Reissmann D Functional and psychosocial impact related to specific temporomandibular disorder diagnoses. J Dentistry. 2007; 35:(8)643-650
Durham J ‘Management is a black art’ – professional ideologies with respect to temporomandibular disorders. Br Dent J. 2007; 202:(11)
Dworkin SF Epidemiology of signs and symptoms in temporomandibular disorders: clinical signs in cases and controls. J Am Dent Assoc. 1990; 120:(3)273-281
Slade GD Study methods, recruitment, sociodemographic findings, and demographic representativeness in the OPPERA study. J Pain. 2011; 12:T12-26
Gray RJ, Davies SJ, Quayle AA A clinical approach to temporomandibular disorders. 1. Classification and functional anatomy. [Erratum appears in Br Dent J 1994; 177(2): 68]. Br Dent J. 1994; 176:(11)429-435
Al-Ani Z, Gray R TMD current concepts: 1. An update. Dent Update. 2007; 34:(5)278-280
Turp JC, Schindler H The dental occlusion as a suspected cause for TMDs: epidemiological and etiological considerations. J Oral Rehabil. 2012; 39:(7)502-512
Suvinen TI Review of aetiological concepts of temporomandibular pain disorders: towards a biopsychosocial model for integration of physical disorder factors with psychological and psychosocial illness impact factors. Eur J Pain. 2005; 9:(6)613-633
McNeill C Management of temporomandibular disorders: concepts and controversies. J Prosthet Dent. 1997; 77:(5)510-522
Okeson JP, 6th edn. St Louis: Mosby; 2008
McNeill C Temporomandibular disorders: diagnosis, management, education, and research. J Am Dent Assoc. 1990; 120:(3)
Ohrbach R Clinical findings and pain symptoms as potential risk factors for chronic TMD: descriptive data and empirically identified domains from the OPPERA case-control study. J Pain. 2011; 12:T27-45
Naeije M Disc displacement within the human temporomandibular joint: a systematic review of a ‘noisy annoyance’. J Oral Rehabil. 2013; 40:(2)139-158
Greene CS, Laskin DM Long-term status of TMJ clicking in patients with myofascial pain and dysfunction. J Am Dent Assoc. 1988; 117:(3)461-465
Ohrbach R Disability assessment in temporomandibular disorders and masticatory system rehabilitation. J Oral Rehabil. 2010; 37:(6)452-480
Brown RS, Johnson CD, Fay RM The misdiagnosis of temporomandibular disorders in lateral pharyngeal space infections – two case reports. Cranio. 1994; 12:(3)194-198
Reiter S Nasopharyngeal carcinoma mimicking a temporomandibular disorder: a case report. J Orofacial Pain. 2006; 20:(1)74-81
Wright EF, Gullickson DC Identifying acute pulpalgia as a factor in TMD pain. J Am Dent Assoc. 1996; 127:(6)773-780
Manfredini D Dental occlusion, body posture and temporomandibular disorders: where we are now and where we are heading for. J Oral Rehabil. 2012; 39:(6)463-471
Helkimo M Studies on function and dysfunction of the masticatory system. 3. Analyses of anamnestic and clinical recordings of dysfunction with the aid of indices. Svensk Tandlakaretidskrift. 1974; 67:(3)165-181
Helkimo M Studies on function and dysfunction of the masticatory system. I. An epidemiological investigation of symptoms of dysfunction in Lapps in the north of Finland. Proc Finnish Dent Soc. 1974; 70:(2)37-49
Helkimo M Studies on function and dysfunction of the masticatory system. II. Index for anamnestic and clinical dysfunction and occlusal state. Svensk Tandlakaretidskrift. 1974; 67:(2)101-121
Levitt SR, McKinney MW, Lundeen TF The TMJ scale: cross-validation and reliability studies. Cranio. 1988; 6:(1)17-25
Fricton JR, Schiffman EL Reliability of a craniomandibular index. J Dent Res. 1986; 65:(11)1359-1364
Dworkin SF Research diagnostic criteria for temporomandibular disorders: current status and future relevance. J Oral Rehabil. 2010; 37:(10)734-743
Dworkin SF, LeResche L Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992; 6:(4)301-355
Hasanain F Adapting the diagnostic definitions of the RDC/TMD to routine clinical practice: a feasibility study. J Dentistry. 2009; 37:(12)955-962
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Groupdagger. J Oral Facial Pain Headache. 2014; 28:(1)6-27
Crow HC The utility of panoramic radiography in temporomandibular joint assessment. Dento-Maxillo-Facial Radiol. 2005; 34:(2)91-95
Petersson A What you can and cannot see in TMJ imaging – an overview related to the RDC/TMD diagnostic system. J Oral Rehabil. 2010; 37:(10)771-778
Limchaichana N, Petersson A, Rohlin M The efficacy of magnetic resonance imaging in the diagnosis of degenerative and inflammatory temporomandibular joint disorders: a systematic literature review. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2006; 102:(4)521-536
AADR. (Accessed March 21, 2012)
Greene CS Managing the care of patients with temporomandibular disorders: a new guideline for care. J Am Dent Assoc. 2010; 141:(9)1086-1088
Wright EF Pulpalgia contributing to temporomandibular disorder-like pain: a literature review and case report. J Am Dent Assoc. 2008; 139:(4)436-440
Turner JA, Holtzman S, Mancl L Mediators, moderators, and predictors of therapeutic change in cognitive-behavioral therapy for chronic pain. Pain. 2007; 127:(3)276-286
Aggarwal VR Reviewing the evidence: can cognitive behavioral therapy improve outcomes for patients with chronic orofacial pain?. J Orofacial Pain. 2010; 24:(2)163-171
Gray RJ Physiotherapy in the treatment of temporomandibular joint disorders: a comparative study of four treatment methods. Br Dent J. 1994; 176:(7)257-261
Feine JS, Lund JP An assessment of the efficacy of physical therapy and physical modalities for the control of chronic musculoskeletal pain. Pain. 1997; 71:(1)5-23
Michelotti A Home-exercise regimes for the management of non-specific temporomandibular disorders. J Oral Rehabil. 2005; 32:(11)779-785
Al-Ani Z Stabilization splint therapy for the treatment of temporomandibular myofascial pain: a systematic review. J Dent Educ. 2005; 69:(11)1242-1250
Conti PCR The treatment of painful temporomandibular joint clicking with oral splints: a randomized clinical trial. J Am Dent Assoc. 2006; 137:(8)1108-1114
Wassell RW, Adams N, Kelly PJ Treatment of temporomandibular disorders by stabilising splints in general dental practice: results after initial treatment. Br Dent J. 2004; 197:(1)35-41
Wassell RW, Adams N, Kelly PJ The treatment of temporomandibular disorders with stabilizing splints in general dental practice: one-year follow-up. J Am Dent Assoc. 2006; 137:(8)1089-1098
Moufti MA, Lilico JT, Wassell RW How to make a well-fitting stabilization splint. Dent Update. 2007; 34:(7)398-400
The glossary of prosthodontic terms. J Prosthet Dent. 2005; 94:(1)10-92
Truelove E The efficacy of traditional, low-cost and nonsplint therapies for temporomandibular disorder: a randomized controlled trial. J Am Dent Assoc. 2006; 137:(8)1099-1107
Davies SJ, Gray RJ The pattern of splint usage in the management of two common temporomandibular disorders. Part II: The stabilisation splint in the treatment of pain dysfunction syndrome. Br Dent J. 1997; 183:(7)247-251
Fricton J Systematic review and meta-analysis of randomized controlled trials evaluating intraoral orthopedic appliances for temporomandibular disorders. J Orofacial Pain. 2010; 24:(3)237-254
Saha S, Summerwill AJ Reviewing the concept of Dahl. Dent Update. 2004; 31:(8)442-447
Stapelmann H, Turp JC The NTI-tss device for the therapy of bruxism, temporomandibular disorders and headache – where do we stand? A qualitative systematic review of the literature. BMC Oral Health. 2008; 8:1-23
Schiffman EL Randomized effectiveness study of four therapeutic strategies for TMJ closed lock. J Dent Res. 2007; 86:(1)58-63
Mujakperuo HR Pharmacological interventions for pain in patients with temporomandibular disorders. Cochrane Database of Syst Revs. 2010; (10)
Cairns BE Pathophysiology of TMD pain - basic mechanisms and their implications for pharmacotherapy. J Oral Rehabil. 2010; 37:(6)391-410
List T, Axelsson S Management of TMD: evidence from systematic reviews and meta-analyses. J Oral Rehabil. 2010; 37:(6)430-451
Luther F, Layton S, McDonald F Orthodontics for treating temporomandibular joint (TMJ) disorders. Cochrane Database Syst Revs. 2010; (7)
Appelgren A Neuropeptides in the arthritic TMJ and symptoms and signs from the stomatognathic system with special consideration to rheumatoid arthritis. J Orofacial Pain. 1995; 9:(3)215-225
Cady RJ, Hirst JJ, Durham PL Dietary grape seed polyphenols repress neuron and glia activation in trigeminal ganglion and trigeminal nucleus caudalis. Mol Pain. 2010; 6
Slade GD Cytokine biomarkers and chronic pain: association of genes, transcription, and circulating proteins with temporomandibular disorders and widespread palpation tenderness. Pain. 2011; 152:(12)2802-2812
Moayedi M Contribution of chronic pain and neuroticism to abnormal forebrain gray matter in patients with temporomandibular disorder. Neuroimage. 2011; 55:(1)277-286
Lotze M The cerebral representation of temporomandibular joint occlusion and its alternation by occlusal splints. Hum Brain Mapp. 2012; 33:(12)2984-2993
Meloto CB Genomics and the new perspectives for temporomandibular disorders. Arch Oral Biol. 2011; 56:(11)1181-1191
Aneiros-Guerrero A Genetic polymorphisms in folate pathway enzymes, DRD4 and GSTM1 are related to temporomandibular disorder. BMC Med Genet. 2011; 12
Planello AC Association of matrix metalloproteinase gene polymorphism with temporomandibular joint degeneration. Eur J Oral Sci. 2011; 119:(1)1-6
Schwahn C The effect of catechol-O-methyltransferase polymorphisms on pain is modified by depressive symptoms. Eur J Pain. 2012; 16:(6)878-889
Gatchel RJ Major psychological disorders in acute and chronic TMD: an initial examination. J Am Dent Assoc. 1996; 127:(9)1365-1374
Pain part 6: temporomandibular disorders Pamela L Yule Justin Durham Robert W Wassell Dental Update 2024 43:1, 707-709.
Authors
Pamela LYule
BDS, MFDS RCPS(Glasg)
Specialty Registrar and Associate Clinical Lecturer in Restorative Dentistry, Newcastle Dental Hospital, Richardson Road, Newcastle upon Tyne, NE2 4AZ, UK
Senior Lecturer and Honorary Consultant in Restorative Dentistry, School of Dental Sciences, Newcastle University, Framlington Place, Newcastle upon Tyne, Tyne and Wear NE2 4BW, UK
TMDs are a complex collection of conditions which can have a significant impact on an individual's quality of life. The aetiology, diagnosis and management of TMDs will be described in this article with the hope of increasing a general dental practitioner's knowledge of these problems, thus helping them to institute simple, initial, conservative therapies for such patients. Diagnosis of TMDs can be simplified by following recent published clinical diagnostic criteria such as those outlined in this article.
CPD/Clinical Relevance: Pain and functional disturbances related to TMDs are common and require simple and pragmatic interventions for most patients. After providing a diagnosis, reassure patients that they do not have a sinister disease, and explain that the condition is usually self-limiting.
Article
Temporomandibular disorders (TMDs) are a complex range of conditions which can cause significant pain and distress for individuals affected,1 and can leave some dentists bewildered into how best to manage such patients.2 The main part of this article describes current best evidence on the epidemiology, aetiology, signs, symptoms and diagnosis, and management of TMDs. The final section gives a flavour of important ongoing research into the mechanisms underlying TMDs.
Epidemiology
The reported prevalence of TMDs in both the general and clinical population varies, and this may be due to differences between studies in diagnostic criteria and their assessment of TMDs.3 Recent research in a group of patients aged 18–44 years suffering from TMDs showed that the likelihood of having TMD increased across successively older age groups.4 In the same clinical group, non-Hispanic Whites were more likely to have TMDs compared to other racial groups, and females were three times more likely than males to suffer TMD symptoms.4 However, in the general population it is worth noting that signs and symptoms of TMD are quite common and found almost equally in males and females.5 Research suggests that only a small proportion of individuals with TMDs actually seek treatment3 and that females are more likely to present to a healthcare professional in an attempt to alleviate their symptoms.3,5
Aetiology
The aetiology of TMDs is poorly understood6,7 although, as we will see at the end of this article, there are major steps being taken to improve this situation. It is worth emphasizing that, for most patients, there is little to support the popular notion that TMDs are caused by the occlusion.8 Clinically, it is therefore best to regard the aetiology as multifactorial and biopsychosocial,9 with predisposing, precipitating and prolonging factors all playing a part.10 Predisposing factors include structural, metabolic, or psychological conditions, which may cause an increased risk of developing TMDs by adversely affecting the masticatory complex. Precipitating factors include trauma, either as a result of direct injury to the head and neck region, or due to repetitive loading through parafunction. Prolonging factors include psychosocial problems, which may perpetuate an existing TMD problem. Exact cause and effect relationships have been difficult to establish, particularly because it is difficult to establish controls for all variables.11 A variety of pathophysiological influences may help to explain why some patients appear more susceptible to developing TMDs than others. These are considered at the end of the article.
Signs, symptoms and diagnosis
The most common initial symptom in TMDs is pain, usually in/around the temporomandibular joint (TMJ), or in the muscles of mastication, or both.12,13 For other symptoms see Key Facts Box 1. In the general population, joint noise, such as clicking, is very common (18–30%14) and, in the absence of pain, is usually of little clinical significance unless it is embarrassingly loud.15 Like other musculoskeletal disorders, patients with TMDs can show a range of difficulties in function, eg difficulty opening, closing, chewing and talking, which can be intermittent or constant and can range from mild to severe.16 It is important to remember that common dental problems (eg caries, periodontal or periapical infections), systemic disease, or neoplasia, although rare, can result in signs and symptoms that mimic those of TMDs.17,18 Pulpitic complaints may also exacerbate the symptoms of TMDs and therefore should be appropriately and promptly managed.19
Signs and symptoms of TMDs are clinically variable and often idiosyncratic but they include six broad groups:
Muscular tenderness – in face (masseter, temporalis, posterior diagastric, mylohyoid), mouth (medial or lateral pterygoid), neck and shoulders (but remember that cervical problems can occur independently of TMDs)
Pain – in head, neck and shoulders
Joint noises – clicking, crepitus (grinding)
Locking – open (dislocation) or closed (inability to open fully)
TMD sufferers have a higher chance of suffering a variety of co-morbidities including headache, lower back pain, irritable bowel syndrome and other chronic pain outside the orofacial region.13 Signs and symptoms of TMDs can also present as part of a spectrum of another condition: for example fibromyalgia, systemic joint laxity (eg Ehlers Danlos syndrome) or arthritis20 (Key Facts Box 2). It is obviously important not only to make a diagnosis of TMDs in such instances but also to liaise with the patient's medical practitioner for further investigation and/or appropriate management if other disorders are suspected.
Other pathologies that can affect the temporomandibular joint complex include:
Hypermobility (eg recurrent dislocation) or hypomobility
Growth disturbances (eg condylar hypoplasia)
Ankylosis
The diagnosis of TMDs in a clinical practice setting mainly depends on completing, and interpreting, a thorough history and clinical examination. Although there are a number of specialist diagnostic tests, eg jaw tracking and vibratography, these have poor sensitivity and specificity. They therefore risk labelling the patient with an incorrect diagnosis21 and prescribing an inappropriate treatment. Imaging techniques can occasionally be helpful but have their limitations, as described in a later section.
In large-scale epidemiological research, short indices have been created and used to screen populations for signs and symptoms of TMDs,22,23,24,25,26 but they are not particularly specific for the sub-classification of the type of TMDs.
The Research Diagnostic Criteria for TMDs (RDC/TMD) was developed in 1992, and is currently being updated.27 Its primary purpose was to facilitate research into TMDs based on well-defined homogeneous sub-groups that could be identified reliably using operationalized criteria. It has shown fair to good reliability and is the most widely used diagnostic system for research into TMDs.27 It provides a rigorous assessment of the patient's problem, other than simple clinical examination, to allow sample selection for research.
The RDC/TMD index has a dual axis approach with Axis 1 concentrating on the clinical examination and Axis 2 assessing the psychosocial aspect of TMDs. Axis 1 follows a standardized protocol for clinical examination and can result in multiple diagnoses being given according to three main groups of common conditions (Table 1). Axis 2 of the RDC/TMD comprises a self-administered questionnaire, giving further information on the patient's complaint and the disability, depression and non-specific pain associated with it. A new shorter version of the RDC/TMD has been developed: the DC/TMD.30 Sadly the new DC/TMD is not any more succinct than the RDC/TMD and so is likely to remain a research instrument. In time, the DC/TMD may be further refined into a shorter protocol more suited to everyday clinical needs.
Main Grouping
Sub-Group
Key Findings from Clinical Exam and History to Support Diagnosis
*To determine if pain provoked during examination is the pain from which the patient is suffering ask, ‘Is this your familiar pain?’.
Clinical assessment
Whilst we await development of a shorter DC/TMD it is worth noting the existence of the Clinical Examination Protocol (CEP-TMD). This has been shown to produce diagnoses as reliable as Axis 1 of the RDC/TMD and is much quicker to complete, making it more suitable for the routine clinical practice setting.29 In a relatively short time dentists can learn to make reliable TMD diagnoses according to the key findings from the clinical examination (Table 1).
A video showing how to carry out the examination plus the accompanying clinical forms, which help with history-taking, examination, diagnosis and follow-up, can be found at www.ncl.ac.uk/dental/AppliedOcclusion/
Although this system does not provide a formal Axis 2 diagnosis, it does ask the patient questions that provide a helpful insight into this important aspect of the condition. Importantly, patients can complete the history questionnaire in the waiting room, which saves time during the appointment. It is important to note if patients have had multiple previous treatments, particularly if they have been unsuccessful. These patients are not well suited to management exclusively in general dental practice. It is also worth remembering that a proportion of TMD patients will have symptoms of persistent orofacial or dento-alveolar pain, which again are not easily managed exclusively in primary care.
Imaging
Imaging in the form of plain radiographs can have a role, for example, in excluding TMJ pathology with osseous changes (eg rheumatoid arthritis). Its use for diagnosis of TMDs is, however, otherwise limited,31 as many TMDs involve the soft tissues. Moreover, when osseous condylar changes are seen radiographically they often fail to correlate with the level of clinical symptoms, which may result in false positives being recorded.31 Computed and cone-beam tomography unsurprisingly demonstrate an excellent ability to detect osseous changes. Nevertheless, the question remains after these ionizing investigations whether or not any demonstrated changes are symptomatic, which can only be identified through history-taking and clinical examination.32
Magnetic resonance imaging (MRI) is principally used to determine the position of the articular disc or explain the existence of a soft tissue swelling (eg a joint effusion). Despite being the ‘gold standard’ for imaging of the soft tissues of the TMJ,33 it too suffers from false positives, especially in relation to disc position and configuration.34 This may change, however, with further advancements in this form of imaging.
It is clear that diagnosis of TMDs is currently best made after careful history-taking and clinical examination, preferably with a standardized approach as used with the RDC/TMD or the CEP-TMD. Imaging should currently be considered as an adjunct to clinical diagnosis and is indicated only in a minority of presenting cases as there is currently no clear evidence as to when TMJ imaging is beneficial.32 In secondary care, imaging may be indicated where conservative management has failed (eg for a disc displacement without reduction) and a comprehensive diagnostic work-up is needed, particularly in the rare cases when surgery may be considered.
Management
Good quality, clear evidence for the management of TMDs is lacking, largely due to heterogeneity of both the methodology and the outcome measures used in trials.11 This has led the American Association for Dental Research to re-issue its policy statement on the management of TMDs, which states that initial treatment of TMDs should focus on conservative, reversible treatment.35 The rationale for this is that conservative, reversible therapies have been shown to be at least as effective as more invasive treatments in producing symptomatic relief but with less potential for harm.35,36
Thorough examination, investigation and diagnosis of patients prior to commencing a TMD management strategy is essential to ensure: first, that the presenting complaint is TMD and not another condition mimicking it; and secondly, that there are no other contributing factors such as acute dental pain19,37 or other co-morbidities.
After exclusion of rare sinister/serious causes of pre-auricular pain (Key Facts Box 3 for red flags for sinister/serious disease), it is imperative for the clinician to reassure patients that they do not have a sinister cause for their pain and that in many cases TMDs are self-limiting.
Red flags for serious pathology causing orofacial pain requiring urgent referral:
History of cancer (may suggest metastasis)
Pain that is abrupt in onset, severe, or precipitated by exertion, coughing, or sneezing, or that interrupts sleep (may suggest intracranial pathology)
Neurological symptoms or signs (may suggest a tumour or other intracranial pathology)
Swelling of the TMJ, mandible, or parotid gland (may suggest tumour, infection, or inflammatory arthropathy)
Facial asymmetry (may indicate a tumour)
Unilateral headache or scalp tenderness, jaw claudication, or visual symptoms (suggests giant cell arteritis)
Nasal symptoms – persistent loss of smell (anosmia), purulent discharge, nasal blockage or epistaxis (may suggest a nasopharyngeal tumour)
Neck mass or persistent cervical lymphadenopathy (may suggest infection or tumour)
Change in occlusion. This may suggest a tumour or bone growth (for example in acromegaly) around the TMJ or inflammatory arthritis; but can also be seen in other TMDs
Decreased hearing on the ipsilateral side (may suggest a nasopharyngeal tumour or acoustic neuroma)
Increasing pain or limitation in function despite initial management (may suggest a tumour)
We clinicians often forget that, when patients have pain of spontaneous onset and of unknown aetiology, they may be very distressed, particularly after consulting the internet. Patients may have been referred from primary care without explanation and may well assume that their unexplained pre-auricular pain must be related to a serious problem as they have been referred to secondary care.
Conservative therapy for management of TMDs including pharmacological treatment
Conservative therapy includes cognitive behavioural therapy, physiotherapy, the use of intra-oral splints and pharmacological therapy.
It has been suggested that all TMD patients may benefit from cognitive behavioural therapy (CBT).38 This may begin in an extremely simple form with the dentist reassuring the patient and providing an explanation of the problem and its aetiology, along with a management strategy. A recent review of studies of CBT used in the treatment of patients with TMDs in secondary care showed it could improve outcomes.39 However, the best mode of delivery and its cost-effectiveness still needed to be determined.39
In many musculoskeletal disorders, physiotherapy started early in the course of the condition may help to reduce symptoms. Completing an exercise programme is beneficial in patients with TMDs whose problems are largely myofascial in aetiology.40,41 Home-exercise programmes (in conjunction with CBT) have been described which general dental practitioners can tailor to their patients' needs, depending on the TMD diagnosis42 (Table 2).
Self-Management Procedure
What This Involves
1. Counselling and Patient Education
- reassure patient
- explain aetiology, prognosis of problem
- habit reversal techniques
- encourage proper use of jaw
2. Thermotherapy
- moist heat pads or cold pads applied to painful muscles
3. Auto-massage
- massaging the muscles of mastication
4. Stretching Exercises
- use of the fingers or tongue depressors to increase opening, performed several times daily
5. Co-ordination Exercises
- opening and closing the mouth slowly 20 times with index finger on lateral poles of TMJs to control mandibular movement, performed several times daily
6. Mobilization Exercises
- series of lateral excursive and protrusive movements performed daily to try and re-capture the disc in patients with disc displacements
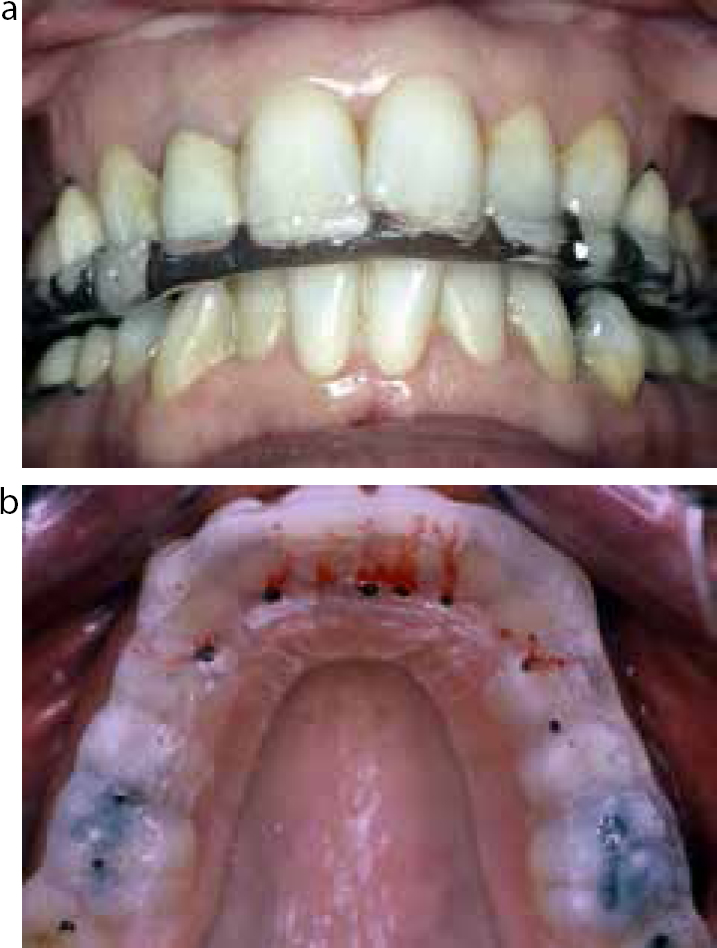
Intra-oral splint therapy can also reduce TMD symptoms43,44 and can work effectively in general dental practice.45,46 The two most commonly used splints in the management of TMDs are: soft splints or stabilization splints. Soft splints are usually made of flexible polyvinyl of 2 mm thickness and are full coverage splints.47 Stabilization splints (also known as Michigan or Tanner appliances, depending on whether they are fitted to the upper or lower teeth) are also full coverage splints, most commonly made of hard acrylic.48 Stabilization splints involve creating ‘occlusal stability’ by producing even contacts throughout the arch on closing in ‘centric relation’, and canine or anterior guidance in lateral excursions, with removal of all interferences48 (Figure 1). It should be remembered that centric relation is defined as a position of health and cannot be recorded in many TMD patients.49 Therefore, stabilization splints often require multiple adjustments to achieve stability.
Figure 1. An upper stabilization splint viewed (a) anteriorly and (b) palatally showing even occlusal contact (marked in black), canine and incisal guidance (marked in red). Patients with adequate posterior support often find it more comfortable to have slightly lighter incisor contacts against the splint.48
There is some evidence to suggest that, for the majority of patients, stabilization splints offer no additional benefit over soft splints,50 or splints with no occlusal surface,45 in reducing TMD signs or symptoms. In routine cases it would therefore seem sensible to construct a simple, less expensive soft splint in the first instance to see how the patient responds. We review such treatment after three months. Approximately 10–15% of our TMD patients are provided with stabilization splints (based on our splint production numbers).
Generally, we recommend patients wear splints only for sleeping,51 although a few patients with occlusal instability wear their stabilization splint full-time with frequent adjustment needed by the dentist, usually on a two-week basis, until a stable occlusion has been created on the splint. Fricton et al, in a meta-analysis of splint studies, have emphasized the importance of accurate splint adjustment in securing any advantage of using this type of appliance.52 To avoid patients becoming over-reliant on the splint they should be encouraged to wean themselves off daily use within six months. In those few patients who need to persist with daily or full-time wear it is important that the splint is kept under close review.
We advise caution in the use of partial coverage splints as unwanted occlusal changes may occur, particularly with prolonged wear when the splint may act as a Dahl appliance.53 A similar consideration applies to anterior repositioning splints which are sometimes used to treat symptomatic TMJ clicking.52 With prolonged wear these appliances can cause posterior open bites in some patients.
Where dentists choose to prescribe partial coverage splints they need to ensure that patients are carefully followed up.54 However, the NTI TSS splint can sometimes be useful for short-term use in patients with acute muscle symptoms, where it would otherwise be difficult to record an impression for a full coverage splint because of limited mouth opening. In such situations, it is important that the dentist makes a correct diagnosis – limited opening caused by a disc displacement without reduction is unlikely to be helped by such an approach. Where a disc displacement without reduction is diagnosed or suspected, dentists are advised to seek early help in management, unless they have training in manipulating the mandible to release the displaced disc. However, with many patients the disc remains displaced forwards or forwards and medially but, over time, opening improves and discomfort decreases in response to exercises and other conservative measures.55 Only very occasionally is surgery needed, usually in the least invasive manner of arthrocentesis or arthroscopy.
In cases where a TMD patient fails to respond sufficiently to conservative treatment, or during episodes of acute pain, medication prescribed in conjunction with the patient's general medical practitioner can be a useful adjunct in management. Many different classes of medication have been used to target the pain caused in differing TMDs, including:
Non-steroidal anti-inflammatory drugs;
Tricyclic antidepressants;
Anxiolytics;
Anti-epileptic drugs; and
Corticosteroids.
The evidence base for the effectiveness of the varied potential pharmacological interventions for pain caused by TMDs is limited and continued research in this field is required.56.57 A reasonable approach to managing TMDs at the initial point of contact may be:
To advise on jaw exercises to be completed twice daily;
To provide a soft splint (but tell the patient to stop using it if, after a couple of weeks of acclimatization, the symptoms worsen);
To advise the use of simple over-the-counter analgesia for a short period of time (subject to no contra-indications to the analgesic's usage).
Patients suffering from TMDs should always be reviewed and followed up carefully once treatment is instituted to ensure that progress is as would be expected.
Irreversible therapy for TMD management
The main types of irreversible therapy which have in the past been proposed are occlusal adjustment and surgical intervention.
There is no evidence that occlusal adjustment is more or less effective than a placebo in treating TMD problems and, as it is irreversible, it is not indicated as a first line treatment.58 In certain circumstances though, it may seem sensible to undertake an occlusal adjustment, for example if the patient's TMD pain began after placement of a restoration and this restoration is shown to be causing an occlusal interference.7 On rare occasions, occlusal adjustment may be required to establish occlusal stability and comfort following stabilization splint treatment. Occlusal equilibration, which can involve sometimes extensive adjustment of multiple teeth, needs to be approached with particular caution as a partial equilibration can result in worsening of a patient's symptoms. Dentists undertaking such work need to be suitably trained and skilled in this procedure.
Surgical treatment of TMDs include procedures such as arthrocentesis, arthroscopy, open joint procedures and joint replacement. The current evidence for using these procedures in TMD patients is poor.58
Historically, orthodontic treatment was thought to cause TMDs in some patients. Orthodontic treatment has also been used in TMD management, based on the outmoded belief that malocclusions cause TMDs. A recent systematic review has refuted that there is any evidence base for either of these assumptions.59
Research into mechanisms underlying TMDs
Recently published and ongoing research has improved our understanding of some of the underlying mechanisms involved in the aetiology of TMDs. These include the following:
Traumatic aetiology of TMDs;
Free radical damage of the TMJ;
Peripheral and central sensitization;
TMDs and genetic polymorphisms;
Cortical changes in TMDs and during splint wear.
Traumatic aetiology of TMDs
Evidence in the form of high ‘odds ratios’ is now emerging that TMD sufferers are more likely to have a positive history of trauma compared with non-TMD sufferers.13 Such trauma may result from external injury, yawning and prolonged opening, as may occur during dental treatment. It may also occur as a result of a variety of parafunctional activity (eg as assessed by the Oral Behaviours Check List13), but parafunctional behaviour may be difficult to measure as it may occur whilst the patient is asleep.
Free radical damage of the TMJ
Recent research suggests that free radicals may be released in the joint capsule as a result of parafunctional stresses.60 If these free radicals build up excessively they can exert a degenerative effect on the TMJ tissues. Such a build-up may result from a defective scavenger system for free radicals. The research breakthrough is that the patient's genotype may determine how effectively the scavenger system works.60
Peripheral and central sensitization
Another significant research finding relates to peripheral and central sensitization, which has been extensively studied in other parts of the body. These two effects effectively amplify the sensation of pain through mechanisms acting along the neuronal track to the brain (peripheral sensitization) or within the brain itself (central sensitization).
A neuropeptide, ‘calcitonin gene-related peptide’ (CGRP), known to be influential in such sensitization, has been demonstrated to cause cellular changes inside the TMJ capsule, which promote and maintain peripheral sensitization. Indeed, elevated levels of CGRP are known to be indicative of mobility impairment and pain in the temporomandibular complex.61 An exciting development would be if CGRP could be targeted for future therapy.62 Widespread pain, outside of the orofacial region, can also accompany the more localized TMDs and recent research has identified several pro-inflammatory cytokines and anti-inflammatory cytokines associated with the presentation of widespread pain alongside TMDs63 and these also could offer potential therapeutic targets.
Cortical changes in TMD and during splint wear
Research on cerebral constitution (eg using functional magnetic resonance imaging, fMRI, which measures changes in blood supply to brain regions) has highlighted the degree of neuroplasticity inherent in sufferers of TMDs. These patients show cortical changes related to pain duration, pain unpleasantness, and pain intensity.64
fMRI studies on the cerebral representation of the TMJs in pain-free controls fitted with stabilization splints have shown decreased activation within affective and sensorimotor areas of the brain, thereby for the first time giving some indication of a potential central mode of action of stabilization splints.65
TMDs and genetic polymorphisms
A polymorphism is a variation in DNA sequence, which is relatively common within the population. Genomic research linking TMDs to polymorphisms in the genes, which encode a number of enzymes, involved in tissue maintenance and neuronal transmission has emerged,66,67,68 including catechol-O-methyltransferase (COMT). COMT degrades catecholamines after they have been released at neuronal synapses, so patients with deficient levels of the enzyme have a lower pain threshold and are more likely to develop TMD. The COMT polymorphism effect has recently been shown to be modified by lifetime incidence of depressive symptoms,69 thereby beginning to help explain the association between chronicity of TMDs and depression.70 All of these polymorphisms may, in the future, help tailor management to the individual's genetic make-up.
Conclusion
TMDs encompass a range of complex conditions, which exert varying biopsychosocial impacts. They can be reliably diagnosed using the RDC/TMD or similar system. Where dentists refer patients to secondary care, they should make the diagnosis clear to the patient. In most patients, the initial management is conservative and reversible in nature, can effectively be delivered in practice and involves explanation of the condition, prescribing exercises, a splint (preferably full coverage) and appropriate analgesia. Ongoing research into the genetic basis for TMDs may give vital information to aid management of TMDs in individuals susceptible to this problem.