Professor of Cariology, Guy's, King's and St. Thomas' Schools of Medicine, Dentistry & Biomedical Sciences, Floor 25, Guy's Tower, Guy's Hospital, London Bridge, London SE1 9RT
Dentine becomes infected as a result of caries lesion formation on root surfaces and when lesions progress following cavitation of enamel lesions. However, this infection is unimportant because the driving force for lesion formation and progression is the overlying biofilm. This explains why root surface caries can be controlled by mechanical plaque control and fluoride, and restorations are not needed to arrest these lesions. Similarly, the infected dentine in cavitated coronal lesions does not have to be removed to arrest the lesion. If the lesion is either accessible or opened for cleaning by the patient or parent, the lesion can be arrested. Sealing of infected dentine within the tooth, either by a Hall crown in the primary dentition or by partial caries removal prior to placing a well-sealed filling, will also arrest the lesion. When restoring deep lesions in symptomless, vital teeth, vigorous excavation of infected dentine is likely to expose the pulp and make root canal treatment necessary. Thus ‘complete excavation’ is not needed and should be avoided.
CPD/Clinical Relevance: Root surface caries can be arrested by cleaning and fluoride application. Restorations are not essential. Vigorous excavation of softened dentine in deep cavities of symptomless, vital teeth is contra-indicated. It is not needed and increases the risk of pulp exposure.
Article
Edwina Kidd Ole Fejerskov Bente Nyvad
Caries, the biofilm and caries control
Dental caries is a result of dynamic processes occurring in a dental biofilm. It is a chemical dissolution brought about by metabolic activity in the microbial deposit (biofilm or plaque) covering a tooth surface at any given time. This metabolic activity results in numerous fluctuations in pH at the interface between the biofilm and tooth surface. Over time these fluctuations may result in a disturbance of the equilibrium between the tooth mineral and the surroundings. Mineral loss, subsequent lesion formation and possible cavity formation in teeth, is a symptom of an imbalance in these dynamic processes and is designated ‘dental caries’.1 Biofilm formation and its metabolism is an ubiquitous natural process; it is part of having teeth. However, its possible consequence, lesion formation and progression, can be controlled so that a clinically visible lesion never forms or an established lesion arrests. The term caries control (rather than caries prevention) reflects the fact that biofilm formation and metabolism cannot be prevented but lesion formation and progression can be controlled so that lesions never become visible or established lesions arrest. Control of the biofilm is the treatment of caries.2 The most important control measures are to clean teeth regularly, and thus disturb the biofilm mechanically, with a fluoride-containing toothpaste and regulate sugar intake.
Lesions, whether in enamel or dentine, surface intact or cavitated, can be arrested by biofilm control alone provided the lesion can be accessed for cleaning. Where a cavitated lesion is not accessible, a filling may be required. However, insertion of fillings without reinforcement of plaque control is malpractice. Fillings do not ‘treat’ caries; they merely serve to hide the symptom. Fillings cannot prevent further caries attack and placing them, without addressing the cause of lesion formation in the first place, is a waste of time and money. It is tantamount to repairing a fire damaged building before putting out the flames.
Is caries an infectious disease?
Although caries is caused by the bacteria in the biofilm it is not an infectious disease in a classical sense. The dental biofilm consists of commensal organisms, not extraneous infecting invaders. Caries lesions are the result of ecological disturbances to the biofilm community. These disturbances originate in the metabolic activity of the host's own microflora in response to various external factors.
Oral bacteria are ultimate adaptors and survivors to the situations they find themselves in! Two examples of adaptation of the biofilm of great relevance to caries are an overgrowth of aciduric bacteria in response to increased sugar exposure or decreased salivary flow. This adaptation to the problem in hand is called the ecological plaque hypothesis.3 This not only explains why caries lesions develop, it also explains why some patients may not develop lesions despite tooth surfaces being constantly covered by biofilm. When caries develops it is therefore logical to focus on strategies to restore the ecological balance by measures such as mechanical plaque removal and sugar control.3
This paper will now concentrate on carious dentine when the enamel over it is cavitated or the dentine has no enamel cover, as in a root surface. This dentine is infected but, as will emerge, this infection is relatively unimportant. By ‘infected’ we mean that the dentine contains micro-organisms. The caries process is driven by the biofilm and control of the overlying biofilm is much more important than dealing with the infected dentine. It is time to lay a few ghosts, such as excavating and restoring teeth to remove infected dentine! But before this we need to take a brief detour to cover some relevant pathology.
Dentine lesions beneath demineralized, but uncavitated, enamel are a result of the biofilm metabolism on the tooth surface. The surface is accessible to cleaning and this is why these lesions can be arrested. They never justify operative intervention (Figure 1). The dentine is not infected.
Once a cavity forms lesion development is likely to progress as a result of bacterial metabolism. Micro-organisms invade the exposed dentinal tubules. This dentine is infected. Softening (demineralization) of the dentine often precedes the organisms responsible for it. It has been suggested that the dentist should remove infected dentine and leave affected dentine which is capable of remineralization. However, infected and affected dentine are histological concepts and the dentist cannot know for sure where they are in the lesion when dealing with it clinically.
Dentine is a vital tissue containing odontoblast processes and dentine and pulp must be considered together.
Dentine mounts a cellular, driven defence to the metabolic processes in the biofilm, resulting in a zone of tubular mineralization – the so-called translucent zone. In histological sections this zone appears translucent because the mineral in the tubules makes the tissue more homogeneous. This zone has sometimes been termed ‘sclerotic’ but this terminology is unfortunate because dictionaries define sclerotic as ‘becoming rigid and unresponsive; losing the ability to adapt’, but this is not really what is happening. Mineral is laid down within and around the tubules and the most relevant consequence of this is the permeability of the dentine is reduced. In addition, tertiary dentine may form at the pulp-dentine border (Figure 2) and this also reduces the permeability of the dentine.
In slowly progressing lesions, these odontoblastic reactions gradually ‘occlude’ the tubules and seal off the pathways between the oral environment and the pulp. This is a cute biological defence mechanism. In rapidly progressing dentine lesions, the odontoblasts may be destroyed and this results in open tubular pathways in the dentine. These tubules may therefore be accessed by bacteria.
When bacterial invasion penetrates the tertiary dentine there will eventually be a severely inflamed pulp followed by necrosis.
Figure 1. This lesion is accessible to cleaning and can be arrested. Operative intervention is contra-indicated.Figure 2. Four consecutive micro-computed tomography scans through a deep caries lesion in a 2000-year-old tooth from Imperial Rome. The lesion had penetrated into the pulp where tertiary dentine is indicated with an asterisk (a). Note the very pronounced translucent dentine reactions (tubular mineralization) that delineate the base of the dentine caries cavity – indicated by arrows on (b), (c) and (d). The framed area in (b) shows an early caries lesion through enamel with a dentine demineralization at the enamel-dentine border.
It is this pulpo-dentinal complex, with certain defence and inflammatory reactions, which the clinician interferes with when instituting operative treatment. It is unfortunate that the clinician cannot see the histological changes of infected dentine, affected dentine, tubular mineralization, tertiary dentine, pulpal inflammation, destruction of odontoblasts and pulpal necrosis. The clinician cannot know when excavating the depth of dentine that remains, how close the excavator is to exposure. To make matters worse, clinical symptoms relate poorly to pulp pathology and this is particularly unfortunate because the clinician needs to assess whether the pulp is likely to survive. Clinicians use the terms reversible and irreversible pulpitis to predict whether a pulp is likely to survive or whether its removal is inevitable.
In reversible pulpitis the pain evoked by a hot, cold or sweet stimulus is of short duration, disappearing when the stimulus is removed. The clinician hopes to preserve a healthy, vital pulp. In irreversible pulpitis the pain persists for a while after removal of the stimulus, or pain occurs spontaneously, and the pulp is likely to be so damaged that it must be removed. The clinician uses a vitality test (reaction to hot, cold or electrical stimuli) to judge total pulp necrosis and it is extraordinary that this works at all because these tests stimulate nerves whereas vitality depends on blood supply! In other words, the vitality test is a surrogate marker; when nerves are gone, blood vessels are as well. It is remarkable that, taken together, these clinical markers work rather well; a symptomless, vital pulp can usually be saved provided the dentist is not obsessed with removing ‘infected’ dentine by cutting innumerable tubules of translucent dentine away and exposing the vital odontoblasts of sound dentine.
We will now consider two circumstances where infected dentine is present. These are root caries and dentine caries in cavitated lesions.
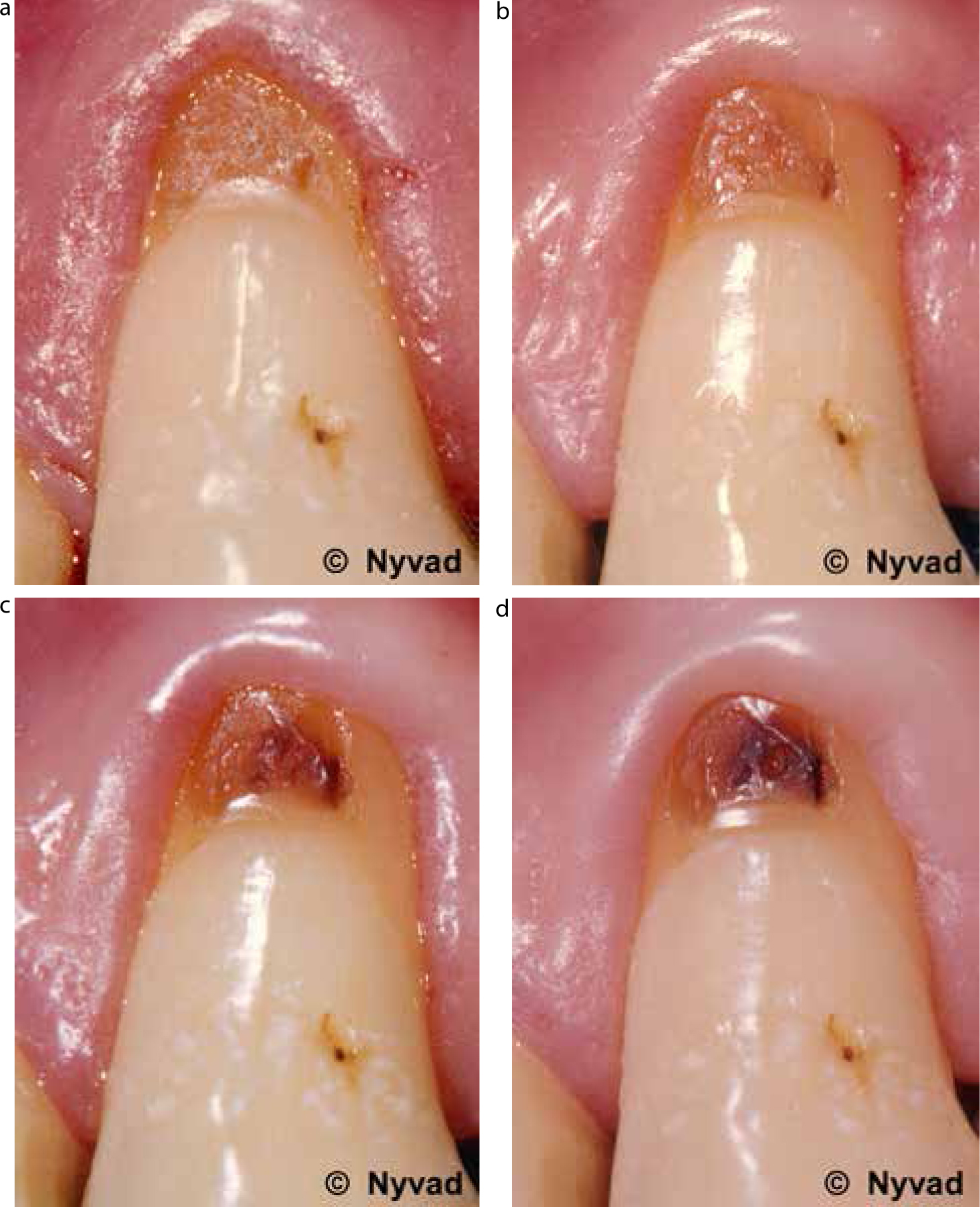
Figure 3 (a–d) is a rather well known illustration that has been reproduced in many textbooks and articles. The four pictures show a root caries lesion in an upper canine. In Figure 3a the lesion is active, it is soft and the dentine would be infected if it were to be sampled for culturing. Despite this infection, the lesion is driven by the biofilm at the tooth surface, not the infected dentine, and mechanically disturbing the biofilm regularly with a fluoride-containing toothpaste and fluoride application is the treatment required to transform the lesion from an active lesion to an arrested one. Over the months the soft surface is gradually worn away and the surface becomes hard due to mineral uptake in the surface layer, and it picks up stain. This is why it now looks dark brown (Figure 3d). Note this management puts the control where it has to be – with the patient. Would the lesion in Figure 3d yield micro-organisms if cultured? Certainly some, but they are of no consequence.
Figure 3.
(a–d) Consecutive stages of non-operative treatment of active non-cavitated root surface caries lesion on the buccal surface of upper left canine. The figure shows changes in the clinical appearance of the lesion after 3, 6 and 18 months. Note that, within the observation period, improved oral hygiene leads to gradual changes in colour and surface structure of the lesion, from soft and yellowish to hard and darkly discoloured. Note also changes in the topography of the marginal gingiva.
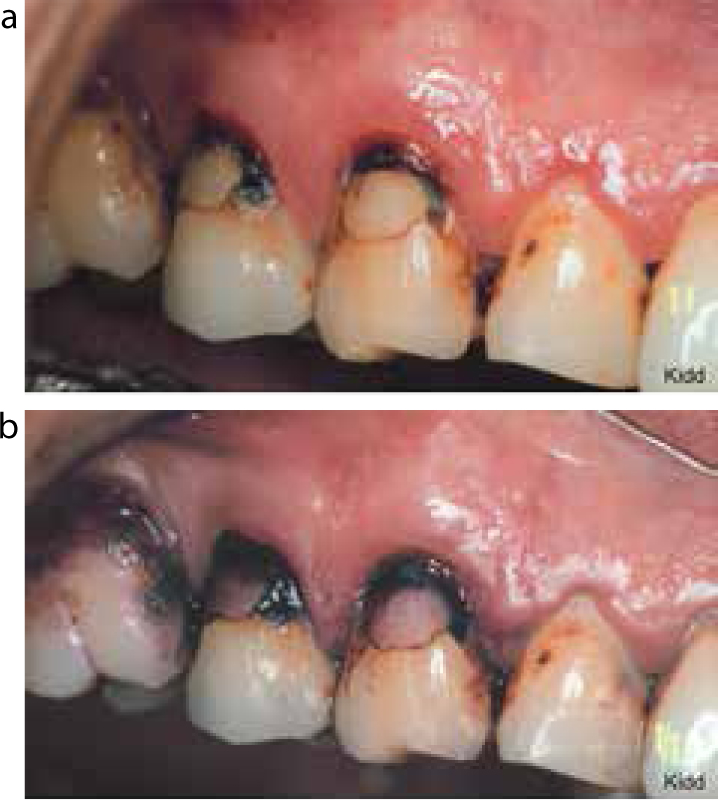
Contrast this to the lesion seen in Figure 4a and b. Here we see an active root caries lesion in a premolar and a dentist has placed a restoration some time previously, to no effect at all, as new caries has developed around the lesion and, when a disclosing solution is used, the surface of the lesion looks like a culture plate.
Figure 4.
(a) Root caries lesions buccal to upper premolars with previous tooth-coloured restorations sitting within new caries lesions. (b) Disclosing shows heavy biofilm deposits over the active lesions. To ‘treat’ these lesions restoratively would be ridiculous!
Finally, consider the lesions in Figure 5 (a–c). Initially, dentist and patient have concentrated on biofilm control. The incisal enamel has been trimmed to aid access for the brush, but then the patient is put in charge and, in Figure 5b, lesions are arresting. But how ugly they are! It is wonderful that we now have such beautiful restorative materials and adhesive techniques to improve appearance, but beware! It is tempting for the patient to believe that the dentist has solved the problem by filling the teeth (Figure 5c). Although the dentist has produced beautiful restorations, the real treatment is the biofilm control by the patient, and the fact that the dentine was infected is totally irrelevant!
Figure 5.
(a) Cervical lesions covered by plaque. (b) Same cavities after removing overhanging enamel with a diamond finishing bur and instruction in cleaning. Teeth were brushed twice a day with a toothbrush and toothpaste with fluoride. From a cariological point of view these teeth are now stable, but to improve their appearance they are to be restored with composite. (c) Completed restorations – the small colour difference is due to the teeth being dry and will disappear after some hours when they are wet with saliva.
Figure 6a shows a deciduous tooth where there is an active, cavitated lesion that cannot be cleaned. Something needs to be done to facilitate cleaning and, in this instance, the dentist, after discussion with the parent, has elected to ‘open’ the lesion for cleaning. This is rapidly done with a bur and no local anaesthetic is required. Now the parent is shown his/her essential role in caries control, which is daily removal of the biofilm with fluoride-containing toothpaste. The final picture taken 6 months later (Figure 6b) shows the lesion arrested and, provided the cleaning continues, this tooth should go symptomless to exfoliation. But the most important part of this management is the active role of the parent. This technique was called non-restorative cavity treatment and it is funded on the Health Service in Holland.
Figure 6. Non-restorative cavity treatment (NRCT). (Courtesy of Rene Gruythysen and BSL, Springer Media, Houten, the Netherlands.) (a) Caries in upper deciduous molars before using a bur to slice and open the teeth for cleaning. (b) Upper deciduous molars 6 months after NRCT. The caries lesions are arrested.
Note in this case that infected dentine was present but, just as in the root caries lesion (Figure 3), brushing has gradually removed the soft dentine and the surface of the lesion is now hard, shiny and coloured brown. The infected dentine was not immediately removed and this has had no detrimental consequence. In fact, this is exactly the same approach as is used in the non-operative treatment of active non-cavitated lesions and perhaps it would be more appropriate to call it non-operative cavity treatment.
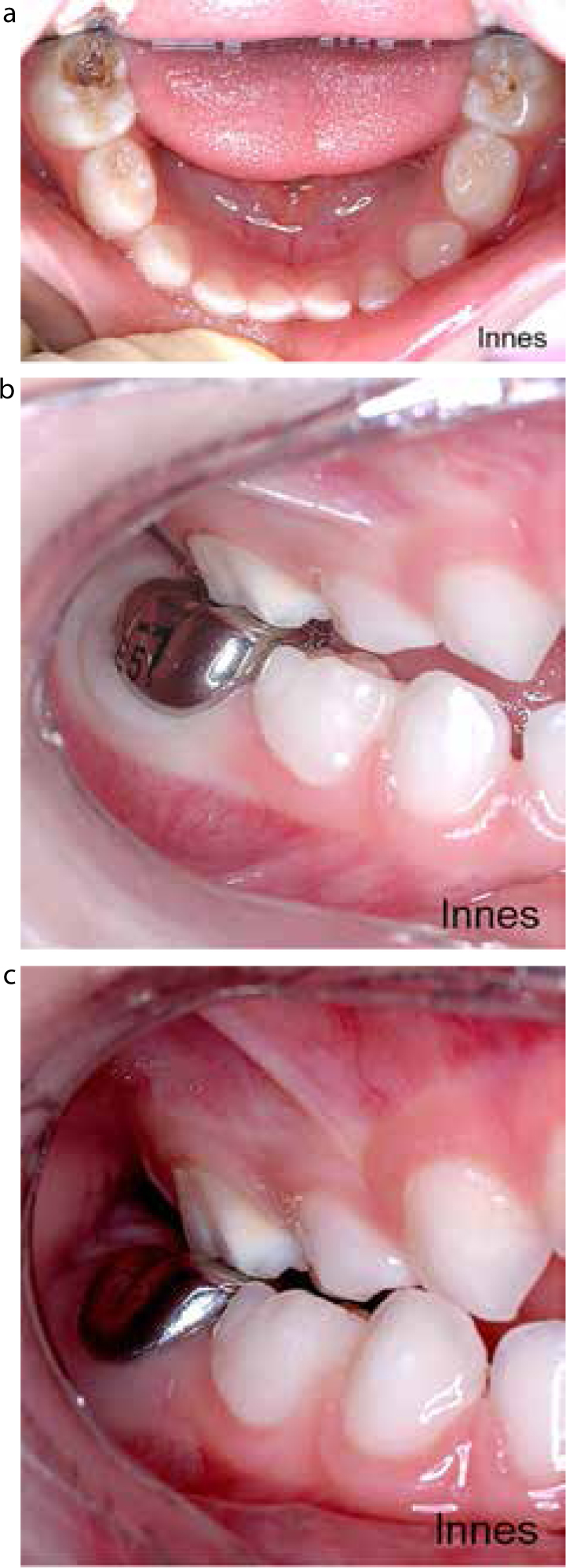
Figure 7 (a–c) shows an alternative management for such lesions in deciduous teeth, the Hall crown. These crowns break all the conventional rules in that no caries is removed. An appropriate size of stainless steel crown is selected and cemented onto the carious tooth with no preparation and no local anaesthetic required. No infected dentine is removed, indeed, it is sealed in the tooth, and leaving infected dentine is of no consequence. Clinical trials carried out in general practice showed these crowns were more successful than glass ionomer restorations with conventional dentine caries removal and the ‘little patients’ preferred the crown technique to the intracoronal restoration.
Figure 7. The Hall crown. (a) Before cementation; no caries removal and no occlusal or proximal reduction. (b) The crown directly after cementation. Inevitably the bite is ‘high’. (c) Six weeks later. The bite has nearly re-established.
In Figures 8 and 9 there are large occlusal lesions in permanent teeth. In Figure 8 there is a cavity but there is also overhanging enamel and the biofilm on the dentine surface is largely protected from disturbance by the toothbrush. The lesion is actively progressing and cleaning alone will not solve this problem; a restoration is required to aid biofilm control and restore the tooth. Just as in the deciduous dentition, opening the lesion to allow cleaning would also lead to lesion arrest. In Figure 9, the lesion was originally active and of similar size but overhanging enamel has fractured away and this lesion is now cleansable. It is now arrested, clean, hard and stained.
Figure 8. Active caries lesion with large cavity extending deep into dentine.Figure 9. Arrested occlusal caries lesion. The partly undermined enamel margins have been fractured and abraded away by mastication. The biofilm in the cavity is removed because the tooth is in functional occlusion. The dark brown dentine is hard and painless.
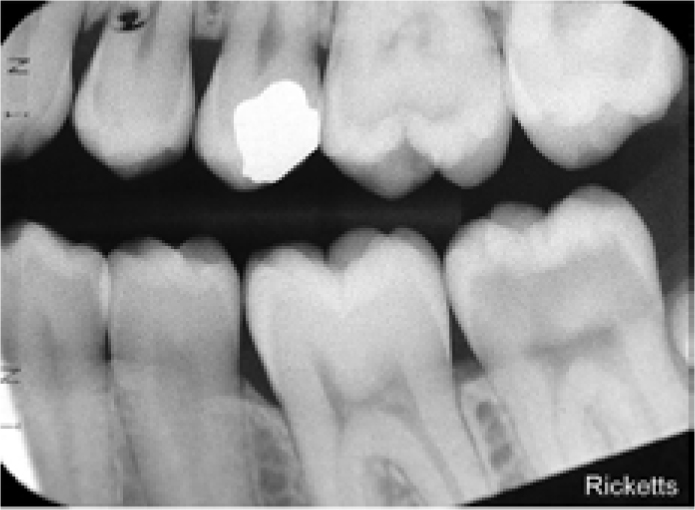
Figure 10 is a radiograph of the deep clinical lesion in Figure 8. The lesion is approaching the pulp but this tooth is symptomless and vital and there is every chance that the pulp can be preserved. In past years the restorative approach would have been to excavate the soft dentine thoroughly prior to tooth restoration, the aim being to remove all the infected dentine. However, this ‘complete excavation’ would be very unwise and would prejudice the pulp as it might expose the pulp and require root canal treatment. As we have already seen, the infected dentine is of no clinical consequence as far as arresting the lesion is concerned and thus complete excavation seems careless to the point of being unethical. A sensible pulp-protecting technique practised for many years is called ‘indirect pulp capping’, where a tiny amount of soft dentine is left over the pulp to avoid exposure. The difficulty is to know where to stop excavation as the distance to the pulp is unknown. Perhaps much more demineralized soft dentine could be left without compromising pulp vitality, so called ‘partial caries removal’.
Figure 10. Radiograph of the deep occlusal caries lesion seen clinically in Figure 8.
A number of randomized clinical trials, on both deciduous and permanent teeth, have compared partial and complete caries removal in deep dentinal lesions in symptomless, vital teeth.5 By ‘deep dentinal lesion’ the operator considers the pulp may be exposed by prolonged excavation. Some 20–50% of completely excavated deep dentinal lesions are likely to experience pulp exposure, while hardly any of those with partial caries removal show exposure. Some of these studies have used the so-called stepwise excavation technique in the partial caries removal group. In this technique, after partial removal of infected dentine corresponding to the deepest part of the lesion, lesions with clean margins are sealed and then re-opened after a number of weeks or months. Excavation is then continued until hard/firm dentine is reached. The logic of this biological approach is to arrest lesion progression by depriving bacteria of nutrients and allowing time for the defence reactions of tubular mineralization and tertiary dentine formation before completing excavation. These studies have yielded some fascinating results:
On re-entry, the dentine has totally changed. Where there was oozing moisture, soft and pale yellow dentine prior to the first restoration, it is now hard but sometimes crumbly, dry and dark brown in colour (Figure 11a, b).
Re-entry to complete excavation exposed the pulp in some 8–17% of the teeth and, since these teeth were symptomless and vital prior to re-entry, one wonders if this second excavation was either necessary or wise.
In many studies, the infected dentine was sampled before the first restoration and then again on re-entry. The microbiology was dramatically changed. There were fewer micro-organisms and those that remained did not belong to the highly aciduric flora. This is exactly what would be predicted according to the ecological plaque hypothesis. Sealing the cavity has changed the environment. The defence mechanisms of tubular mineralization and tertiary dentine have reduced the permeability of the dentine. The micro-organisms are now stressed, cut off from the mouth by the seal of the restoration and also cut off from nutrients coming up through the dentinal tubules by the defence reactions. The starved micro-organisms adapt to the new environment.
Figure 11.
(a) Clinical picture of partial excavation of a deep lesion. The dentine is soft and wet. The tooth is now restored to give a good cavity seal. (b) After a few months the tooth is reopened. Notice that the dentine is now dark brown and no longer wet. When scraped with an excavator, this dentine is hard but the surface can be removed provided the dentist uses a sharp excavator firmly. This lesion is seen clinically in Figure 8 and radiographically in Figure 10.
What should we excavate and how?
From the discussion above the answer may be nothing (non-operative cavity treatment, Hall crown) or partial caries removal. In a deep dentinal lesion and a symptomless, vital tooth the excavation should never aim to scrape hard squeaky dentine; this so-called ‘complete caries removal’ invites pulp exposure. When restoring a tooth with a conventional filling, the clinical aims of excavation should be:
Avoid exposure. Do not attempt to excavate to hard tissue in deep dentine lesions. There is no need to remove all of the infected dentine prior to placing the restoration. You do not know where the pulp is and there is no need to risk exposure.
Always produce a sound cavity margin for bonding. Cavity seal is very important to pulpal health and microbiological control.
Use a hand excavator rather than conventional bur close to the pulp! Tactile feel is difficult when using a bur, even at low speed.
Excavation is conveniently carried out with excavators, although some dentists use round carbon steel or tungsten-carbide burs at low speed. Some ‘smart’ techniques have been designed to remove only infected dentine, leaving affected dentine behind.7 These include the use of plastic burs, and fluoresce-aided caries excavation (FACE) techniques, sono-abrasion and air abrasion. However, since the level of infection is irrelevant, these are not required. Caries disclosing dyes are notoriously contra-indicated. Originally designed to stain infected dentine, they encourage overcutting of tissue that should not be removed.
Chemo-mechanical excavation techniques using either sodium hypochlorite-based or pepsin-based agents, used with instruments gently to abrade the cavity floor, were designed to dissolve denatured collagen selectively, removing heavily infected dentine at the base of the cavity. These techniques are very gentle as far as the patient is concerned. There is no vibration as with a conventional bur and no feeling of pressure as is felt when an excavator is used. For those dentists treating very nervous patients, these methods may still be helpful, even when removing less dentine than was originally intended.
Conclusions
Dentine becomes infected with commensal micro-organisms as a result of caries lesion formation on root surfaces and when lesions progress following cavitation of enamel lesions. However, this infection is unimportant because the driving force for lesion development and progression is the overlying biofilm. This explains why root surface caries can be controlled by mechanical plaque control using fluoride toothpaste, and restorations are not needed to arrest these lesions.
Similarly, the infected dentine in cavitated enamel lesions does not have to be removed to arrest the lesion. If the lesion is either opened for cleaning by the patient or parent, the lesion can be arrested. Sealing of infected dentine within the tooth, either by a Hall crown or by partial caries removal prior to placing a well-sealed filling, will also arrest the lesion. When restoring deep lesions in symptomless, vital teeth, vigorous excavation of infected dentine is likely to expose the pulp and make root canal treatment necessary. This ‘complete excavation’ is not needed and should be avoided.