Renton T, Adey-Viscuso D, Meechan JG, Yilmaz Z. Trigeminal nerve injuries in relation to the local anaesthesia in mandibular injections. Br Dent J. 2010; 209:(9)
Renton T, Yilmaz Z. Profiling of patients presenting with posttraumatic neuropathy of the trigeminal nerve. J Orofac Pain. 2011; 25:(4)333-344
Teixeira MJ, de Siqueira SR, Bor-Seng-Shu E. Glossopharyngeal neuralgia: neurosurgical treatment and differential diagnosis. Acta Neurochirurgica. 2008; 150:(5)471-475
Rokyta R, Fricova J. Neurostimulation methods in the treatment of chronic pain. Physiol Res/Acad Scient Bohemoslov. 2012; 61:S23-S31
Oomen KP, van Wijck AJ, Hordijk GJ, de Ru JA. Effects of radiofrequency thermocoagulation of the sphenopalatine ganglion on headache and facial pain: correlation with diagnosis. J Orofac Pain. 2012; 26:(1)59-64
Cruccu G, Anand P, Attal N, Garcia-Larrea L, Haanpaa M, Jorum E EFNS Guidelines on Neuropathic Pain Assessment. Eur J Neurol. 2004; 11:(3)153-162
Moazzam AA, Habibian M. Patients appearing to dental professionals with orofacial pain arising from intracranial tumors: a literature review. Oral Surg Oral Med Oral Pathol Oral Radiol. 2012; 114:(6)749-755
Zakrzewska JM, Akram H. Neurosurgical interventions for the treatment of classical trigeminal neuralgia. Cochrane Database Syst Rev. 2011; (9)
Cruccu G, Gronseth G, Alksne J, Argoff C, Brainin M, Burchiel K AAN-EFNS guidelines on trigeminal neuralgia management. Europ J Neurol. 2008; 15:(10)1013-1028
Renton T, Yilmaz Z. Managing iatrogenic trigeminal nerve injury: a case series and review of the literature. Int J Oral Maxillofac Surg. 2012; 41:(5)629-637
Baad-Hansen L. Atypical odontalgia – pathophysiology and clinical management. J Oral Rehabil. 2008; 35:(1)1-11
List T, Leijon G, Svensson P. Somatosensory abnormalities in atypical odontalgia: a case-control study. Pain. 2008; 139:(2)333-341
List T, Leijon G, Helkimo M, Oster A, Dworkin SF, Svensson P. Clinical findings and psychosocial factors in patients with atypical odontalgia: a case-control study. J Orofac Pain. 2007; 21:(2)89-98
Mongini F, Rota E, Evangelista A, Ciccone G, Milani C, Ugolini A Personality profiles and subjective perception of pain in head pain patients. Pain. 2009; 144:(1–2)125-129
Farrar JT, Young JP, LaMoreaux L, Werth JL, Poole RM. Clinical importance of changes in chronic pain intensity measured on an 11-point numerical pain rating scale. Pain. 2001; 94:(2)149-158
Mick G, Correa-Illanes G. Topical pain management with the 5% lidocaine medicated plaster – a review. Curr Med Res Opin. 2012; 28:(6)937-951
Affolter B, Thalhammer C, Aschwanden M, Glatz K, Tyndall A, Daikeler T. Difficult diagnosis and assessment of disease activity in giant cell arteritis: a report on two patients. Scand J Rheumatol. 2009; 38:(5)393-394
Renton T, Yilmaz Z. Profiling of patients presenting with posttraumatic neuropathy of the trigeminal nerve. J Orofac Pain. 2011; 25:(4)333-344
Aggarwal VR, Tickle M, Javidi H, Peters S. Reviewing the evidence: can cognitive behavioral therapy improve outcomes for patients with chronic orofacial pain?. J Orofac Pain. 2010; 24:(2)163-171
Kirsch DL, Nichols F. Cranial electrotherapy stimulation for treatment of anxiety, depression, and insomnia. Psych Clins N Am. 2013; 36:(1)169-176
Arch JJ, Eifert GH, Davies C, Plumb Vilardaga JC, Rose RD, Craske MG. Randomized clinical trial of cognitive behavioral therapy (CBT) versus acceptance and commitment therapy (ACT) for mixed anxiety disorders. J Consult Clin Psychol. 2012; 80:(5)750-765
Fledderus M, Bohlmeijer ET, Pieterse ME, Schreurs KM. Acceptance and commitment therapy as guided self-help for psychological distress and positive mental health: a randomized controlled trial. Psychol Med. 2012; 42:(3)485-495
McCracken LM, Gutierrez-Martinez O. Processes of change in psychological flexibility in an interdisciplinary group-based treatment for chronic pain based on Acceptance and Commitment Therapy. Beh Res Therapy. 2011; 49:(4)267-274
Cammin-Nowak S, Helbig-Lang S, Lang T, Gloster AT, Fehm L, Gerlach AL Specificity of homework compliance effects on treatment outcome in CBT: evidence from a controlled trial on panic disorder and agoraphobia. J Clin Psychol. 2013; 69:(6)616-629
Wolitzky-Taylor KB, Arch JJ, Rosenfield D, Craske MG. Moderators and non-specific predictors of treatment outcome for anxiety disorders: a comparison of cognitive behavioral therapy to acceptance and commitment therapy. J Consult Clinical Psychol. 2012; 80:(5)786-799
Jurgens TP, Muller P, Seedorf H, Regelsberger J, May A. Occipital nerve block is effective in craniofacial neuralgias but not in idiopathic persistent facial pain. J Headache Pain. 2012; 13:(3)199-213
Zakrzewska JM. Multi-dimensionality of chronic pain of the oral cavity and face. J Headache Pain. 2013; 14:(1)
Zakrzewska JM, Jassim S, Bulman JS. A prospective, longitudinal study on patients with trigeminal neuralgia who underwent radiofrequency thermocoagulation of the Gasserian ganglion. Pain. 1999; 79:(1)51-58
Leo RJ, Latif T. Repetitive transcranial magnetic stimulation (rTMS) in experimentally induced and chronic neuropathic pain: a review. J Pain. 2007; 8:(6)453-459
Oral A, Ilieva EM, Kucukdeveci AA, Varela E, Valero R, Berteanu M Generalised and regional soft tissue pain syndromes. The role of physical and rehabilitation medicine physicians. The European perspective based on the best evidence. A paper by the UEMS-PRM Section Professional Practice Committee. Europ J Phys Rehab Med. 2013; 49:(4)535-549
Nizard J, Raoul S, Nguyen JP, Lefaucheur JP. Invasive stimulation therapies for the treatment of refractory pain. Discov Med. 2012; 14:(77)237-246
Sarsam Z, Garcia-Finana M, Nurmikko TJ, Varma TR, Eldridge P. The long-term outcome of microvascular decompression for trigeminal neuralgia. Br J Neurosurg. 2010; 24:(1)18-25
Zakrzewska JM, McMillan R. Trigeminal neuralgia: the diagnosis and management of this excruciating and poorly understood facial pain. Postgrad Med J. 2011; 87:(1028)410-416
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
Honorary Clinical Researcher, Department of Oral Surgery, King's College London Dental Institute, King's College Hospital London, Bessemer Road, London SE5 9RS, UK
Orofacial chronic pain provides a significant challenge to all clinicians and the patients seeking treatment for it. Due to the anatomical and regional complexities, diagnosis can be extremely difficult, and due to the lack of cross specialty training, patients will undergo a variety of treatment under different disciplines. Dysfunctional pain provides a unique challenge for patient management and requires a multidisciplinary team.
Clinical Relevance: Lack of recognition of dysfunctional chronic pain can result in inappropriate dental treatment and further damage. to the patient. Appropriate patient reassurance and referral to an orofacial pain multidisciplinary team is recommended as most of these conditions require medical management.
Article
Persistent post-surgical pain without demonstrable neuropathy
This is defined as pain that is present one year or longer post-surgical procedure, that is unexplained by local factors and is best described as neuropathic in nature.
Non-odontogenic dysfunctional pain is often difficult to diagnose because it is poorly understood.1 Even defining and categorizing such persistent pain is challenging. Non-odontogenic pain may represent half of all cases of persistent tooth pain, as shown by a recent systematic review of prospective studies that reported the frequency of non-odontogenic pain in patients who had undergone endodontic procedures. Non-odontogenic pain was defined as dento-alveolar pain present for 6 months or more after endodontic treatment without evidence of dental pathology. Endodontic procedures reviewed were non-surgical root canal treatment, retreatment, and surgical root canal treatment: 770 articles were retrieved and reviewed, 10 met the inclusion criteria with a total of 3,343 teeth enrolled within the included studies; 1,125 had follow-up information regarding pain status. The authors identified non-odontogenic pain in 3.4% (95% confidence interval, 1.4–5.5% frequency of occurrence).2
The prevalence of persistent post-surgical pain in the trigeminal system may be low compared with other surgical sites. However, a recent report highlights the importance of dentists' awareness of neuropathic pain (NePain) before trying to solve apparent ‘toothache’ with conventional dental treatment, which will not be effective and results in additional harm to the patient.3
However, when one considers the significant frequency of dental surgical procedures undertaken, then significant numbers of individuals should be affected by both post-traumatic neuropathy and persistent post-surgical pain but, fortunately, the condition remains rarely associated with dentistry. This may be because most procedures are performed under local anaesthetic, which helps prevent central sensitization.
Risk factors for developing persistent post-surgical pain include:
Genetics (deficiency of the enzyme catecholamine-O-methyltransferase);
The surgical procedure and technique (tension due to retraction).4
All these persistent post-surgical pain conditions may be attributable to post-traumatic neuropathy but it is difficult to be conclusive without a demonstrable neuropathic area in relation to the previous surgery.
Idiopathic or dysfunctional chronic pain
This group includes persistent idiopathic facial pain (PIFP formerly known as atypical facial pain), persistent idiopathic intra-oral pain (formerly known as atypical odontalgia) and possibly burning mouth syndrome (BMS Paper 8) and a sub-group of temporomandibular disorders, persistent myalgia or arthromyalgia (Paper 6). However, BMS is increasingly being recognized as a neuropathic pain and perhaps should be reclassified.
Persistent idiopathic facial pain (PIFP)
Frazier and Russell introduced the term atypical facial pain in 1924. It has since been renamed persistent idiopathic facial pain (PIFP).5 PIFP refers to chronic persistent pain within the distribution of the trigeminal nerve not commensurate with the classic presentation of other cranial neuralgias.1 The duration of pain is usually long-lasting for most of the day (if not continuous). Pain is often unilateral and without autonomic signs or symptoms and it often radiates in areas not supplied by the same sensory nerve, ie the pain does not follow neurological dermatome boundaries. It is described as a severe ache, crushing or burning sensation for which no cause can be found. The PIFP patient will often present with years of facial pain that has not changed in level or characteristics during long periods, with the exception of those persistently seeking care undergoing regular interventions, which often provide relief for a few months before the same pain returns.
Definition
The International Association for the Study of Pain (IASP)5 defines chronic facial pain as facial pain symptoms which have been present for at least 6 months. ‘Atypical’ pain is a diagnosis of exclusion, when all other conditions have been eliminated as a potential cause (ie it is idiopathic), and is characterized by chronic, constant pain in the absence of any apparent cause in the face or brain.
Previously idiopathic facial pain conditions may have included neuropathic pain due to sensory nerve damage, complex regional pain syndrome (CRPS) from sympathetic nerve damage, atypical facial pain1 and atypical odontalgia, or phantom tooth pain.
Epidemiology and features of PIFP include:
Estimated incidence is 1 case per 100,000 population, although this number may be underestimated;
PIFP affects both sexes approximately equally, but more women than men seek medical care. The disorder mainly affects adults and is rare in children. Patients are aged between 30 and 50 years;
The maxillary region;
In a small number of patients the pain may be one consequence of significant psychological or psychiatric disease.6,7
Clinical presentation
PIFP has a very variable presentation. Often it is characterized by continuous, daily pain of variable intensity, usually moderate to severe. Typically, the pain is deep and poorly localized, is described as dull and aching, and does not waken the patient from sleep. At onset the pain may be confined to a limited area on one side of the face, while later it may spread to involve a larger area non-compliant with sensory dermatomes. The pain is not triggered and is not ‘electrical’ in quality. The description of the pain may be inconsistent because the patient can complain of bilateral pain that often changes locations over weeks to months. Intensity fluctuates but the patient is rarely pain-free. Pain is typically located in the face and seldom spreads to the cranium in contradistinction to tension headache.
Psychological features
Between 60% and 70% of these patients have significant psychiatric findings, including:
Depression;
Somatization;
Adjustment disorders.
Therefore psychiatric evaluation and therapy is indicated in all cases.6,7,8,9 Medical treatment of PIFP is usually less satisfactory than medical treatment for other facial pain syndromes.1 There are several guidelines for the medical management of chronic orofacial pain.10,11,12,13 Medical treatment commonly utilized for PIFP includes:
Antidepressants;
Tricyclic antidepressants;
Serotonin and norepinephrine re-uptake inhibitors (SNRIs); and
Membrane stabilizers (gabapentin and pregabalin).
The mechanisms of these drugs vary and all have significant side-effects for the patient, often compromising compliance with medication. Of these classes of medications, anticonvulsants and antidepressants appear to be the most effective as the neuropathic component of pain responds well to them. Pharmacotherapeutic knowledge is paramount in the treatment of this refractory pain syndrome.11
A multi-mechanistic approach, using modulation of both peripheral and central components of the ascending and descending pain pathways, is necessary. The goal of therapy is to manage the pain effectively with the fewest adverse medication effects, whilst ensuring that the patient has realistic expectations. Alternative therapies, such as acupuncture and neuromuscular re-education, should be considered as part of a comprehensive treatment plan. Psychological interventions are an essential component in the overall management of a patient with chronic pain.
The term atypical odontalgia (AO) is a confusing and controversial condition, now defined by the International Headache Society14 as a subgroup of persistent idiopathic facial pain (PIFP), which is described as ‘persistent facial pain that does not have the characteristics of the cranial neuralgias and is not attributed to another disorder’.14 This condition was first introduced to the medical community by the English anatomist and surgeon, John Hunter (1728–1793). The Academy of Orofacial pain defines atypical odontalgia (AO) as
…‘also known as atypical facial pain or phantom tooth pain, is characterized by chronic pain in a tooth or teeth, or in a site where teeth have been extracted, without an identifiable cause. Over time, the pain may spread to involve wider areas of the face or jaws. The intensity of the pain can vary from very mild to very severe. There is typically no identifiable cause to explain the pain and it often follows or is associated with a history of some type of dental procedure such as having a root canal or tooth extraction. This often presents a frustrating and confusing situation for both the patient and the dentist, and can lead to more and more dental treatment, none of which is effective at relieving the pain.’11
The pain remains constant despite repeated dental treatment, even extractions in the region, often rendering patients with persistent pain but whole quadrants stripped of dentition.
AO has been well characterized recently by Baad-Hansen,15 List et al,16 and Benoliel et al.2 AO patients have more comorbid pain conditions, higher scores for depression and somatization, significant limitation in jaw function, and lower scores on quality of life measures when compared with controls,16 when compared to patients with TMD. AO patients were more likely to describe their pain as aching, find rest relieving but cold and heat aggravating. Over 80% relate the onset of their pain to dental treatment. These somatosensory abnormalities suggest generalized sensitization of the nociceptive mechanism. The author believes that the relationship with previous surgical intervention infers that this condition may, in some cases, be partial postsurgical neuropathy of the superior alveolar nerves. This concept is substantiated by persistent post-endodontic dental pain.2
The diagnosis of AO is often difficult, and is based on exclusion of common conditions in teeth or adjacent structures with known pathophysiology. Diagnostic local anaesthetic blocks may be useful, especially when a local (eg dental) peripheral pathological process is suspected. In addition, ascertaining a history as to whether the pain responds to antibiotics (indicating infective inflammatory process) or NSAIDs or Paracetamol (indicating a likely inflammatory pain) is essential to qualify the NePain diagnosis. The lack of randomized controlled trials (RCTs) makes evidenced-based care in AO difficult.16 Similar to other neuropathic pain conditions, AO is difficult to manage effectively. Treatment of neuropathic pain is complex and challenging, and consideration must be given to both peripheral and central mechanisms. One of the major problems with managing this condition is convincing patients, and informing their dentist, that there are no dental causes for their pain, so avoiding unnecessary irreversible invasive dental treatment. AO patients are often diagnosed late and therefore need a multidisciplinary approach. In her recent review, Baad-Hansen15 presents a sensible progressive approach to managing AO, beginning with topical lidocaine or capsaicin, then tricyclic anti-depressants. Ultimately, the drugs used in neuropathic pain are often gabapentin and pregabalin, tramadol or oxycodone.
There may be weak evidence that Botox injections may provide long-term temporary relief for AO. However, complications, such as facial nerve palsy/weakness, may preclude this intervention becoming routine practice.
In summary, better education of the dental profession is essential to prevent both patient and dentist from falling into the ‘over prescription of dental interventions’ for neuropathic pain. Although AO has a distinct presentation from routine toothache, this may not be absolutely clear early on. A simple strategy that should be adopted by all dental professionals is to ask a simple question, ‘Does the pain respond to paracetamol or ibuprofen?’ if the answer is a categorical ‘no’ then neuropathic pain must be considered as this confirms it is not routine inflammatory ‘dental’ pain.
Management strategies for neuropathic pain
Systemic analgesia
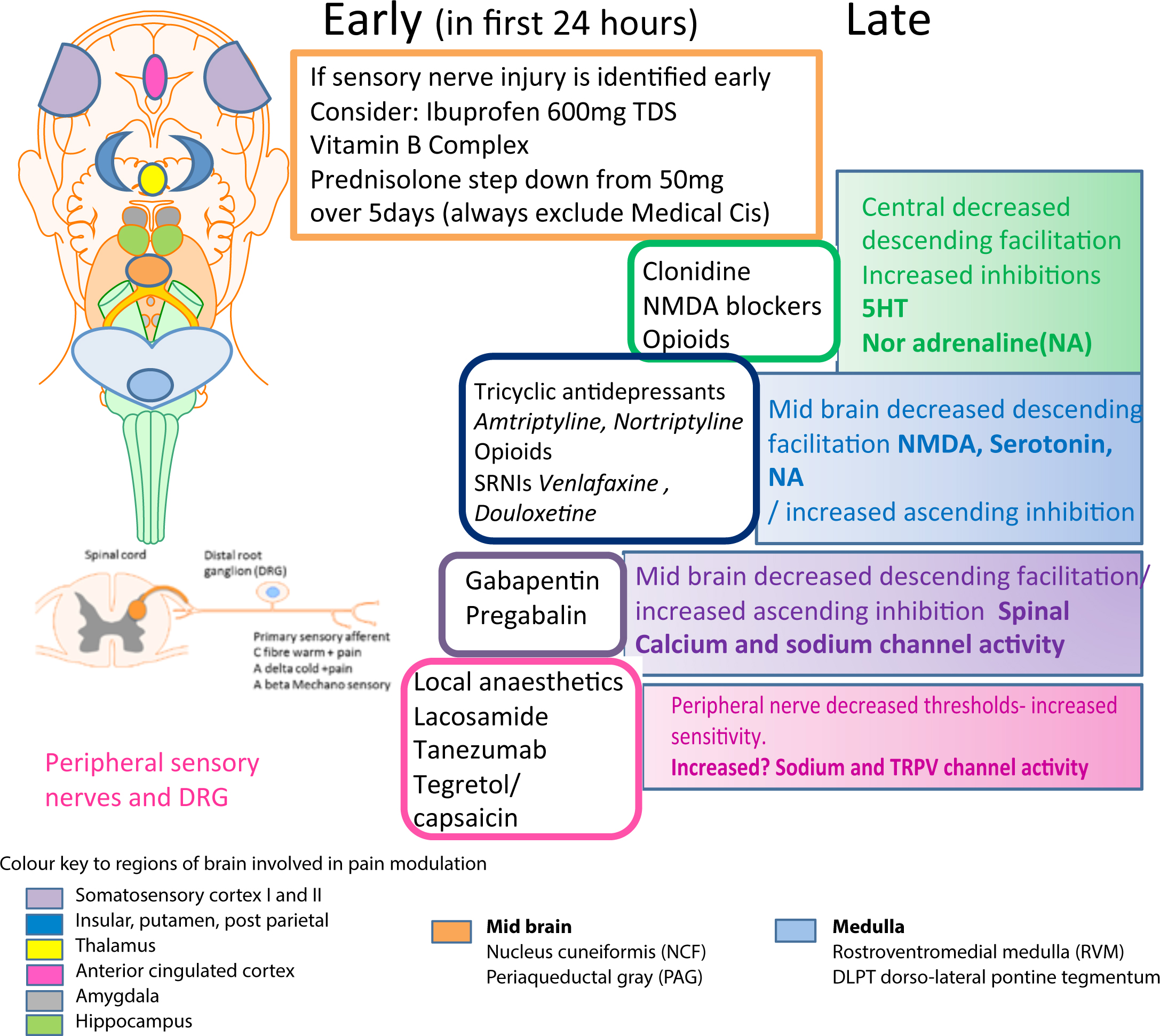
IASP,10,13 AAOP11,12 and NICE17 have recommended medical guidelines for neuropathic pain. Low dose anti-depressants (amitriptyline, nortriptyline), and/or anti-epileptic agents (carbamazepine, oxcarbamazepine, gabapentin, pregabalin) can be used to manage pain experienced by patients with post-traumatic neuropathy (Table 1). However, such systemic medications can cause a multitude of side-effects that the patients would find hard to cope with in addition to their existing morbidity (Table 2). Mechanisms of known action of the recommended drugs for NePain are summarized in Figure 1.
*Investigational drug (approval pending from US Food and Drug Administration).
Drug
Contra-indications
Main Side-effects
Tricyclic Anti-depressants
Amitriptyline
Nortriptyline
10 mg nocte raising 10 mg per week up to 40 mg nocte-maintenance dose
Cardiac conduction abnormalities, recent cardiac events, narrow-angle glaucoma, elderly patients, epilepsy, bipolar disorder. TCAs may enhance the response to alcohol and the effects of barbiturates and other CNS depressants
Dry mouth, constipation, urinary retention, sedation, weight gain
Side-effects: nausea, sedation, decreased libido, sexual dysfunction, headache, weight gain
Anti-epileptics
Tegretol Carbamazepine
Liver disease, acute intermittent porphyria, hyponatremia, a serious blood disorder, marrow depression, taken an MAO inhibitor within the past 14 days. 8% rashes that may be very serious are more likely to occur in people with a particular gene called ‘HLA-B*1502’. This gene occurs almost exclusively in patients with ancestry across broad areas of Asia, including South Asian Indians. Patients with ancestry from these areas should have a blood test by their physician to see if they have the ‘HLA-B*1502’ gene before starting treatment
Dizziness, diplopia, nausea. Treatment can result in aplastic anaemia
Figure 1. Medical management for chronic pain related to mechanisms of known action of the recommended drugs. (Neuropathic pain – pharmacological management: The pharmacological management of neuropathic pain in adults in non-specialist settings NICE guidelines [CG173]. Published date: November 2013 https://www.nice.org.uk/guidance/cg173).
However, there is undoubtedly a consensus that a multidisciplinary approach will maximize addressing the complex and numerous multiple factors contributing to the patients' pain experience. Several emerging strategies are discussed below.
Topical analgesia
Novel strategies that include a combination of topical 5% lidocaine patches, topical clonazepam and botulinum toxin injections may be effective for managing post-traumatic trigeminal neuropathic pain.
Patches containing lidocaine have successfully reduced the pain experience amongst patients with post-herpetic neuralgia (PHN), painful diabetic neuropathy, and low back pain.18,19 A small proportion of IANI patients experiencing neuropathic pain in a recent study were managed by applying topical 5% lidocaine patches to the area in which they were experiencing pain, and this therapy provided significant pain relief.17,18 However, clinicians prescribing these topical patches should warn the patients to discontinue use of the patch if they develop a rash, since the patches are applied overnight on a 12 hour-on and 12 hour-off cycle. This modality is very useful for patients suffering from sleep interruption due to mechanical allodynia.17 The combined application of topical 5% lidocaine patches with other modalities is potentially a simple useful strategy for patients with permanent inferior alveolar nerve injury suffering from neuropathic pain.
Some evidence has shown that botulinum toxin injections are useful in managing peripheral extra-oral or intra-oral sensory neuropathic pain,16 however, evidence of its effective use for post-traumatic trigeminal pain remains limited.
Clonazepan (used topically as a crushed 300 mg tablet) applied to the mucosa for 3–5 minutes, and not swallowed, followed by rinsing, may reduce oral mucosal neuropathic pain, but evidence is weak for widespread application of this technique.20
Psychiatric and psychological therapies
It is well established that patients who develop chronic orofacial pain conditions undergo marked negative psychological and personality changes,21,22 and display increased levels of anxiety, depression, and psychosocial distress.9 Significantly, a number of recent studies have reported reduced quality of life, impaired psychosocial functioning, and elevated levels of anxiety and depression in patients suffering from orofacial pain with a neuropathic component, such as patients diagnosed with trigeminal neuralgia and idiopathic continuous orofacial pain.9,23
Assessment and treatment by a psychiatrist and clinical psychologist can help in the management of these psychological changes in these patients. The iatrogenic nature of many nerve injuries can compound pre-existing mental health problems and, interestingly, evidence suggests that treating concomitant anxiety and depression can lead to a decrease in pain.23,24
Therapies with the best evidence for chronic pain are cognitive-behavioural therapy (CBT)25,26 and Acceptance and Commitment Therapy (ACT).27 These therapies are not intended to lower the patients' perceived pain levels, but enable patients to cope with their pain better. This often includes the acceptance by patients of the presence of their chronic condition.
Cognitive-behavioural therapy currently has the largest amount of research carried out on its effectiveness, and is recommended by NICE for a wide variety of mental health and behavioural conditions. CBT focuses on what people think, how those thoughts affect them emotionally, and how they ultimately behave as a result. When patients are distressed or anxious, the manner in which they see and evaluate themselves can become negative. CBT therapists work alongside patients to help them begin to see the link between negative thoughts and mood. This empowers patients to assert control over negative emotions and to change to modify their behaviour.
A trained therapist, usually in a clinical setting, delivers CBT. During CBT, the therapist will first assist in identifying the problem (along with the behaviour, thoughts, and feelings that may be linked to the problem). Once the problem has been explored, the therapist will help to examine the thought and behaviour patterns and help to work on ways of changing these patterns. If patients access this type of therapy, they will often be provided with a set number of sessions that typically last 50 minutes per session. Therapists will usually set ‘homework tasks’ that are completed between sessions. Homework tasks may include carrying out activities such as thought monitoring and entering these into a thought diary, or practising specific behaviours through what is known as ‘behavioural exposure’.28
Cognitive behavioural approaches are delivered in a number of clinical settings, with various differing protocols. While the cognitive elements of the programme are usually the province of psychologists, other staff working alongside them, such as physiotherapists, occupational therapists, nurses and doctors, are required to improve their psychological understanding and skills to enable them to contribute to the treatment regimen. Not surprisingly, the outcomes vary greatly between individual patients, with some subjects finding the ideas life-changing in their relevance and applicability, while others struggle to make even small changes. Studies demonstrate that, although there is some diminution in effect with time, most patients never return to their previous levels of distress or disability.28
Cognitive-behavioural therapy (CBT) alone, or within the context of an interdisciplinary pain rehabilitation programme, has the greatest empirical evidence for success in patients with chronic pain conditions,28 and there is emerging evidence that CBT-based treatment methods can improve both short-term and long-term outcomes in patients with chronic orofacial pain.23 However, thus far there is no evidence of the benefits of CBT for patients with IANI or LNI induced neuropathic pain.
There are an increasing number of studies qualifying the role of CBT in the management of chronic pain, however, more recently, several novel techniques are gaining credibility in this field, including ACT.27 Acceptance and Commitment Therapy is a third wave behavioural therapy (along with Dialectical Behaviour Therapy and Mindfulness Based Cognitive Therapy) that uses mindfulness skills to develop psychological flexibility and help clarify and direct values-guided behaviour. ACT (pronounced ‘act’ and not by the initials ‘A-C-T’) does not attempt to change or stop unwanted thoughts or feelings directly, but aims to develop a new mindful relationship with those experiences to free a person up to be open to take action that is consistent with his/her chosen life values. Thus, values clarification is a key component to ACT.
Evidence suggests that ACT can help to improve mental health.24 In a comparative trial with CBT, ACT was shown to have comparable outcomes (there is increasing evidence to support its use with chronic pain in both a group and individual setting).29
Other non-surgical interventions
Other non-surgical interventions include; education, transcutaneous electrical nerve stimulation (TENS), peripheral nerve stimulation, massage, acupuncture, and exercise/reconditioning. These strategies have mainly been explored for chronic pain management applicable to many patients with permanent trigeminal nerve injuries.1
Combined therapies
These include CBT, surgery and medication with 5% lidocaine patches and/or botulinum toxin.
Surgical interventions
Details of neurosurgical interventions are beyond the scope of the dentist and the domain of multidisciplinary pain management team. Various interventions include:
Percutaneous nerve blocks;
Occipital nerve block;
Trigeminal ganglion blocks.
In a recent study of 20 patients, occipital nerve block (ONBs) were found to be effective in trigeminal pain involving the second and third branches and seemed most effective in craniofacial neuralgias rather than PIFP.30 They should be considered in facial pain before more invasive approaches, such as thermocoagulation or vascular decompression, are performed, given that side-effects are mild and the procedure is minimally invasive.
Botox injections are effective in attenuating painful focal neuropathies and a recent case report highlights the potential for management of trigeminal neuralgia. Trigeminal ganglion blocks originally using ethanol but now superseded by glycerol injections were described in 1921. Balloon compression has also been used to ablate chronic trigeminal pain.
Another recent report claimed that a low level laser applied peripherally may also have a role to play in post-traumatic neuropathy and PIFP.31
Trigeminal ganglion radiofrequency uses the same approach as block techniques, using real-time fluoroscopy, but lidocaine is injected prior to the motor stimulation and identification of motor nerves is achieved.32 The patient is sedated during the procedure. Radiofrequency ‘neurodestructive’ thermo coagulation of the trigeminal/gasserian or the sphenopalatine ganglion are reported to have varied success rates, with pain often recurring.32
Pulsed radiofrequency is non-destructive and has a reported lower morbidity, with some success when applied extracranially to the affected peripheral nerve. However, they may have a role to play in late management of refractory chronic orofacial pain conditions with an autonomic element.
Extracranial nerve obliteration is rarely indicated and techniques using cryosurgery are becoming obsolete.32 Neuromodulation or neurostimulation techniques include:
Peripheral nerve stimulation (PNS);
Spinal cord stimulation (SCS);
Deep brain stimulation (DBS);
Motor cortex stimulation (MSC); and
Repetitive transcranial magnetic stimulation (rTMS).
These may have a role in chronic pain management.8,33,34,35 Such neuromodulatory (neurostimulatory) techniques are highly recommended for the treatment of different types of pharmacoresistant pain and may prove promising for TN and PIFP.
Microvascular decompression (MVD) is highly evidenced for the treatment of classical trigeminal neuralgia in patients with MRI confirmed vascular compromise of the trigeminal nerve stem. However, first line therapy remains medical using carbamazepine. The mortality rate for MVD may be as high as 1% thus, for compromised patients, the Gamma knife technique is gaining in popularity. However, the long-term pain relief is lower than for MVD.36,37
Conclusion
Chronic orofacial pain continues to present a diagnostic challenge for many practitioners. The most important part of the diagnostic process is time to listen and take a good history from the patient. Patients are frequently misdiagnosed and they can often suffer from multiple pain conditions, concomitant psychological/psychiatric symptoms of depression and anxiety, making them complex and hard work for the clinician.
Daily or near-daily orofacial pain (OFP) is a widespread problem for many patients. Importantly, the clinician must be competent to distinguish the many conditions, such as chronic daily headache syndromes, including hemicrania continua, TMJ syndrome, migraine, chronic cluster headache, SUNCT, TN, and many others from each other. Underlying pathology such as malignancy, vasculitis, infection, and central or peripheral demyelination may manifest early as neuralgia and, not until focal neurological deficits, imaging abnormalities, or laboratory abnormalities are discovered does the diagnosis become evident. Rare cases of referred pain must also be considered. A careful history and physical examination, including a dental consultation, laboratory studies, and imaging studies, may be necessary to rule out occult pathology.
A differential diagnostic must include possible neoplastic disease, which is often of most concern to the patient. A recent report highlights the red flags for this conditions as unilateral disease; acute episodic pain associated with a neuropathy.31 Undoubtedly, MRI screening of these patients is an invaluable tool in excluding detectable neoplasia and often reassuring for the patient. Treatment for chronic orofacial NePain is less effective than in other pain syndromes and a multidisciplinary approach treatment is desirable.