Via WF. Submerged deciduous molars: familial tendencies. J Am Dent Assoc. 1964; 69:127-129
Steigman S, Koyoumdjisky-Kaye E, Matrai Y. Submerged deciduous molars in preschool children: an epidemiologic survey. J Dent Res. 1973; 52:(2)322-326
Kurol J, Thilander B. Infraocclusion of primary molars and the effect on occlusal development, a longitudinal study. Eur J Orthod. 1984; 6:(1)277-293
Darling AI, Levers BG. Submerged human deciduous molars and ankylosis. Archs Oral Biol. 1973; 18:(8)1021-1040
Winter GB, Gelbier MJ, Goodman JR. Severe infra-occlusion and failed eruption of deciduous molars associated with eruptive and developmental disturbances in the permanent dentition: a report of 28 selected cases. Br J Orthod. 1997; 24:(2)149-157
Blakely D, Burden DJ, Mullally BH. Ankylosis: an orthodontic problem with a restorative solution. Br Dent J. 1995; 179:426-429
Albers DD. Ankylosis of teeth in the developing dentition. Quintessence Int. 1986; 17:(5)303-308
Brearley LJ, McKibben DH. Ankylosis of primary molar teeth. I. Prevalence and characteristics. ASDC J Dent Child. 1973; 40:(1)54-63
Messer LB, Cline JT. Ankylosed primary molars: results and treatment recommendations from an eight-year longitudinal study. Pediatr Dent. 1980; 2:(1)37-47
Altay N, Cengiz SB. Space-regaining treatment for a submerged primary molar: a case report. Int J Paediatr Dent. 2002; 12:(4)286-289
Baccetti T. A controlled study of associated dental anomalies. Angle Orthod. 1998; 68:(3)267-274
Lai PY, Seow WK. A controlled study of the association of various dental anomalies with hypodontia of permanent teeth. Pediatr Dent. 1989; 11:(4)291-296
Bjerklin K, Al-Najjar M, Kårestedt H, Andrén A. Agenesis of mandibular second premolars with retained primary molars. A longitudinal radiographic study of 99 subjects from 12 years of age to adulthood. Eur J Orthod. 2008; 30:(3)254-261
Jenkins FR, Nichol RE. Atypical retention of infraoccluded primary molars with permanent successor teeth. Eur Arch Paediatr Dent. 2008; 9:(1)51-55
Shalisha M, Peck S, Wassersteinc A, Peck L. Increased occurrence of dental anomalies associated with infraocclusion of deciduous molars. Angle Orthod. 2010; 80:(3)440-445
Williams HA, Zwemer JD, Hoyt DJ. Treating ankylosed primary teeth in adult patients: a case report. Quintessence Int. 1995; 26:(3)161-166
Infraoccluded upper deciduous second molars leading to caries in the permanent dentition Claire Rooney Imran Suida Richard James Spencer Dental Update 2024 42:5, 707-709.
Authors
ClaireRooney
BChD BSc (Hons)
Pinderfields General Hospital, Aberford Road, Wakefield, West Yorkshire WF1 4DG, UK
Infraocclusion of primary teeth is a problem that can be recognized early by the general dental practitioner. Allowing affected teeth to deteriorate beyond a point where active intervention would be recommended can make treatment of the condition more complex or may lead to unexpected sequelae. The case described in this report of infraoccluded primary teeth, suffered pathology in adjacent teeth, leading to multiple extractions and fixed orthodontic treatment post surgery. This case highlights the need for early recognition of infraocclusion by the GDP and will suggest interceptive treatment options.
CPD/Clinical Relevance: To highlight the need of interceptive orthodontics in primary care when required.
Article
Infraoccluded primary molars are a relatively common dental abnormality, however, it is rare for them to cause significant problems. This paper will discuss a case in which a patient's infraoccluded upper deciduous second molars led to associated pathology.
Background
The term dental infraocclusion refers to a tooth which ‘fails to maintain vertical height with the adjacent teeth, hence appearing to submerge below occlusal level’.1 A tooth is considered to be infraoccluded if its intact marginal ridge is greater than 0.5 mm below the intact marginal ridge of the adjacent tooth.2
The prevalence of infraocclusion has been reported to range from 1.3–38.5%.3,4 This phenomenon has been shown to affect children as young as 3 years old, although peak prevalence ranges from 8–9 years.5
At present, the aetiology is unknown, although there are a number of theories that have been suggested. The most commonly cited cause is ankylosis of the deciduous molar.6,7 Ankylosis describes the union of cementum and alveolar bone and occurs when there is a break in the continuity of the periodontal membrane and osteoclasts can act directly on the root cementum.8 Deciduous molars have the highest incidence of anklyosis, ranging from 1.5–9.9%.9 Mandibular first deciduous molars appear to be the most frequently affected, followed by the second mandibular deciduous molars.10 A review by Messer and Cline found that, when this phenomenon presents bilaterally, it tends to affect symmetrical teeth.11
It has been shown that there may be a genetic predisposition to infraocclusion. A familial tendency was recognized by Via, who reported a general incidence of 1.3%, and an incidence of 44% in their siblings when looking at a sample of the general population.3
Other suggested theories include disturbed local metabolism, gaps in the periodontal membrane, local mechanical trauma and local infection.12 Chemical or thermal irritation, local failure of bone growth, abnormal pressure from the tongue and disturbance in interaction between normal resorption and hard tissue repair have also been suggested as causes.12
Developmentally absent premolars have been associated with infraocclusion of the deciduous predecessor, along with other dental abnormalities.13 A study of 1032 patients reported 65.7% of children with missing permanent teeth had infraoccluded primary teeth compared to 1.5% of control children.14 Bjerklin et al reported, however, that 90% of healthy second deciduous molars with adequate root length and mild infraocclusion had good long-term prognosis.15
Infraocclusion of deciduous molars can have a detrimental effect on the developing dentition. Examples of this include tipping of adjacent teeth, periodontal problems and restriction of bone growth leading to alveolar ridge defects. Other consequences include space loss, delay or displacement of developing successor teeth, overeruption of teeth in the opposing arch, caries and gingival hyperplasia.16
Brearley's system is commonly used for classifying the extent of infraocclusion as follows:10
Slight – defined as the occlusal surface 1mm below the expected occlusal plane for the tooth;
Moderate – occlusal surface is approximately level with the contact point of one or both adjacent tooth surfaces;
Severe – occlusal surfaces are level with or below the interproximal gingival tissue of one or both adjacent tooth surfaces.
Severe infraocclusion only affects 2.5–8.3% of all affected deciduous molars and is specifically related to the absence of a permanent successor.17
Case presentation
MC, a 12-year-old female, presented to the Accident and Emergency department of Pinderfields Hospital with left-sided facial swelling. The patient had visited the dentist previously, where she was prescribed a five-day course of amoxicillin 500 mg and was advised to attend the hospital.
The patient complained of toothache in the upper left quadrant, starting two weeks previously and a two-day history of facial swelling. The patient was medically fit and well with no known drug allergies. She also revealed that she was an irregular dental attender.
On examination the patient was awake, alert, apyrexial and able to maintain her own airway. Mild oedema was noted around the left eye and erythema was observed at the left angle of the mandible. Intra-oral examination revealed that there was a large swelling in the upper left buccal sulcus. Despite this, the patient had good mouth-opening with minimal trismus. UL6 was tender to percussion and it was noted that ULE was severely infraoccluded.
At presentation the case had lateral open bites bilaterally, mesial tipping of the upper first permanent molars and over-eruption of the upper second molars (Figure 1). An orthopantomogram was taken and showed that both upper Es were severely infraoccluded with associated caries in UR6 and UR5 (Figure 2). After incision and drainage of the buccal space abscess under local anaesthetic, the patient was referred for a joint orthodontic/oral surgery opinion.
Figure 1.
(a–d) At presentation the case had lateral open bites bilaterally, mesial tipping of the upper first permanent molars and over-eruption of the upper second molars.Figure 2. Orthopantomogram showing infraoccluded upper second deciduous molars.
The orthodontic assessment revealed the following findings:
Mild Class III incisal relationship with lateral open bites;
Upper first permanent molars were mesially tipped, causing bilateral premature contacts; and
There was over-eruption of the upper second molars.
A periapical radiograph revealed UL6 was affected by gross caries extending into the pulp below the alveolar crest (Figure 3).
Figure 3. Periapical showing severe infracclusion in ULE and mesial caries UL6.
After discussion with the oral surgeon, the patient and her mother, a decision was made to remove UR5, URE, ULE and UL6 surgically then treat the malocclusion with fixed appliances.
Discussion
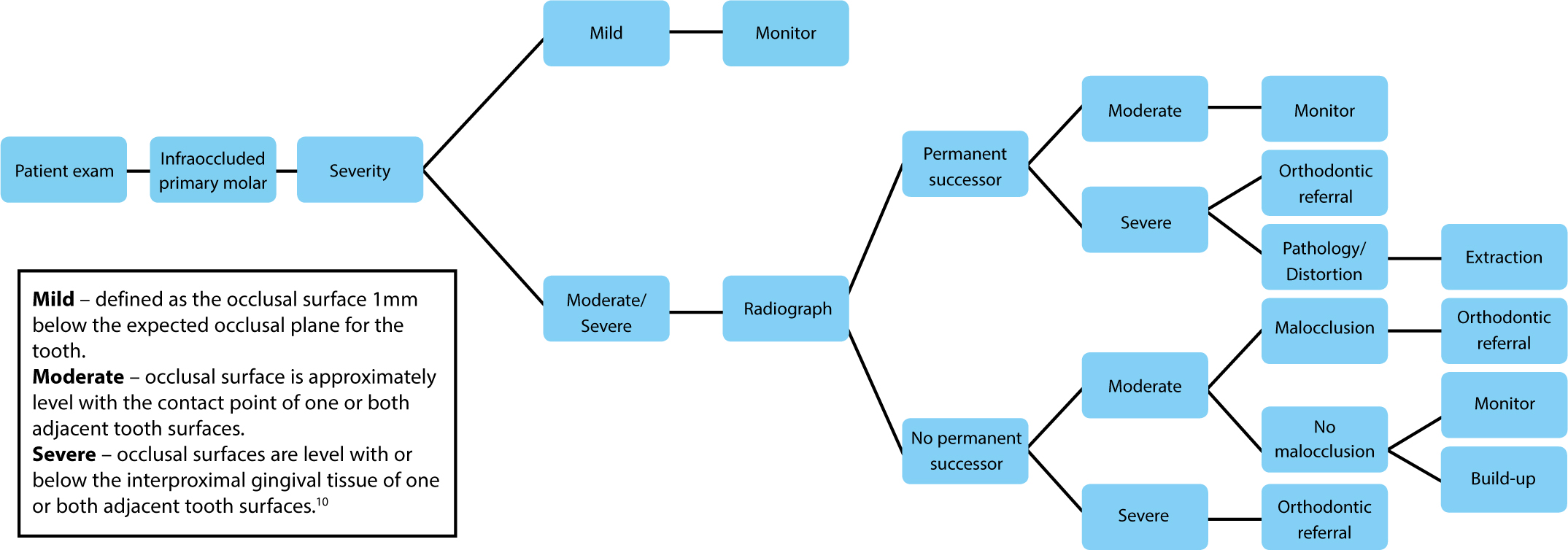
When managing the developing dentition, knowledge of normal eruption allows abnormalities to be identified early. There are many adverse outcomes if infraoccluded teeth are inappropriately managed. Figure 4 gives a timeline of how to manage infraoccluded primary molars. Treatment of these cases depends upon the degree of infraocclusion, the presence of a successor, the time of onset and the degree of tilting of adjacent teeth. The main aims of treatment should be to allow normal eruption of permanent successors and maintain alveolar ridge height so that restoration of functional units, if required, is possible.
Figure 4. How to manage infraoccluded primary molars.
Infraoccluded primary molars with absent permanent successor must be handled with care.
Extraction of the infraoccluded tooth would be indicated if there were obvious signs that this anomaly was impacting upon the health of the neighbouring dentition. Generally, the extraction would be carried out early to allow mesial drift of the first permanent molar. This phase should be carefully monitored; over-eruption of the opposing teeth can become problematic and may restrict mesial drift.
Restoration of occlusal height is another option for treating infraoccluded teeth to prevent undesirable effects occurring. This can be done by using composite resin, stainless steel crowns or cast crowns.18 Owing to progressive infraocclusion with facial growth, further intervention may be required to maintain occlusal height. For this treatment option to be viable, there must be substantial periodontal support and regular monitoring.
In cases where there is a permanent successor, there are further options, such as monitoring of infraoccluded teeth or early extraction and space maintenance.
Conclusion
As a general practitioner, one should be aware of the complications associated with long-term monitoring of infraoccluded teeth. They can have a tendency to cause problems in the developing dentition which could be avoided if interceptive orthodontics is carried out. Figure 4 shows the most reasonable options for treatment of these cases.