural choice and leading to a pro-active rather than reactive response.
The systemic approach
As can be inferred from Figure 1, NLPt is a systemic philosophy; any change in one aspect of an individual will be reflected throughout the whole system. Any problem which is being experienced by an individual will also be reflected throughout the whole of the system, ie the individual's environment or lifespace. This theory was developed by Gregory Bateson and is based on Jungian concepts of wholeness and connectedness.17
It is therefore necessary to consider the problem as a pattern being run by individuals, within the context of the whole system of their lives. The concept of pattern detection is a key element within the therapeutic framework of NLPt, in order to enable the individual to gain a conscious understanding of something which was previously unconscious.
Problems as a linguistic construct
The theory that problems exist in our neurology as a linguistic construct is at the heart of NLPt. In the same way that our internal representations of the reality that exists around us are not the same as that reality, the language we use to describe our experience of reality also differs from that actual experience.9 For example, as we name or identify an object, this can impact on our present and future perception of the object.12 As it becomes associated with our own constructs, it becomes a projective identification rather than a purely objective one; the word is not the item it represents. This is the basis of the NLP presupposition that ‘the map is not the territory’, which originates from Alfred Korzybski's principles of General Semantics, as described in his 1933 work, Science and Sanity.18
Use of a specific word can therefore create a sensory experience for an individual, who has connected the word with an experience from the past. However, the sensory experience is not precisely the same as the original reality, and the language the individual uses to describe the sensory experience is not the same as the sensory experience.17 As we take in information from the original reality it is deleted, distorted and generalized in order for us to give it meaning, and we must, of necessity, then delete, distort and generalize any experience once again in order to describe it linguistically. An individual's linguistic description of a problem is therefore, as it were, two removes from the original reality.
Stressed dentists could be stressed because of the internal representations they are running regarding a future event, which is a construct based on their experience of something that happened in the past (which is in itself a construct). For example, an associate might be afraid to approach his/her principal with a request, not because the principal is unpleasant or unapproachable, but because of an unconscious belief which the dentist is running with regard to authority, self-esteem or an aversion to conflict. In order to assist the dentist, it is necessary to make sense of the dentist's experience, as perceived by him/her, and one of the keys to this lies in the art of linguistic analysis.
The NLP Meta-Model was developed by the founders of NLP19 and was derived from Noam Chomsky's theories of Transformational Grammar and Alfred Korzybski's principles of General Semantics. It comprises a ‘specific set of linguistic tools and categories that rests upon the premise that words only have meaning insofar as they are associated with internal representations or sensory experience.’9 The Meta-Model questions are a method of recovering unuseful deletions, distortions and generalizations through analysis of the ‘surface structure’ of an individual's linguistics, in order to reconnect with his/her ‘deep structure’ of fundamental experience.
When working with stressed dentists, it is possible to use this model to discover what, specifically, is causing them to feel stressed and begin to uncover some of the constructs they are running; the unconscious double binds and unuseful complex equivalences which are creating their stressful reality.
Sometimes, all that is required is for individuals to have an experience of perceiving their problems from a different perspective. A dentist who presented with stress and anxiety due to conflict with a colleague within her practice was able to make significant positive changes just through gaining understanding of her colleague's values being different from her own. Her realization was that she was judging his behaviours based on her own values, and thereby inferring a complex equivalence that was neither true, nor useful; ‘He is doing this, and that means I'm not a good dentist.' Understanding that there could be other possibilities and intentions behind someone's behaviour created a more liberating construct for her in this, and other, relationships.
Applications of NLPt within the dental profession
NLPt could potentially be a valuable model to help reduce incidence of burnout and psychological distress within the dental profession. As has been noted, stress is created through an individual's own constructs and there is therefore potential to assist dentists in making positive changes in this area in order to transform their way of perceiving the world and provide them with greater behavioural choice.
Perfectionism, as has been noted, is a tendency often displayed within the profession; which is not surprising, given that students applying to study dentistry are selected for high academic achievement. Whilst excellence is achievable, perfection is not – changing this construct can therefore create liberation from the stress of the unattainable goal. Through the medium of NLPt, it is possible to elicit the unuseful constructs which lie behind individuals' needs for perfection and assist them in making whatever changes are desired.
Depression, low self-esteem and feelings of isolation are all contributory factors in the high levels of burnout and, again, are issues which can be helped through NLPt. In a recent research project undertaken as part of the author's postgraduate study,20 it was noted that:
‘There was a general consensus between each of the interviewees that members of the dental profession have a tendency to not call for help until it is too late; there is a perceived need to appear “strong” and a fear of any request for help resulting in a fitness to practice enquiry. All of the interviewees who had received professional help to recover from breakdown cited the need within the profession for a safe, confidential, non-judgemental environment where they could discuss their issues without putting their career at risk.’
If NLPt was widely available and perceived as a useful means of support within the profession, provided within a ‘safe, confidential and non-judgemental environment’, it is possible that the stigma attached to seeking help could be reduced.
In addition, if some of the models and philosophies of NLP were to be adopted within the profession and within practices as a whole, it is possible that much of the stress induced by poor communication and staff conflict could be reduced. Tools, such as the Milton Model,8 for example, are very valuable when dealing with anxious patients; another source of stress.2
When individuals within the profession are able to challenge the fundamental negative constructs which lie at the heart of their problems, this will impact not only on their own lives, but also on the lives of those around them.
Conclusion
As various studies have proven, levels of stress are high and widespread within the dental profession as a whole. As individuals, each will have their own unique constructs and models of the world which create their ability to cope well with potentially stressful situations – or not. Whilst there is an overall pattern of stress, when viewed holistically it cannot be said that there is any one specific cause, other than the constructs of the individuals within the system who are creating for themselves a reality that is stressful – or not.
As a constructivist approach, therefore, it could be postulated that NLPt might provide a robust methodology for reducing the incidence of psychological distress within the profession and, if dental professionals can be encouraged to seek help, to increase the overall levels of wellbeing and mental health through the development of self-awareness and increased behavioural choice.
This would be of immeasurable benefit not only to the profession as a whole, but to their families, colleagues and patients; the latter of whom would enjoy increased levels of care, which would in turn result in reduced incidence of patient complaints – in itself a major source of stress in the current climate.