Quality guidelines for endodontic treatment: consensus report of the European Society of Endodontology. Int Endod J. 2006; 39:921-930
Friedman S, Mor C. The success of endodontic therapy − healing and functionality. J Calif Dent Assoc. 2004; 32:493-503
Ng Y, Gulabivala K, Mann V. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 1 perapical health. Int Endod J. 2011; 44:583-609
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of non-surgical root canal treatment: part 2: tooth survival. Int Endod J. 2011; 44:610-625
Pjetursson BE, Bragger U, Lang NP Comparison of survival and complication rates of tooth supported fixed dental prostheses (FDPs) and implant supported FDPs and single crowns (SCs). Clin Oral Implants Res. 2007; 18:97-113
Torabinajad M, Anderson P, Bader J Outcome of root canal treatment and restoration, implant-supported single crowns, fixed partial dentures and extraction without replacement: a systematic review. J Prosthet Dent. 2007; 98:285-311
Farzaneh M, Abitbol S, Friedman S. Treatment outcome in endodontics: the Toronto study. Phases I and II: Orthograde retreatment. J Endod. 2004; 30:627-633
Ng YL, Mann V, Rahbaran S Outcome of primary root canal treatment: systematic review of the literature. Part 1. Effects of study characteristics on probability of success. Int Endod J. 2007; 40:921-939
Sjögren U, Hägglund B, Sundqvist G Factors affecting the long-term results of endodontic treatment. J Endod. 1990; 16:498-504
Lofthag-Hansen S, Huumonen S, Gröndahl K Limited cone-beam CT and intraoral radiography for the diagnosis of periapical pathology. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:(1)114-119
Kayser A. Shortened dental arches and oral function. J Oral Rehabil. 1981; 8:457-462
Witter D, van Palenstein Heldman W, Creugers N The shortened dental arch concept and its implications for oral health care. Community Dent Oral Epidemiol. 1999; 4:249-258
Graham R, Mihaylov S, Jepson N Determining ‘need’ for a Removable Partial Denture: a qualitative study of factors that influence dentist provision and patient use. Br Dent J. 2006; 200:155-158
Jepson N, Thomason J, Steele J. The influence of denture design on patient acceptance of partial dentures. Br Dent J. 1995; 178:296-300
Thomason J, Moynihan P, Steen N Time to survival for the restoration of the shortened lower dental arch. J Dent Res. 2007; 86:646-650
Jepson N, Allen P. Short and sticky options in the treatment of the partially dentate patient. Br Dent J. 1999; 187:646-652
Djemal S, Setchell D, King P Long-term survival characteristics of 832 resin-retained bridges and splints provided in a post-graduate teaching hospital between 1978 and 1993. J Oral Rehabil. 1999; 26:302-320
Chang H, Zidan O, Lee I Resin-bonded fixed partial dentures: a recall study. J Prosthet Dent. 1991; 65:778-781
Edelhoff D, Sorensen JA. Tooth structure removal associated with various preparation designs for anterior teeth. J Prosthet Dent. 2002; 87:503-509
Saunders W, Saunders E. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:(3)137-140
Zarb G, Schmitt A. The longitudinal clinical effectiveness of osseointegrated dental implants: the Toronto study. Part III: Problems and complications encountered. J Prosthet Dent. 1990; 64:(2)185-194
Pennington M, Vernazza C, Shackley P Evaluation of the cost-effectiveness of root canal treatment using conventional approaches versus replacement with an implant. Int Endod J. 2009; 42:(10)874-883
Modern endodontic planning part 1: assessing complexity and predicting success Sarra Jawad Carly Taylor Reza Vahid Roudsari James Darcey Alison Qualtrough Dental Update 2024 42:7, 707-709.
Authors
SarraJawad
BDS, BSc, MFDS
Specialty Registrar/Honorary Clinical Lecturer in Restorative Dentistry, University Dental Hospital of Manchester
Following a diagnosis of irreversible pulpal disease, periapical disease or failed endodontic therapy, the options for the tooth are extraction or root canal treatment. There is increasing evidence that certain factors may allow the clinician to predict the likely outcome of root canal therapy (RCT) and thus better inform the patient of the possible success rates. Should the patient choose root canal treatment, the clinician must also be able to gauge the potential difficulties that may be encountered and consequently determine whether it is within their competency.
CPD/Clinical Relevance: Assessing outcomes and complexity of care is an essential part of informed consent. Knowing when to refer is an essential component of best clinical practice.
Article
The primary goal of endodontics is to preserve the health of the pulp. When the pulp is irreversibly damaged, the goal is to prevent infection and periapical disease. When there is bacterial contamination of the root canal system, the clinician must be aware that success is more intimately tied to the decontamination of the root canal system. The intricate anatomy of the root canal system, the challenging oral environment and a plethora of patient factors can present challenges to achieving these goals. There are a multitude of reasons as to why root canal treatment may be difficult to achieve or more likely to fail. This ability to predict outcomes is critical to the decision to treat. All clinicians must be able to assess the prognosis of endodontic treatment, make a sensible decision about its complexity and decide whether it is within their capabilities if they are to obtain informed consent.
Assessing prognosis
Dentists are often asked by patients, ‘Will it work?’ and it falls to the dentist to give an indication as to the projected success rate of their treatment. The definition of success has been a topic of much debate in the endodontic literature in recent years. The European Society of Endodontology definition of success is (Figure 1):1
Figure 1. Success following endodontic retreatment: intact lamina dura and an absence of symptoms: (a) pre-treatment and (b) after 18 months.
An intact lamina dura;
Normal periodontal ligament space;
The absence of clinical signs and symptoms of disease;
No loss of function.
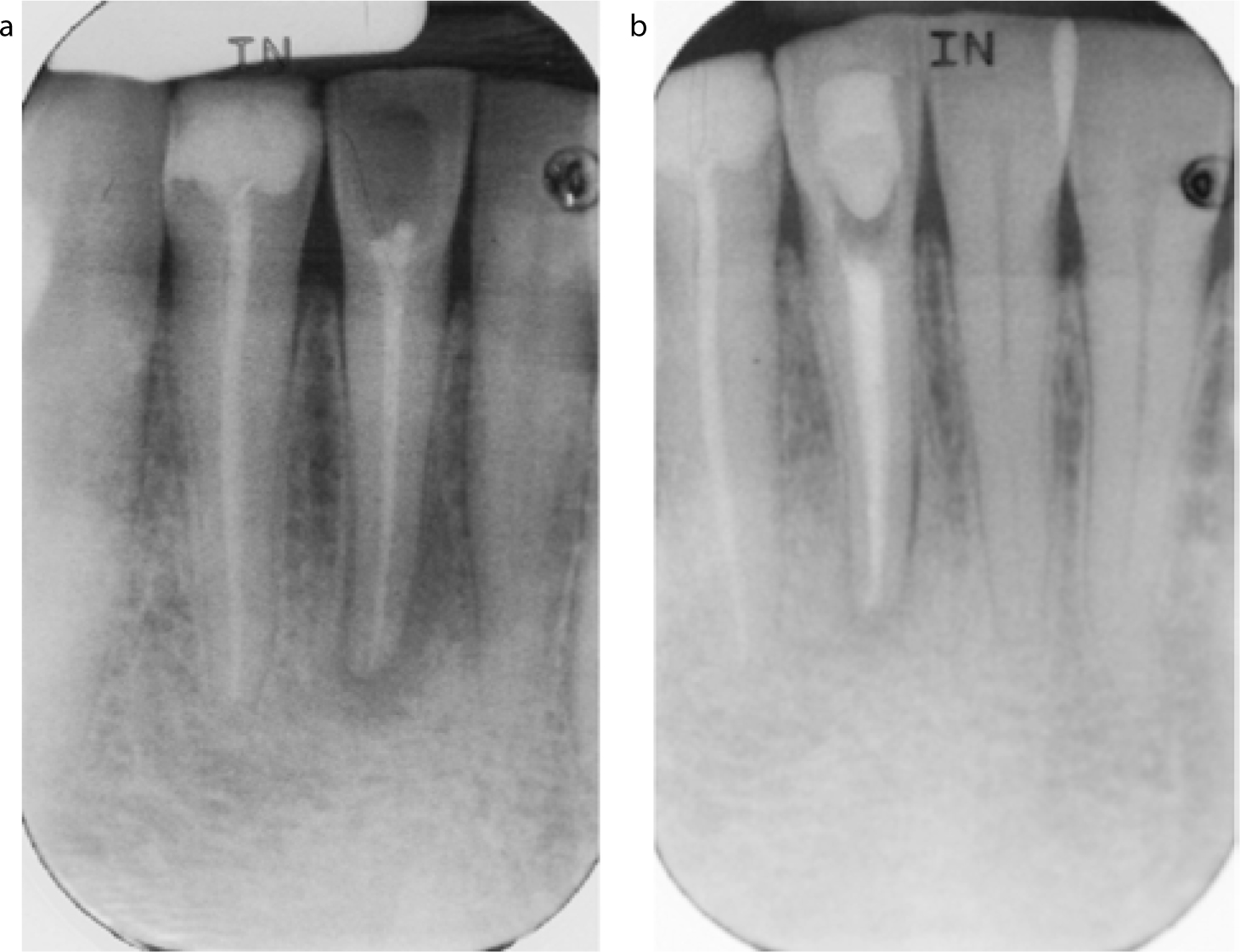
Survival indicates that the tooth is still present (Figure 2), although there is:
Figure 2. Survival following endodontic treatment of (a) LR1. In (b) the periapical lesion remains but has reduced in size after 6 months. There is an absence of symptoms. Surely this functional tooth has a successful outcome?
Radiographic evidence of peri-apical disease which may still be the same or slightly diminished;
Figure 3.
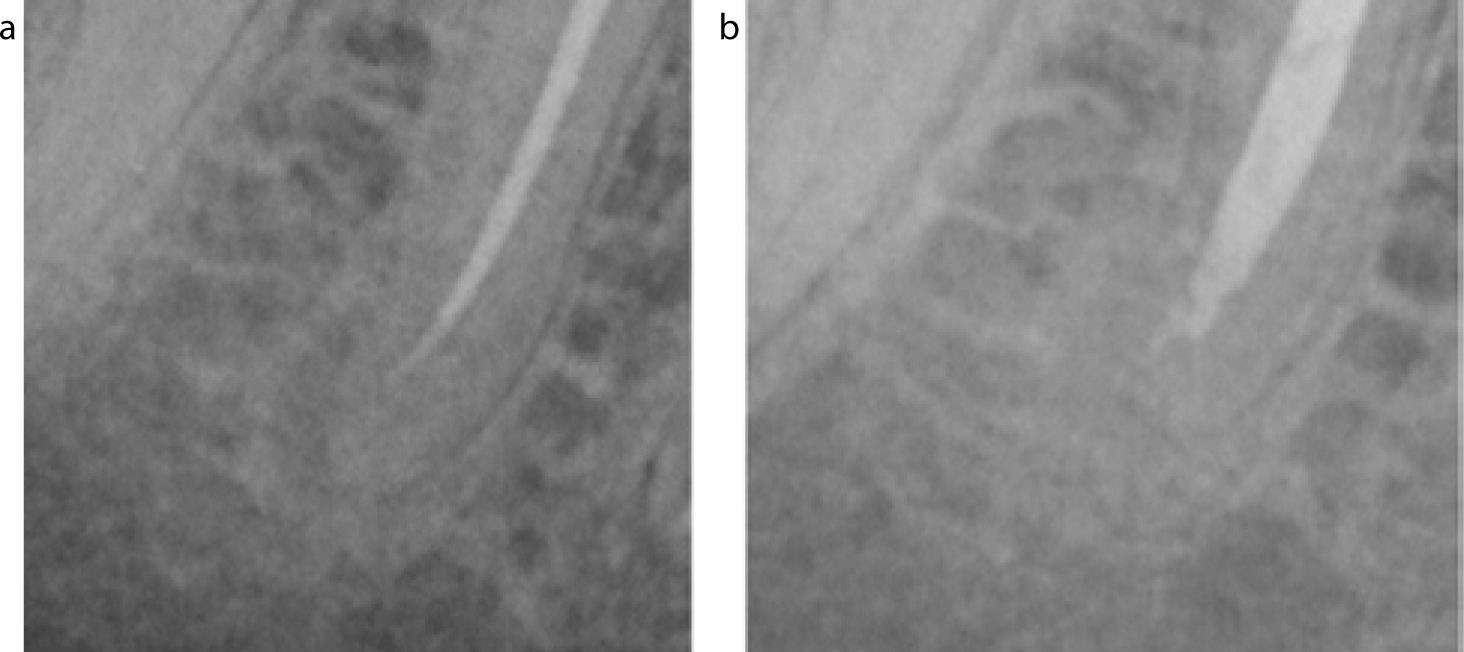
(a, b) Failure following endodontic treatment. The lesion has increased in size.
Persistent or enlarging periapical disease;
Signs and symptoms associated with the tooth;
Continuing resorption.
A tooth is said to be functional when there are no clinical signs or symptoms irrespective of whether there is radiographic evidence of disease.2 Functionality may be a more relevant indicator of success: if the tooth is pain free and functional, then this could be considered a successful outcome. This becomes important when comparing endodontic treatment with the provision of dental implants, a potential treatment alternative in certain cases and often reported in terms of survival figures. The success of endodontic treatment has been estimated at 83% for primary treatment and 80% for retreatment.3,4 The survival figures from the same study demonstrated 95.4% of primary treatments and 95.3% of retreatments were surviving after 4 years. It is clear that both success and survival rates equal, if not surpass, those of tooth-supported bridges and implant-based solutions (Table 1).5 Furthermore, both endodontic- and implant-based treatment is associated with higher survival and improved psychosocial outcomes over extraction and replacement with fixed bridgework.6 Interestingly, success rates for endodontic treatment have not dramatically changed over the last five decades, despite significant technological advances.7,8 This may be in part due to the increased complexity of cases being undertaken.
Survival @ 5 years
Success @ 5 years
Single tooth implants
94.5%
61.3%
Adhesive cantilever bridges
87.7%
not reported
Conventional cantilever bridges
93.8%
not reported
Ng et al demonstrated that eleven factors were shown to influence the success of both primary and endodontic re-treatment when using strict assessment criteria (Table 2).3 Other longitudinal studies have found that the pre-operative pulpal status and the presence of apical periodontitis also influence treatment success.7,9 Many of these factors can be assessed at examination and factored into discussions considering treatment options and prognoses, thus assisting decision-making. Furthermore, it is clear that the prognosis of endodontic therapy may change as treatment progresses (lack of patency, creation of a perforation, etc) and such information can be a useful tool for both clinician and patient. The presence of periapical pathology post-treatment does not equate to failure and dentists should reassure patients that the healing may be prolonged. Bony healing may take longer where larger lesions are present, therefore it is important to have serial comparative intra-oral radiographs, over an extended time period, before a decision may be made as to whether treatment is successful or has failed.
Pre-operative Factors
Effect on Odds of Treatment Success
Presence of a peri-apical lesion
Reduced success by 49%
Size of the peri-apical lesion
Every 1 mm increase in size reduced success by 14%
Presence of a sinus
Reduced success by 48%
Presence of a perforation
Reduced success by 56%
Intra-operative Factors
Achieving canal patency
Doubled the chance of success
Apical extent of root canal instrumentation
12% reduction in success for every mm which was not instrumented
Over extended root filling
Reduced success by 62%
Irrigation with chlorhexidine and sodium hypochlorite
Reduced success by 53%
Irrigation with EDTA and sodium hypochlorite (increased success for secondary RCT only)
Doubled re-treatment success
Associated pain or swelling between visits
Reduced success by 47%
Post-operative Factors
High quality coronal seal
11 times greater success irrespective of restoration type
Assessing complexity
There are several factors to be considered as to whether RCT should be undertaken and the level of difficulty involved. These should be used objectively to:
Make a judgement upon whether the proposed treatment is within the capabilities and training of the clinician.
To ensure that consent prior to commencement is robust and informed, that patient expectations are managed and that a referral for treatment or advice is considered if appropriate.
Essential considerations include:
Diagnostic prerequisites;
Patient factors;
Mouth factors;
Tooth factors;
Root factors;
Operator factors.
Diagnostic prerequisites
It is essential to have a high quality periapical radiograph, taken using a parallelling device, as part of the diagnostic process. The radiograph must include the entire root and apical area. All practitioners should have a quality assurance programme in place to monitor the justification, diagnostic and processing quality of their radiographs. Parallax radiographs are helpful in multi-rooted teeth to differentiate anatomy. Recent developments have demonstrated that cone beam computed tomography (CBCT) may have a role in assessment of anatomy and pathology. There is evidence that CBCT has a higher diagnostic yield when assessing for periapical pathology than conventional periapical radiography.10 In addition, CBCT can help identify anatomical variations, patency, separated instruments, fractures, resorptive conditions and the quality and extent of pre-existing root canal filling.11 CBCT delivers a significantly higher radiation dose than conventional radiography and should only be used to answer specific questions that may alter the decision to treat a tooth.12 Therefore, all CBCT scans must be appropriately justified and practitioners must not view CBCT as a routine diagnostic tool for all patients.
Patient factors
Patients must be prepared to undergo lengthy and potentially expensive treatment if they wish to proceed with endodontic treatment. Multiple visits may be necessary. The management of a patient with a prominent gag reflex is potentially challenging, but the majority cope well once a rubber dam, isolating the mouth from instruments and medicaments, has been applied. Anxious/phobic patients may require adjunctive sedation. This service may not be readily available, especially for lengthy or complex procedures. Dentists should be honest about the clear difficulties which these patients present and consider extractions if the teeth are not of strategic significance or an appropriate referral.
There are very few medical conditions which contra-indicate endodontic therapy. It has been suggested that a patient with an ASA status 3 (Table 3) or greater should not be treated in general practice. Often it is not the patient's medical but physical condition that may preclude RCT, such as a difficulty in lying flat (for long periods), or involuntary muscular movements. Patients with significant learning difficulties may not be able to consent to treatment and, in these instances, a best interests decision should be made with the input of their next of kin or an independent mental capacity advocate.
ASA I
Healthy
ASA II
Mild systemic disease
ASA III
Serious, non-incapacitating disease
ASA IV
Life-threatening disease
ASA V
Dying, likely to die, within 24 hours
There are a number of circumstances in which root canal treatment is preferable to extraction. These may include patients with a history of head and neck radiotherapy, the use of bisphosphonates or patients with coagulation defects (Figure 4). For many of these patients multidisciplinary care is required and this is most often achieved in a secondary or tertiary centre but this is not a reflection on the complexity of the root canal treatment per se but a management issue. With good support from a local consultant, practitioners can treat these cases in practice.
Figure 4. This patient has Huntington's disease, has been treated with warfarin, has been on IV bisphosphonates for >3 years and takes steroids. Despite the advanced dental disease, root canal treatment is probably the first line intervention before extractions should be considered.
Mouth factors
The need for endodontic treatment must be placed in the context of the patient's oral disease status and general oral health. Complex care should be deferred if there is active caries and periodontal disease (Figure 5). When teeth are painful and the pulp irreversibly damaged this must be addressed by extirpation and dressing a tooth or extraction. Practitioners should not prescribe antibiotics unless there is evidence of systemic involvement (fever/malaise) and/or enlarging facial swelling that has not been controlled with local measures (RCT/extraction) alone.
Figure 5. This patient has no control of primary disease: there is widespread caries and chronic periodontitis. It would be sensible to defer endodontic treatment until there is disease control through improved home care and lifestyle changes.
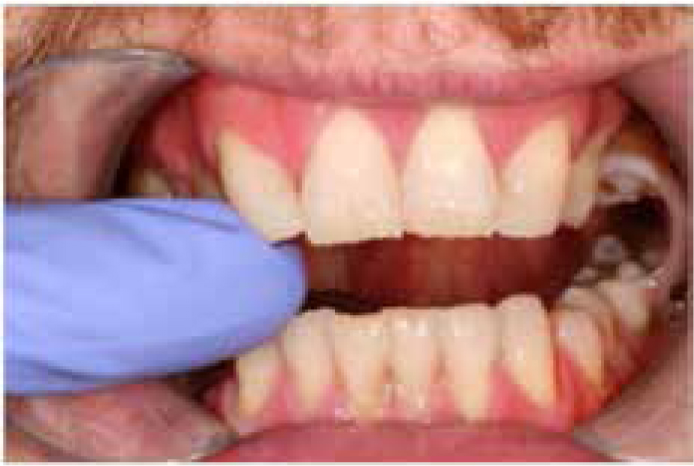
Limited opening, poor access to affected teeth and an inability to place rubber dam all add to the potential difficulties of providing treatment (Figure 6). Mouth props may help, but if rubber dam cannot be placed this must be regarded as a contra-indication to endodontic treatment.
Figure 6. Following radiotherapy, trismus can prevent any significant dental treatment. Root canal treatment is clearly impossible for this patient.
Tooth factors
Diagnostic complexity
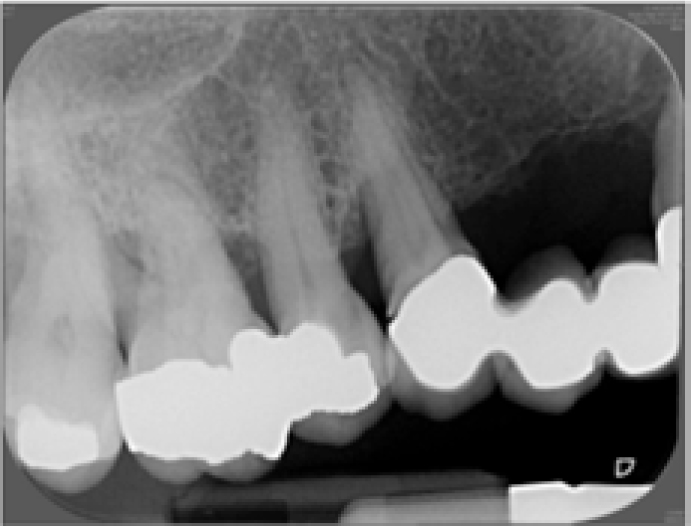
Irreversible pulpal disease in a heavily restored dentition can make identification of the offending tooth difficult (Figure 7). Following the appropriate diagnostic tests, if doubt remains as to the source of the pain, it may be prudent to offer analgesics and defer intervention. If symptoms do not correlate with dental disease, the clinician must be more cautious. Unusual pain histories, when teeth are minimally restored, if pain crosses the midline or there is a history of extractions following previous similar presentations, the clinician should be alerted that such pain may not be dental. In these cases, rather than commence RCT, a referral for a second opinion to discount non-odontogenic pain is indicated.
Figure 7. This patient presented with a dull ache to warm food emanating from the maxillary right quadrant. The heavily restored dentition reveals many teeth that could have irreversible pulpal disease: diagnosis can be very difficult.
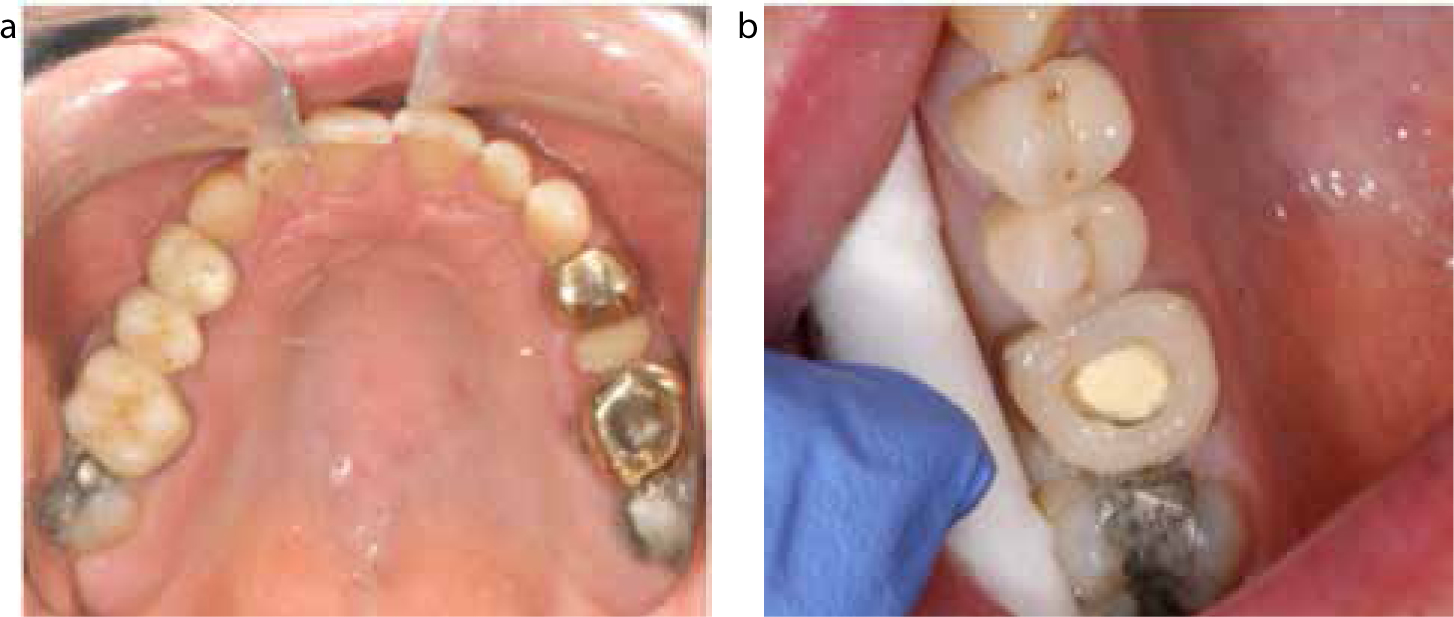
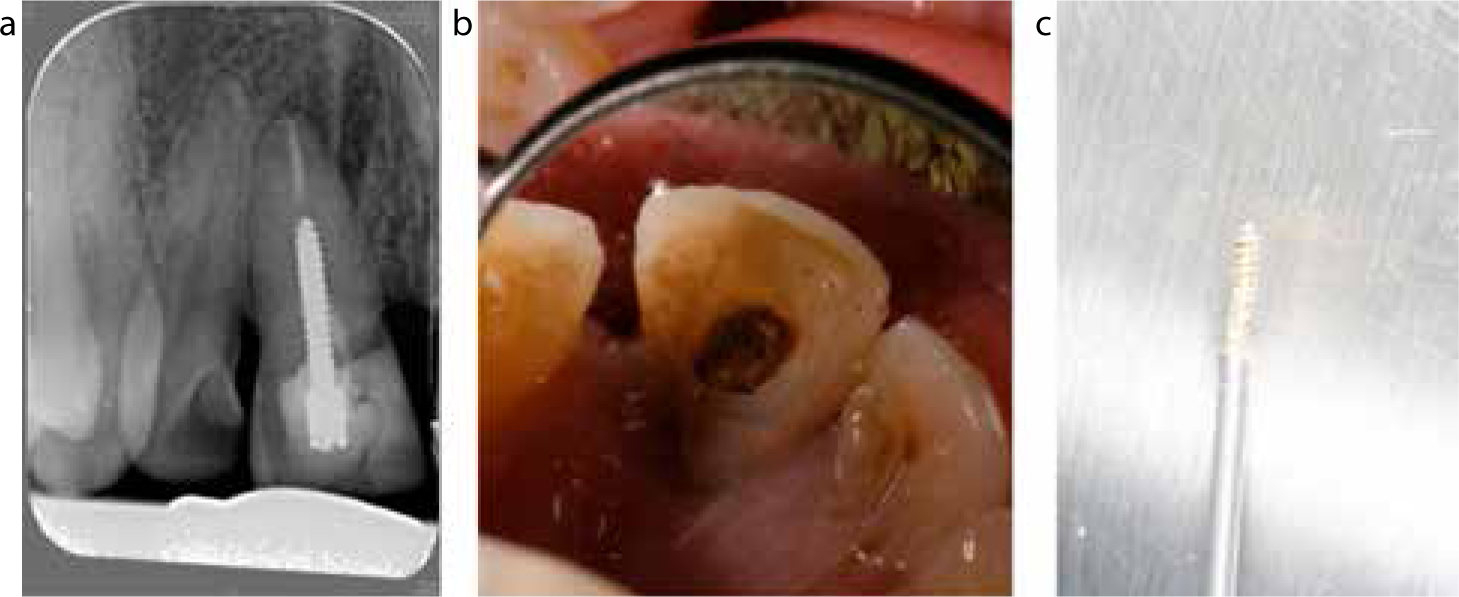
It is a prerequisite that rubber dam can be placed and this may be tried prior to treatment. If the dam margins do not form a water-tight seal, treatment may need to be abandoned unless novel approaches can be used (Figure 8). Extensive caries which is inaccessible to complete removal should be considered a contra-indication to further treatment. If there is evidence of failed coronal seal or recurrent disease, consideration must be given to the removal of crown and bridgework in advance of treatment. This also allows a more thorough inspection of the underlying tooth structure and may facilitate access to the pulp chamber and root canal system (Figure 9). Access through crowns can be difficult; there is often impaired visibility. Furthermore, loss of anatomical markers and alterations in crown-root angulation may increase the likelihood of excessive tooth removal and perforation.
Figure 8.
(a–c) Placement of a rubber dam clamp was only possible following buccal gingivectomy.Figure 9.
(a, b) Following crown removal of the UR6 there was minimal residual core. In this case a ring of composite was bonded to the root surface to permit engagement of the rubber dam clamp.
Assessment of restorability is often subjective
A tooth restorability index has been described.13 Though this remains unvalidated, it may serve as a more objective aid when assessing teeth.
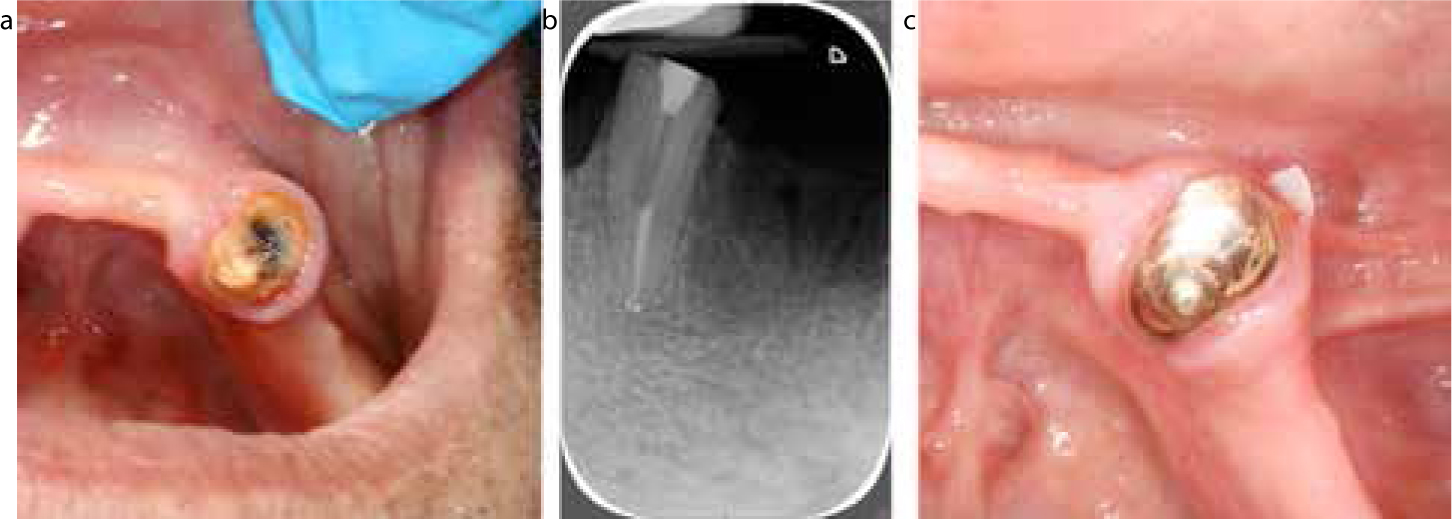
If the coronal aspect of a tooth is not restorable, and capable of being isolated with rubber dam, the root(s) may still be used as an overdenture abutment. This allows preservation of alveolar bone, tactile proprioception, increased support for prostheses and, if root surface anchors are used, an increase in the retention of prostheses (Figure 10).
Figure 10.
(a–c) The underlying core of the LR3 was heavily carious following crown removal. Endodontic treatment was performed and the root prepared for a stud-retained overdenture.
In the case of perio-endo lesions, all diagnoses with a primary periodontal disease origin carry an uncertain prognosis. It is imperative that endodontic therapy is undertaken parallel with periodontal treatment if outcomes are to be improved in teeth that have perio-endo lesions.
Root factors
If a root canal shows no evidence of radiographic patency this may increase the complexity, but many canals that appear sclerosed on a radiograph are not always sclerosed clinically14 (Figure 11). It is important to attempt orthograde treatment first but inform the patient that surgical treatment or an extraction may be the only solution should access prove futile. Access to the root canal can be difficult, especially when extensive cores have been placed or posts used (Figure 12). Techniques for accessing sclerosed canals are described later in this series.
Figure 11.
(a, b) Despite the radiographic appearance of canal sclerosis and a failed attempt by a previous dentist to access this tooth, the canal was patent and instrumented. Radiographs can be deceiving.Figure 12.
(a–c) Posts present a common impediment to accessing the canal system though invariably they can be removed with little damage to the tooth or risk of fracture.
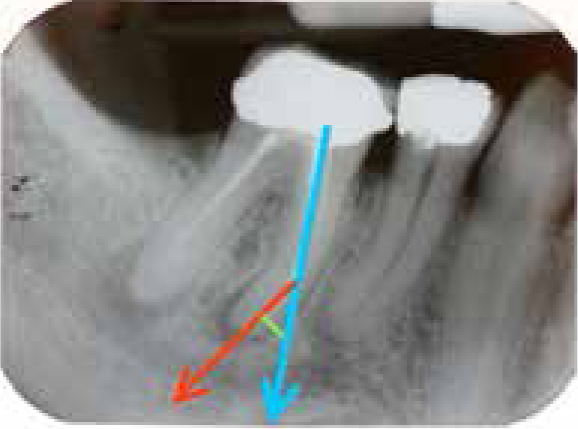
With increased curvature comes an increased likelihood of iatrogenic damage, canal shortening, instrument fracture and inadequate cleaning and shaping. The basic curvature of the root can be calculated on an undistorted periapical radiograph by the intersection of a line passing through the long axis of the tooth and a line connecting the long axis and apical position (Figure 13). Double curves present even more difficulty (Figure 14). Complexity is also increased where complex root canal anatomy is evident, such as C-shaped canals and internal resorption.
Figure 13. The angulation of the root is calculated by the intersection of a line passing through the long axis of the tooth (blue) and a line connecting the long axis and apical position (red). In this example the angulation is about 30°.Figure 14.
(a, b) Teeth with double curves are clearly much more difficult to assess and treat. By not respecting the curves and using instruments that are too large the canal curvature can be destroyed, resulting in straightening of the canal and over preparation.
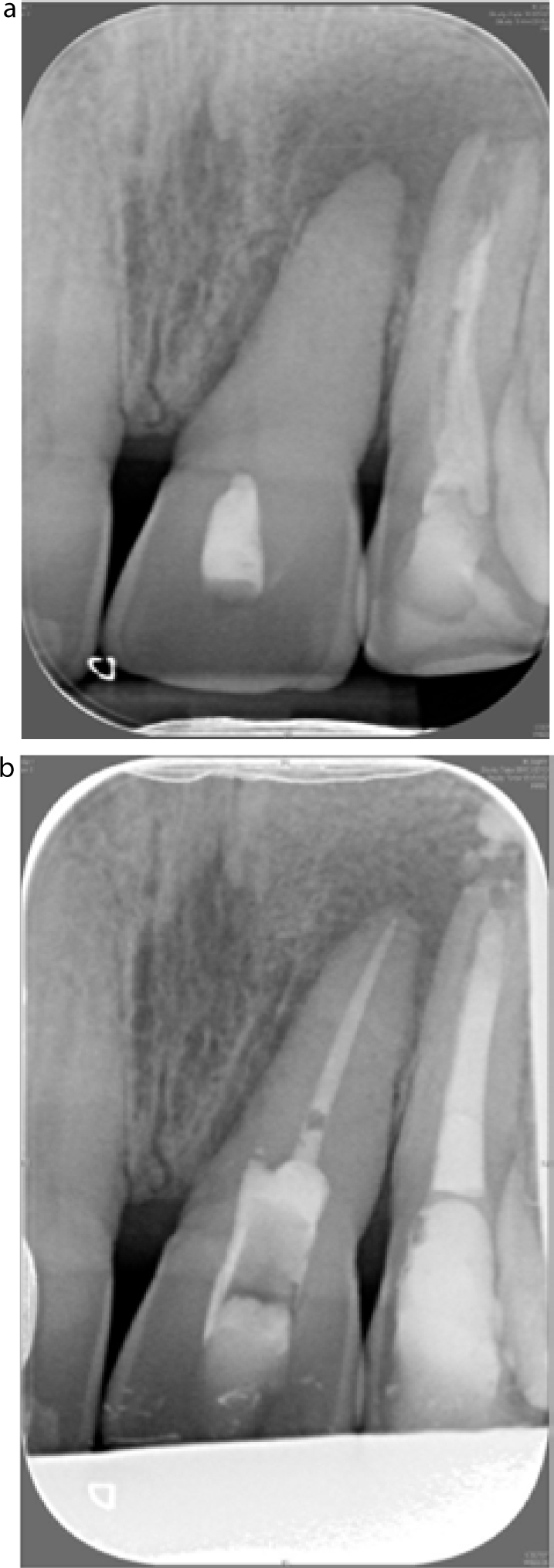
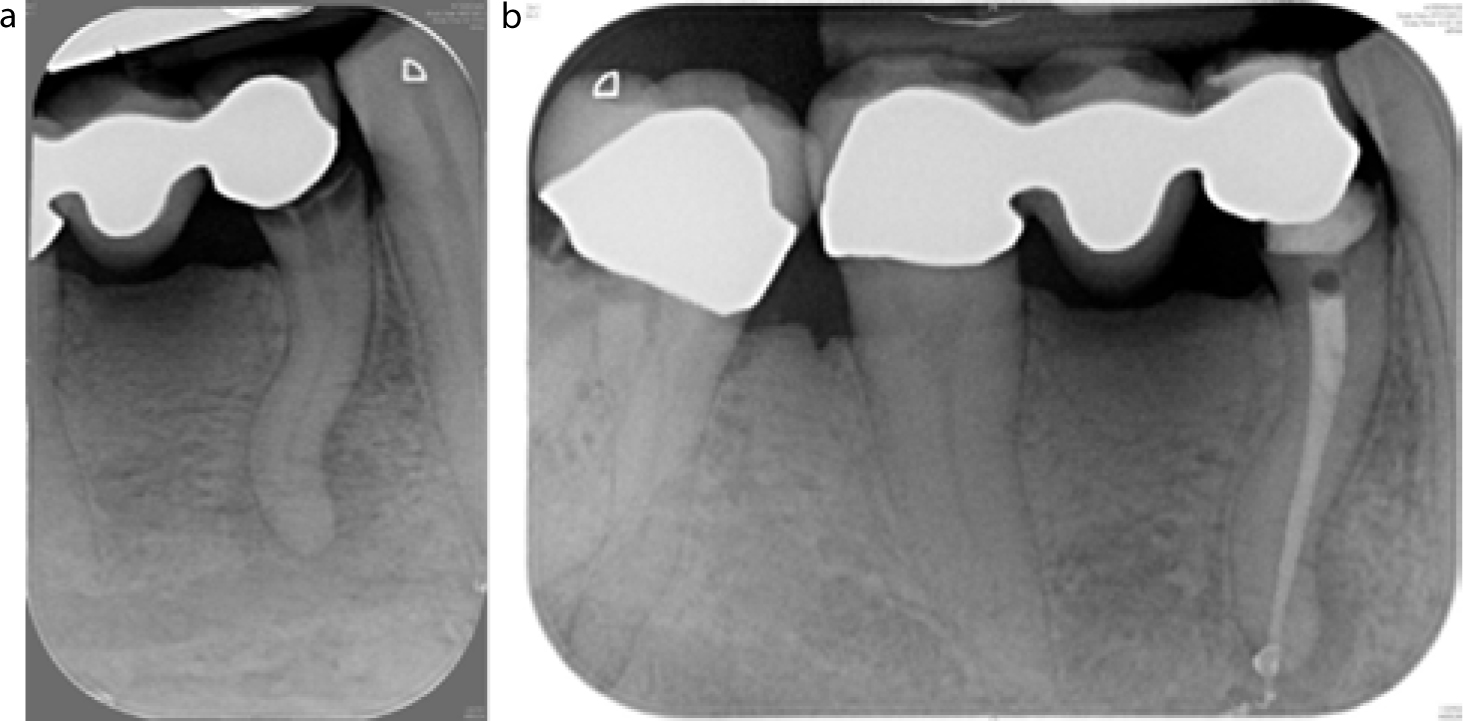
An open apex results from incomplete root formation or external inflammatory resorption of the apex. This may necessitate the use of alternative obturation materials and techniques not commonly practised. Where there is incomplete root development, consideration must be given to using different techniques and materials, such as mineral trioxide aggregate. These will be described in later papers (Figure 15).
Figure 15.
(a) Ordinarily, the apical constriction allows precise instrumentation and controlled obturation but figures (b, c) demonstrate the problems of external inflammatory resorption and incomplete apical development.
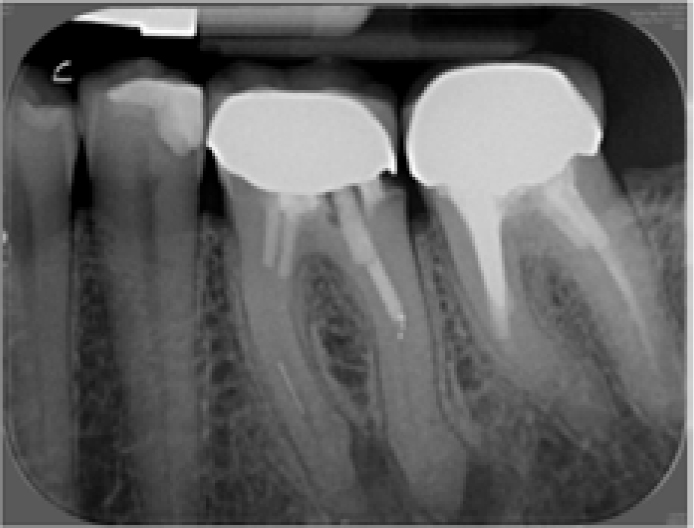
Previous RCT in a tooth invariably complicates subsequent attempts at root canal treatment. This may be due to the difficulties of removing old root canal materials and sealers or to iatrogenic deviations from the root canal system. Correction of errors of preparation, such as ledges, zipping and perforation, may be very difficult to undertake and require considerable skill and often additional equipment and materials (Figure 16). However, not all retreatments are difficult. It may be evident that primary treatment was not undertaken to a high standard with poorly compacted gutta percha and retreatment may not be challenging (Figure 17). Referral centres may reject these cases, suggesting that the primary care clinician attempts re-treatment.
Figure 16. Retreatment of LL6 and LL7 would be fraught with difficulty: separated instruments, ledging and canals with questionable patency should all alert the clinician to trouble ahead.Figure 17.
(a–c) The obturation of UL1 was so poor upon opening the canal that the two points could be removed with college tweezers, proving that not all re-treatments are the territory of the specialist. (In this case the UL2 was also root canal treated.)
The presence of fractured instruments may not preclude orthograde root and root canal re-treatment but may complicate it15 (Figure 18). As a general rule, if an instrument can be visualized, it may be possible to retrieve it. If it is beyond a curvature or in the apical portion of the tooth, retrieval may become impossible. In these instances, successfully bypassing the instrument is the only solution, but again this may not be possible. One must always consent patients to the risk of further iatrogenic damage when instrument removal is to be attempted.
Figure 18.
(a) Separated instrument tips in both mesial canals of LL6 and (b) a silver point in the mesial canal LR6. Such obstructions can present great difficulty in retreatment cases.
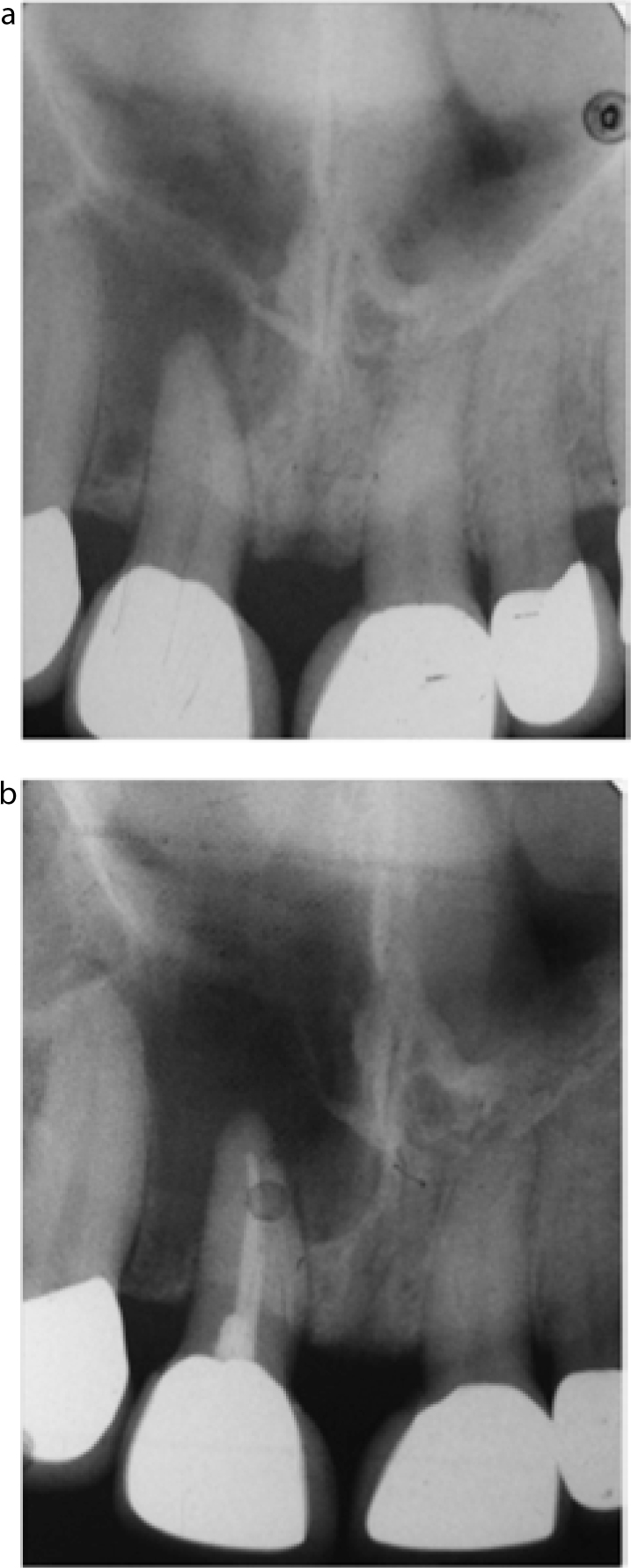
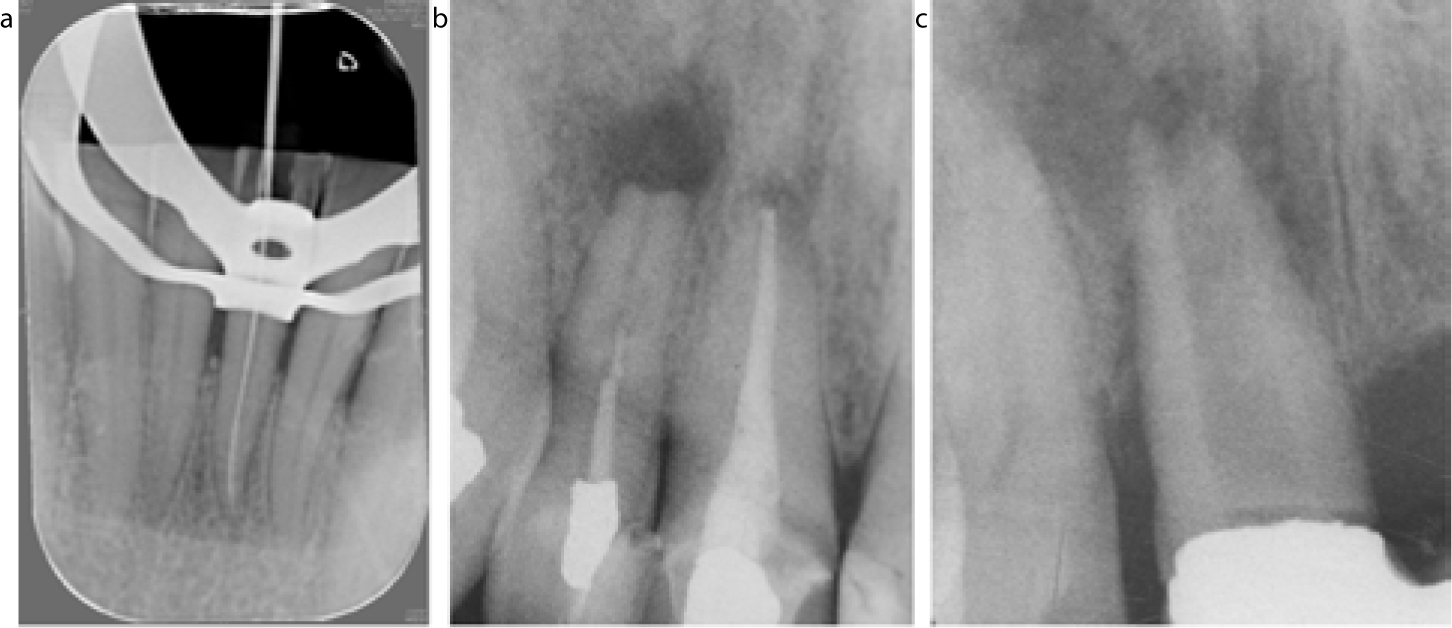
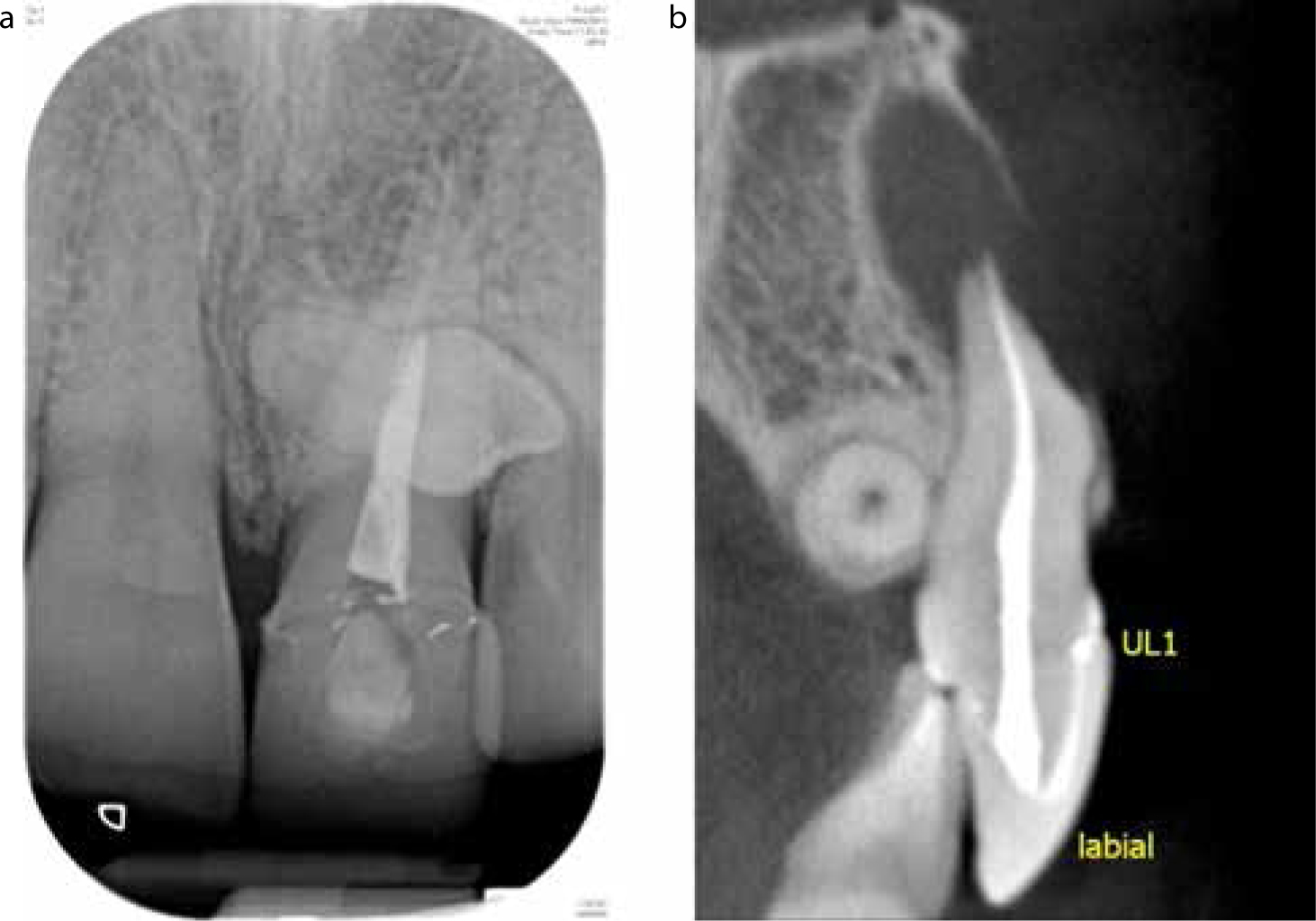
The existence of additional pathology (eg root resorption) indicates that more specialized investigations, such as CBCT, and potentially different techniques may be required (Figure 19). See Table 4 for a summary of the key factors to be considered in decision-making.
Figure 19.
(a) Is this patient's pain associated with the midline supernumerary or the poor quality root canal treatment UL1? (b) The question was answered categorically with the aid of CBCT.
Factors to Consider Before Carrying Out RCT
Patient Factors:
Lengthy appointmentsMultiple appointmentsPotentially costly treatmentAnxiety of patientMedical conditions
Mouth Factors:
Active caries or periodontal disease elsewhere in the mouthLimited mouth opening/unable to access affected teethDifficulties placing rubber dam
Tooth Factors:
Diagnosis unclearRestorability of toothPeriodontal condition
Operator training is associated with improved success.6 Thus it is essential to work within one's competency. Access to loupes, an operating microscope, and more specialized equipment and materials is best practice for more complex cases. Indeed, some would argue that these are necessary for all cases!
Endodontics – When to refer?
Clinicians with an understanding of complexity will be able to justify a referral more robustly. There are guidelines to aid the clinician in assessing complexity. The Royal College of Surgeons of England has developed a proforma for assessing complexity to be used as part of the Index of Restorative Treatment Needs.16 A summary of this can be found in Table 5. Level 1 Complexity treatment is thought to be within the skill range of the general dental practitioner. Level 3 Complexity treatment is thought to be largely within the remit of specialist practice. The Level 2 Complexity treatments lie somewhere in the middle. A list of modifying factors are included that may increase the complexity of a simple case, if present.
Surgical treatment of single canals with lesion <6 mm
1
Single/multiple negotiable root canals fully patent. >15° but <40°
Surgical treatment: single canals, no radiolucency, hemisection of mandibular molars
Teeth with incomplete root development
2
Single/multiple root canals with curvature >40°
Single/multiple root canals not considered negotiable from clinical/radiographic evidence through the entire length
Surgical treatment: single or multi-rooted teeth with radiolucency >6 mm
Teeth with iatrogenic damage or root resorption
Teeth with difficult morphology
3
Modifying Factors
Co-ordinated medical (eg renal: cardiac) and/or dental (eg oral surgery: orthodontic) multidisciplinary care
Medical history that significantly affects clinical management
Special needs for the acceptance or provision of dental treatment
Mandibular dysfunction
Atypical facial pain
Undiagnosed facial pain
Presence of a retching tendency
Limited operating access
Relevant to root canal treatment
Surgery in the proximity of important anatomical structures (eg mental foramen)
Surgery when periodontal attachment loss exceeds 3.5 mm
Medical history that significantly affects clinical management
Patients requiring IM or IV medication as a component of clinical management
Patients with a history of head/neck radiotherapy
Patients who are significantly immune-compromised or immuno-suppressed
Patients with a significant bleeding dyscrasia/disorder
Patients with a potential drug interaction
The American Association of Endodontists’ (AAE) Guidelines are also very useful.17 These categorize the difficulty of the case into minimal difficulty, moderate difficulty and high difficulty, depending on:
Patient considerations (eg medical history; ease of achieving anaesthesia; patient co-operation; mouth-opening ability; gag reflex and presence of any swelling associated with the tooth).
Diagnostic and treatment considerations (eg clarity of diagnosis; ability to take intra-oral radiographs; ease of isolation; position of the tooth in the arch (and inclination); crown morphology and its influence on potential deviation from root canal anatomy; root canal anatomy and morphology (eg curvature, length); presence of resorption).
Additional considerations (eg history of trauma; previous endodontic treatment; concurrent periodontal involvement).
The reader is referred to the easily accessible PDF of these guidelines which can be kept as an aide memoire for when to refer particular cases. Indeed, they can also be used in secondary care to assist in triaging referrals for endodontics: http://www.aae.org/uploadedfiles/dental_professionals/endodontic_case_assessment/2006casedifficultyassessmentformb_edited2010.pdf
Practitioners referring into the secondary NHS services must also be aware of local referral guidelines as these may differ, with some facilities offering minimal or no specialist endodontic services. With the development of ‘Dentists with Enhanced Skills’ it may be that more commissioning groups will fund endodontic services for complex care within the primary sector, but currently this concept is in its infancy.
Alternative treatments
Alternatives to root canal treatment must always be considered. This is of particular importance if the prognosis and/or complexity of the root canal treatment indicate that the outcome will be poor.
Leave: Doing nothing is always an option. This may even be encouraged in the case of a pathologically involved but functional tooth. Patients must be counselled upon the likelihood of future pain from such teeth.
Extraction: If a tooth is not of strategic importance, either for function or aesthetics, extraction is a viable option. A report published by the WHO suggests that 20 teeth are sufficient for a functional dentition18 and there is now established evidence that a shortened dental arch is accepted by patients.19,20 Nonetheless, it is likely that patients will wish to maintain anterior teeth. If a decision for extraction is made, the options to manage the residual space should be discussed with the patient. The space may be left unrestored, however, restorative options include provision of the following.
Removable partial denture
These are simple, cost-effective and can restore both aesthetics and function. Unfortunately, many do not get worn and there may be both psychological and physiological costs related to removable prostheses.21,22,23
Adhesive bridge
These are predictable and minimally invasive and can offer a good solution for missing teeth.24 Evidence suggests successful retention of 7+ years.25 Anterior adhesive bridges will survive longer than posterior bridges and both have more favourable outcomes than bridges replacing canines.26
Conventional bridge
These have similar, if not improved, survival rates compared to adhesive bridges, but at an increased biological cost.5 Up to 63–72% of tooth structure is removed when a tooth is prepared for a metal-ceramic restoration.27 Furthermore, 19% of such teeth may lose vitality.28 When these bridges fail, the result is more detrimental to the remaining dentition.
Single tooth implant
These offer very good survival rates at 5 and 10 years at 94.5% and 89.2%.5 The aesthetics can be excellent and destruction of abutment teeth is not required. Bone grafting may be indicated to prepare the site for placement and anatomic structures may prohibit placement. In the posterior maxilla, the presence of the maxillary sinuses often means that there is insufficient bone volume for a dental implant. In the posterior mandible, implants may only be placed if there is sufficient bone volume above the inferior dental nerve. Implants can be prohibitively expensive and patients must be consented to the cost of ongoing maintenance.29
Health economic evaluation has demonstrated that there is merit in attempting root canal treatment ahead of implant therapy.30 The condition of the remaining dentition should be assessed and any pre-exisiting disease stabilized. It is important that the clinician should not focus on the missing tooth in isolation but consider it in context with the rest of the mouth and in accordance with the general wellbeing of the patient.
Conclusion
Assessment of the tooth, roots, mouth and patient is vital prior to commencing endodontic treatment. The prognosis of the tooth in question may be predicted based on the tooth at baseline and may change through and following treatment. One must always consider alternatives to treatment: extraction with or without a prosthodontic replacement is always an option for the patient.