Merskey H, Bogduk N, 2nd edn. Seattle: IASP Press; 1994
The International Classification of Headache Disorders. 2004; 24:9-160
Okeson JP The classification of orofacial pains. Oral Maxillofac Surg Clin N Am. 2008; 20:133-144
Dworkin SF, LeResche L Research diagnostic criteria for temporomandibular disorders: review, criteria, examinations and specifications, critique. J Craniomandib Disord. 1992; 6:301-355
Hapak L, Gordon A, Locker D, Shandling M, Mock D, Tenenbaum HC Differentiation between musculoligamentous, dentoalveolar, and neurologically based craniofacial pain with a diagnostic questionnaire. J Orofac Pain. 1994; 8:(4)357-368
Woda A, Tubert-Jeannin S, Bouhassira D, Attal N, Fleiter B, Goulet JP Towards a new taxonomy of idiopathic orofacial pain. Pain. 2005; 116:396-406
Schiffman E, Ohrbach R, Truelove E, Look J, Anderson G, Goulet JP International RDC/TMD Consortium Network, International Association for Dental Research; Orofacial Pain Special Interest Group, International Association for the Study of Pain. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J Oral Facial Pain Headache. 28:(1)6-27 https://doi.org/10.11607/jop.1151
Reissmann DR, John MT, Schierz O, Wassell RW Functional and psychosocial impact related to specific temporomandibular disorder diagnoses. J Dent. 2007; 35:643-650
Locker D, Grushka M The impact of dental and facial pain. J Dent Res. 1987; 66:1414-1417
Deb S, Thomas M, Bright C Mental disorder in adults with intellectual disability. 1: Prevalence of functional psychiatric illness among a community-based population aged between 16 and 64 years. J Intellect Disabil Res. 2001; 45:(6)495-505
Renton T, Durham J, Aggarwal VR The classification and differential diagnosis of orofacial pain. Expert Rev Neurother. 2012; 12:(5)569-576 https://doi.org/10.1586/ern.12.40
Cruccu G, Anand P, Attal N, Garcia-Larrea L, Haanpää M, Jørum E, Serra J, Jensen T EFNS guidelines on neuropathic pain assessment. Eur J Neurol. 2004; 11:153-162
Dubner R Discussion on new approaches to the differential diagnosis of chronic orofacial pain. Anesth Prog. 1990; 37
Matos R, Wang K, Jensen JD, Jensen T, Neuman B, Svensson P, Arendt-Nielsen L Quantitative sensory testing in the trigeminal region: site and gender differences. J Orofac Pain. 25:(2)161-169
Madland G, Feinmann C Chronic facial pain: a multidisciplinary problem. J Neurol Neurosurg Psychiatry. 2001; 71:716-719
Sarlani E, Schwartz AH, Greenspan JD, Grace EG Facial pain as first manifestation of lung cancer: a case of lung cancer-related cluster headache and a review of the literature. J Orofac Pain. 2003; 17:(3)262-267
Dworkin RH, Turk DC, Revicki DA, Harding G, Coyne KS, Peirce-Sandner S Development and initial validation of an expanded and revised version of the Short-form McGill Pain Questionnaire (SF-MPQ-2). Pain. 144:(1–2)35-42 https://doi.org/10.1016/j.pain.2009.02.007
Baranoff J, Hanrahan SJ, Kapur D, Connor JP Validation of the Chronic Pain Acceptance Questionnaire-8 in an Australian pain clinic sample. Int J Behav Med. 21:(1)177-185 https://doi.org/10.1007/s12529-012-9278–6
Lima-Verde AC, Pozza DH, Rodrigues LL, Velly AM, Guimarães AS Cross-cultural adaptation and validation for Portuguese (Brazilian) of the pictorial representation of illness and self measure instrument in orofacial pain patients. J Orofac Pain. 27:(3)271-275 https://doi.org/10.11607/jop.1070
La Touche R, Pardo-Montero J, Gil-Martínez A, Paris-Alemany A, Angulo-Díaz-Parreño S, Suárez-Falcón JC, Lara-Lara M, Fernández-Carnero J Craniofacial pain and disability inventory (CF-PDI): development and psychometric validation of a new questionnaire. Pain Physician. 17:(1)95-108
Ravaghi V, Farrahi-Avval N, Locker D, Underwood M Validation of the Persian short version of the Oral Health Impact Profile (OHIP-14). Oral Health Prev Dent. 2010; 8:(3)229-235
dos Santos Calderon P, Peixoto RF, Gomes VM, da Mota Corrêa AS, de Alencar EN, Rossetti LM, Conti PC Concordance among different pain scales in patients with dental pain. J Orofac Pain. 26:(2)126-131
Tölle T, Dukes E, Sadosky A Patient burden of trigeminal neuralgia: results from a cross-sectional survey of health state impairment and treatment patterns in six European countries. Pain Pract. 6:(3)153-160
The Pain Catastrophizing Scale: development and validation. 1995.
Sherman JJ, Carlson CR, Wilson JF, Okeson JP, McCubbin JA Post-traumatic stress disorder among patients with orofacial pain. J Orofac Pain. 19:(4)309-317
Slade GD, Foy SP, Sugars DA The impact of third molar symptoms, pain, and swelling on oral health-related quality of life. J Oral Maxillofac Surg. 2004; 62:(9)1118-1124
Freynhagen R, Baron R, Gockel U, Tölle TR painDETECT: a new screening questionnaire to identify neuropathic components in patients with back pain. Curr Med Res Opin. 2006; 22:(10)1911-1920
Johnson JA, Coons SJ, Ergo A, Szava-Kovats G Valuation of EuroQOL (EQ-5D) health states in an adult US sample. Pharmacoeconomics. 1998; 13:(4)421-433
Yap JC, Lau J, Chen PP Validation of the Chinese Pain Catastrophizing Scale (HK-PCS) in patients with chronic pain. Pain Med. 2008; 9:(2)186-195
Thoresen S, Tambs K, Hussain A Brief measure of posttraumatic stress reactions: Impact of Event Scale-6. Soc Psychiat Epidemiol. 2010; 45:(3)405-412
Strong J, Westbury K, Smith G Treatment outcome in individuals with chronic pain: is the Pain Stages of Change Questionnaire (PSOCQ) a useful tool?. Pain. 2002; 97:(1-2)65-73 https://doi.org/10.1016/S0304-3959(01)00493–6
Pain paper 2b: classification of orofacial pain and an update on assessment and diagnosis Obi Egbuniwe Tara Renton Dental Update 2024 42:4, 707-709.
Authors
ObiEgbuniwe
BDS, MSc, PhD
Honorary Clinical Researcher, Department of Oral Surgery, King's College London Dental Institute, King's College Hospital London, Bessemer Road, London SE5 9RS, UK
Professor of Oral Surgery, King's College London; Honorary Consultant in Oral Surgery, King's College Hospital NHS Foundation Trust and Guy's and St Thomas' NHS Foundation Trust, London
The classification of chronic orofacial pain remains a contentious area. However, more recently, with the clarification of pain mechanisms and improved understanding of the underlying neurophysiology and modulation factors, there is more clarity of the possible division of pain conditions. Interestingly, the pathophysiology provides a basis for classification that has more clinical relevance. The principles of assessing and managing patients with pain have modified significantly, in line with recent improved understanding of the affective and emotional components in pain behaviour and suffering.
Clinical Relevance: This paper aims to provide the dental and medical teams with a review of the classification of trigeminal pain with an overview of how to assess and diagnose patients with trigeminal pain.
Article
Classification of chronic orofacial pain
There have been several attempts to classify chronic orofacial pain (OFP) conditions by pain associations. The most used main categories have either been topographical (odontogenic versus non-odontogenic) and/or chronological (chronic versus acute). Several associations with interest in pain have published classifications: The International Association for the Study of Pain;1 International Headache Society (International Classification of Headache Disorders 2nd edn;2 The American Academy of Orofacial Pain;3 and the Research Diagnostic Criteria for Temporomandibular Disorders.4 As one would expect, critique and suggestions for modification for most of these systems has been published.5
The IASP classification1 categorized orofacial pain (OFP) into ‘Relatively Localized Syndromes of the Head and Neck’ composed of five axes. The IASP system does not, however, fully address the psychosocial aspects of pain, which are required in order to provide a more comprehensive view of the disorder. There is a suggested modification of the classification, which may be applicable to the IASP (the Multiaxial Assessment of Pain [MAP]), as it integrates physical, psychosocial, and behavioural data.
The International Headache Society (IHS)2 has published diagnostic criteria for primary and secondary headaches as well as facial pain. Criteria have also been published by the International Association for the Study of Pain (IASP). The impact of trigeminal pain must not be underestimated. Facial pain can be associated with pathological conditions or disorders related to somatic and neurological structures. There are a wide range of causes of chronic orofacial pain and these have been divided into three broad categories by Hapak et al (1991)5 and Woda et al (2006)6 (Table 1):
The commonest cause of chronic orofacial pain are temporomandibular disorders (TMDs), principally myofascial in nature, and a heterogeneous group including arthritides, arthromyalgia and dysfunctional groups.7
As mechanisms underlying these pains begin to be identified, more accurate classifications, which are mechanism-based, are being used. A major change in mechanism has been that burning mouth syndrome probably has a neuropathic cause, using the newly defined definitions, rather than being a pain resulting from psychological causes. However, we still fall short of an established pathophysiologically based classification system for orofacial pain that would clarify diagnostics and potentially be predictive for management outcome.
Incidence
comparable with other pain conditions in the body, and accounts for between 20 and 25% of chronic pain conditions.8 A 6-month prevalence of facial pain has been reported by between 1%3 and 3%9 of the population. In the study by Locker and Grushka,10 some pain or discomfort in the jaws, oral mucosa or face had been experienced by less than 10% in the previous 4 weeks. In 1980, Bonica11 estimated that 5–7 million Americans suffered from chronic pain in the face and mouth, and 25–45% were affected at some time in their lives. Most population-based studies have shown that women report more facial pain than men,8,9,10,11 with rates approximately twice as high among women compared to men.10 In clinic populations, the rates for women are even higher. On the other hand, other studies have found no sex difference in the prevalence of orofacial pain. Several studies have also shown variability in the prevalence across age groups. The age distribution of the facial pain population differs from that of the most usual pain conditions. In contrast to chest and back pain, for example, facial pain has been suggested to be less prevalent in older age. Consequences include interruption with daily social function, such as eating, drinking, speaking, kissing, applying make-up, shaving and sleeping. Burning mouth syndrome has been reported to cause significant psychological impact in 70% of patients with temporomandibular joint (TMJ) pain; 29% of patients report high disability resulting in unemployment.7
Assessment and diagnosis of orofacial pain
Often, patients with OFP will be seen by a clinician who has experience in one aspect of orofacial pain. Dentists will explore dental pain, an ENT surgeon will assess for sinus and ear-related pain, etc. Consulting a patient in pain requires specific skills and excellent communication. Patients are often anxious visiting the dentist without pain; whilst in pain their anxiety levels are potentially increased, related to the imminent treatment necessary to treat the cause of their pain. Communication is key to eliciting an appropriate history from your patient and the clinician must be a good listener. The patient must also be able to communicate clearly and this is often difficult, for example, children, intellectual disability in the general population (2.5%), cerebral palsy, dementia in 8% of people over 65 years, brain damage (5–1.9 million head injuries per year with 10% of these being serious).12 These people are all even more vulnerable to pain because of their inability to communicate how they feel.
In order to provide each patient with the most suitable treatment plan to address individual needs, it is essential to discover as much information as possible about each patient's experience, expectations, health and quality of existing dentures. Ideally, a multidisciplinary team should assess complex chronic pain patients including: dentists, neurologists, clinical psychologists, psychiatrists, neurosurgeons and pain management consultants.
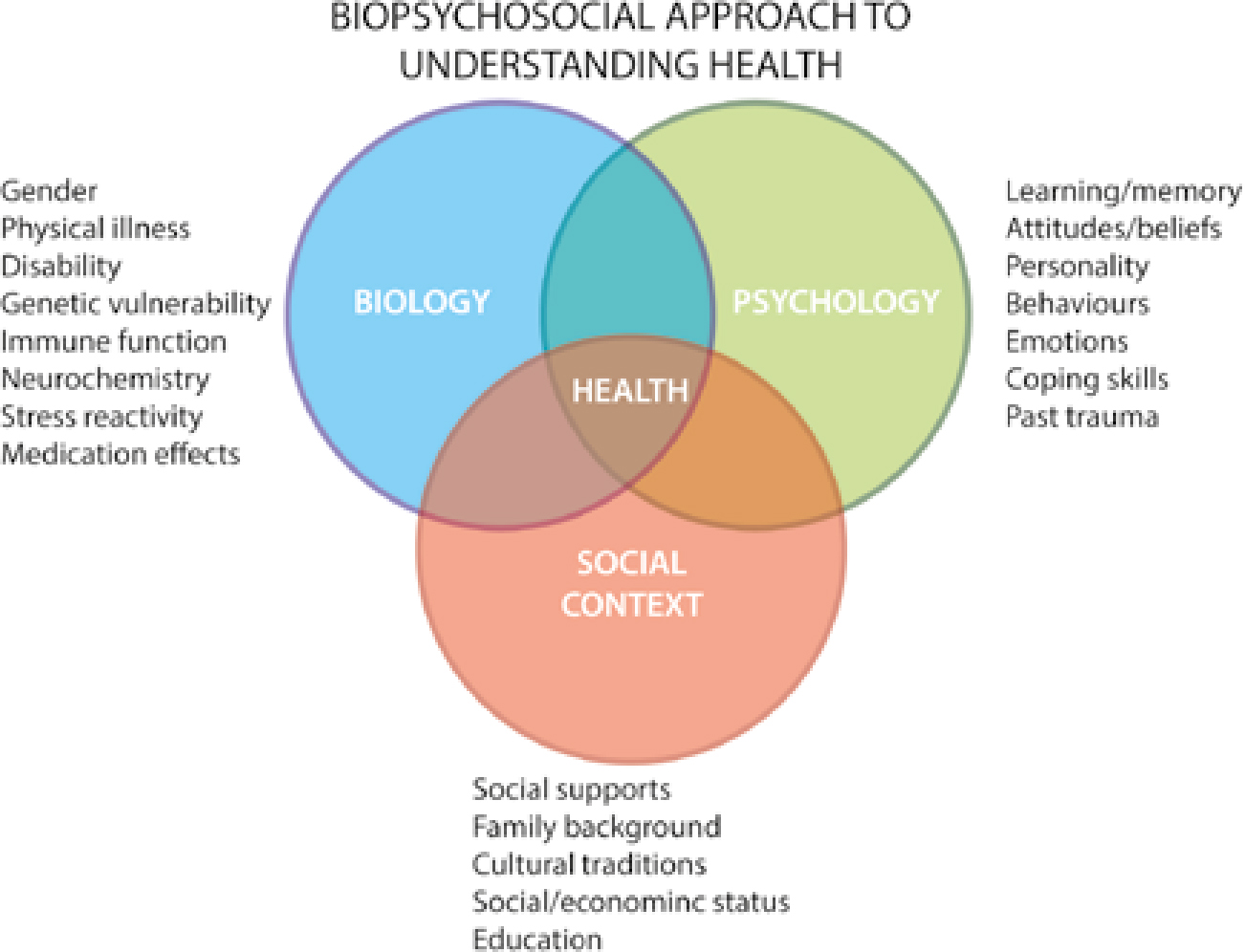
Patient presentation with persistent pain is often complex and may be driven by many factors. Patients may be fit and well or have significant co-morbidity, including psychological, medical history complexities, or have difficulty managing their anxieties and fears. Fear and anxiety will increase the pain experience and may require adjunctive therapy, including behavioural and medical techniques. As pain is multi-dimensional, many aspects of the impact of pain on the patient must be assessed. The biopsychosocial model illustrates the many environmental, phenotypic and psychological factors (Figure 1).
Figure 1. The biopsychosocial model of pain.
These factors must be taken into account when consulting the pain patient. The attentive, listening clinician will build a rapport with his/her patient rapidly and the ensuing trust will allow the patient to confide in the attending clinician, providing invaluable information about the ongoing complaint. Managing patients' expectations is paramount and often a cure is not possible but management is; providing the patient with a clear understanding of what is taking place with realistic goals is essential.
Communication skills
Communication skills underpin a successful consultation for chronic pain.
Pain is invisible thus diagnosis is based upon what patients can communicate to their clinicians. Good advice is:
The patient must be heard;
Careful listening and confirmation of what the patient is trying to convey will elucidate important features and facts about the patient's experience.
Often a careful history will suffice in making a diagnosis. The cornerstones of assessment and establishing a diagnosis and treatment planning are:
Haematological to exclude systemic medical conditions that may contribute to the development or exacerbation of orofacial pain (Table 6):
Histological investigations may be indicated if a pathological lesion is discovered. Neurologists routinely biopsy tissues to quantify peripheral nerve density in patients presenting with neuropathy, usually from lower limbs for diabetic patients. This routine practice is more of a challenge for patients with orofacial pain as sampling facial skin will leave a scar;
Adjunctive neurological tests may include quantitative sensory assessment, nerve conduction tests and somatosensory evoked potentials;
Functional, neurological, psychological assessment ideally undertaken by a multidisciplinary team.
Site – Where is the pain? Or the maximal site of the pain.Onset – When did the pain start, and was it sudden or gradual?(Include also whether it is progressive or regressive.)Character – What is the pain like? An ache? Stabbing?Radiation – Does the pain radiate anywhere? (See also Radiation)Associations – Any other signs or symptoms associated with the pain?Time course – Does the pain follow any pattern?Exacerbating/Relieving factors – Does anything change the pain?Severity – How bad is the pain?
Inspection of the head and neck, skin, topographic anatomy, and swelling or other orofacial asymmetry;
Palpation of the temporomandibular joint and masticatory muscles, tests for strength and provocation. With assessment and measurement of the range of mandibular movement;
Palpation of soft tissue (including lymph nodes);
Palpation of cervical muscles and assessment of cervical range of motion;
Cranial nerve examination (usually excluding cranial nerve 1 (olfactory) and VII (vestibule cochlear) and include examination of C2 and C3 as cervicogenic referred pain is not uncommon;
General inspection of the ears, nose and oropharyngeal areas;
Examination and palpation of intra-oral soft tissue;
Examination of the teeth and periodontium (including occlusion).
Diagnostic requirements:
Identify signs of: Inflammation
Redness swelling heat pain (tenderness)
Response to anti-inflammatories
Response to antibiotics if initiated by infection
Tenderness to percussion of a tooth-indication of periapical periodontitis
Loss of function
Trismus, inability to bite on tooth, difficulty swallowing
Neuropathy
Pulpal testing (ethyl chloride)
Non response does not signify pulpal necrosis, positive response may be complicated in multi-rooted teeth with varying rates of pulpal death in different canals
Hyper-responsiveness to cold may indicate that the pulp is inflamed reversibly and hyperaemic
Hyper-responsiveness to heat may indicate irreversible pulpitis
Pain with sweetness may indicate leakage into the pulpal cavity via caries or fractured breached crown
Intermittent hypersensitivity on biting may indicate ‘cracked tooth syndrome’ using a ‘tooth sleuth’ or simply a mirror handle between the tooth cusps. Pain will often be elicited on biting down on the instrument
Neuropathic sign
Mechanical allodynia (pain to touch)
Thermal allodynia (pain with hot or cold)
Hyperalgesia (increased pain to painful or noxious stimulus)
Radiographs
Long cone periapical for individual to 3 teeth in single quadrant
If multiple quadrants or impacted teeth use DPT
Rarely additional radiographs are required (spreading infection covered in Oral Surgery section)
McGill Pain questionnaire short version (Dworkin et al (2009) developed the SF-MPQ-2)20
OHIP 14 Health Impact Profile (also known as the OHIP-14 Questionnaire), which asks about the frequency of 14 functional and psychosocial impacts that people have with oral functional problems24
Pain detect and question survey to detect neuropathic pain versus inflammatory pain25
EuroQOL (EQ-5D™) is a standardized instrument for use as a measure of health outcome26
Full blood count with haematinics (Fe (Iron), B 12, Folate)
Deficiency in haematinics may cause peripheral neuropathies and burning type sensations
Zinc level
Required for Fe absorption
Haemoglobin A1C or HbA1C
The more glucose in the blood, the more haemoglobin A1C or HbA1C will be present in the blood. Exclude Diabetes, a common cause for painful neuropathy
Thyroid function tests
Hypothyroidism may be associated with sensory neuropathy
Autoantibody screen Extractible nuclear antibodies and anti-nuclear antibodies NAs
When connective tissue disease is suspected (rheumatoid, systemic erythematosis, Lupus, Sjögrens, Polymyositis)
For pain diagnosis the standard history and examination should be augmented with specific questions relating to the history (Table 2) and specific examination of the mouth and special tests (Table 3).
A recent report13 on the differential diagnosis of orofacial pain (OFP) highlights some important strategies to help distinguish between OFP conditions and comes to a diagnosis or differential diagnoses. History-taking remains of paramount importance in facilitating the diagnostic process. There are specific guidelines for the assessment and diagnosis of neuropathic pain.14,15 Several recent studies have made further recommendations regarding neurological assessment of patients presenting with orofacial pain.16,17 However, it remains a challenge to assess these often complex patients fully and a multidisciplinary team is essential.18
There are many systemic conditions that can and must be excluded in order to make diagnoses, for example burning mouth syndrome is a diagnosis by exclusion. Neoplasia can occasionally mimic or masquerade as orofacial pain; though rare this must always be excluded and fear of cancer is likely to be a prominent reason for the patient seeking care.19 Risk factors or RED Flags for occult neoplasia include:
Age over 50 years;
Sudden recent onset and intense pain, motor or sensory neuropathy;
Painless persistent lymphadenopathy;
Painless trismus;
Worsening trismus despite therapy;
Developing spontaneous asymmetry;
Trigeminal neuralgia in patients under 50 years can be suspected to be multiple sclerosis. Conversely, some orofacial pain conditions may masquerade or be misdiagnosed or misinterpreted as toothache, for example trigeminal neuralgia.
Measuring pain
Measuring pain is near impossible. The pain experience is an entirely individual response. No other person can derive your own experience of pain because you alone experience it and, owing to its complexity, conveying your total pain experience to others is impossible. Unless your clinician is equipped with Dr Spock's (from Starship Enterprise not paediatrics) ability to key into your experience using bi-temporal palpation, sharing your pain experience will depend upon your clinician's talent for listening and empathizing which may, in part, allow him/her to begin to understand your pain. We attempt to gain an idea of the affective component of your pain experience using questionnaires for psychometrics and we use questionnaires to assess your functionality, disability and behaviour. Scoring pain using a Lickhert scale is standard practice but it massively oversimplifies the complex pain experience.
A pain diary may provide both clinician and patient with an extremely useful adjunct to the initial pain history, particularly by clarifying the response of the pain to various medications, avoidance strategies taken by the patient, and identifying factors that exacerbate the pain. Daily changes in the pain are important, for example:
Does the patient wake up at night with the pain? This is very rare for neuropathic pain disorders (trigeminal neuralgia);
Is the pain worst in the morning? This may be an indication of nocturnal bruxism precipitating TMJ pain;
Is the pain worse with stress or anxiety (symptomatic of neuropathic pain)? Does the pain respond to anti-inflammatories (including paracetamol and ibuprofen)? If the pain does NOT respond it is likely to be neuropathic rather than inflammatory pain.
Psychological assessment of the pain patient (Table 5)
In the introductory section to this series the significant component of the affective and emotional role in pain perception, behaviour and suffering is highlighted. As pragmatic clinicians we tend to focus on ‘mechanical/medical’ interventions to prevent the nociceptive pain and forget the ‘holistic’ management of pain. With simple acute inflammatory conditions that can be simply managed with a swift and effective surgical intervention, less understanding of the affective burden is required. However, in chronic pain the emotional components of persistent pain, its social, functional and resultant psychological sequelae, cannot be underestimated.20,29 The biopsychosocial model of pain (Figure 1) emphasizes the complexity of managing pain patients. Many authors have made recommendations regarding the preferred psychological assessment of the pain patient.30,31,32,33,34,35 Our local orofacial pain team, which includes liaison psychiatrist, clinical psychologist, health psychologist, dental clinicians, neurosurgeon, neurologist and pain management consultant, use the questionnaires in Table 5. Using these questionnaires we are able to elicit anxiety and depression that may be contributory to the patient's pain condition. We can identify his/her ability to cope and how impactful the pain is in relation to daily function. Red flags including self-harming tendency and suicidal ideation can also be identified early on, precipitating an expeditious referral to the psychiatrist. Overall, the patients are extremely co-operative with completing these questionnaires and the data collected is undoubtedly facilitating the development of tailored cognitive behavioural techniques for specific orofacial pain conditions.
Summary
Most importantly, the clinician must keep a broad perspective of the patient's presentation and complaint. Systemic diseases, psychological and environmental factors all play a potential role in the patient's pain experience and thus must be considered in order to provide effective pain alleviation and education. The subsequent papers provide an update on the management of acute and specific chronic trigeminal pain conditions. Pain management procedures, including local anaesthesia and the management of anxiolysis (behavioural techniques and medical techniques – sedation), are not included in this series.