Oliver RG The casual attender. Br J Orthod. 1982; 9:(3)154-157
Jones ML, Chan C Pain in the early stages of orthodontic treatment. J Clin Orthod. 1992; 26:311-313
Bradley RL, Ellis PE, Thomas P, Bellis H, Ireland AJ, Sandy JR A randomized clinical trial comparing the efficacy of ibuprofen and paracetamol in the control of orthodontic pain. Am J Orthod Dentofacial Orthop. 2007; 132:511-517
Walker S Root resorption during orthodontic treatment. Evid Based Dent. 2010; 11:(3)
Banks P, Elton V, Jones Y, Rice P, Derwent S, Odondi L The use of fixed appliances in the UK: a survey of specialist orthodontists. J Orthod. 2010; 37:(1)43-55
Emergencies in orthodontics part 1: management of general orthodontic problems as well as common problems with fixed appliances Paul Dowsing Alison Murray Jonathan Sandler Dental Update 2024 42:2, 707-709.
Fixed appliance treatment is a popular treatment modality with a burgeoning increase in the numbers of children and adults realizing the benefits that can be gained. Appliance breakage is an unavoidable nuisance which is at best inconvenient, and at worst may result in significant pain or discomfort for the patient. General dental practitioners (GDPs) should have the practical knowledge of how to provide timely and appropriate orthodontic ‘emergency treatment’. This will significantly reduce the sometimes considerable inconvenience and discomfort for both the patient and his/her parents, and the inevitable frustration for the clinician providing ongoing care. This first paper will deal with general orthodontic problems that commonly present, as well as some issues specific to fixed appliances. The second paper will deal with the other orthodontic appliances that may be encountered by GDPs in their daily practice.
Clinical Relevance: Appropriate handling of an orthodontic ‘emergency’ by the general practitioner will, on many occasions, provide immediate relief of pain and distress for the patient. This will in turn allow treatment to continue moving in the right direction, thus allowing more efficient and effective use of valuable resources.
Article
Orthodontic emergencies, though relatively infrequent, do occur.1 It is generally felt that 90% of the problems come from 10% of our orthodontic patients, and these ‘wreckers’ will be familiar to most practising clinicians. It is not always possible or convenient for patients to get back to see the clinician who is providing their long-term orthodontic care. The GDP may often be the first point of call and is often in an ideal position to provide orthodontic ‘first aid’, should a complication arise.
The aim of these articles is to remind GDPs about the various components of the most commonly used appliances and to give them an idea as to which may give trouble. We also intend to provide useful and practical advice, should the patient attend for an unexpected visit, as a result of breakage of the appliance. By appropriately managing the problem, inconvenience to the patient can be minimized whilst ensuring the continued efficiency and effectiveness of the appliance. There are some orthodontic problems that are common to all appliance types, as well as others that are of a more specific nature.
The most common appliances which may be available for use by GDPs are discussed, with all their attendant problems, as well as some of those less likely to be encountered. The article is not meant as an exhaustive guide but it should be possible to apply many of the principles contained therein to the less commonly encountered scenarios.
Common problems
As with all patients who attend for an emergency appointment, it is important to carry out a brief history of the specific problem, noting any relevant medical conditions, before carrying out a thorough clinical examination. Whenever possible, as the first choice the patient should be directed to the orthodontic practitioner who is responsible for the fitting and maintenance of the appliance, but if this is not possible, the GDP is the next best option. It is unlikely that the patient's general medical practitioner will have a great deal to offer in the majority of orthodontic emergencies, and this should be pointed out to the parents of the patient at the outset.
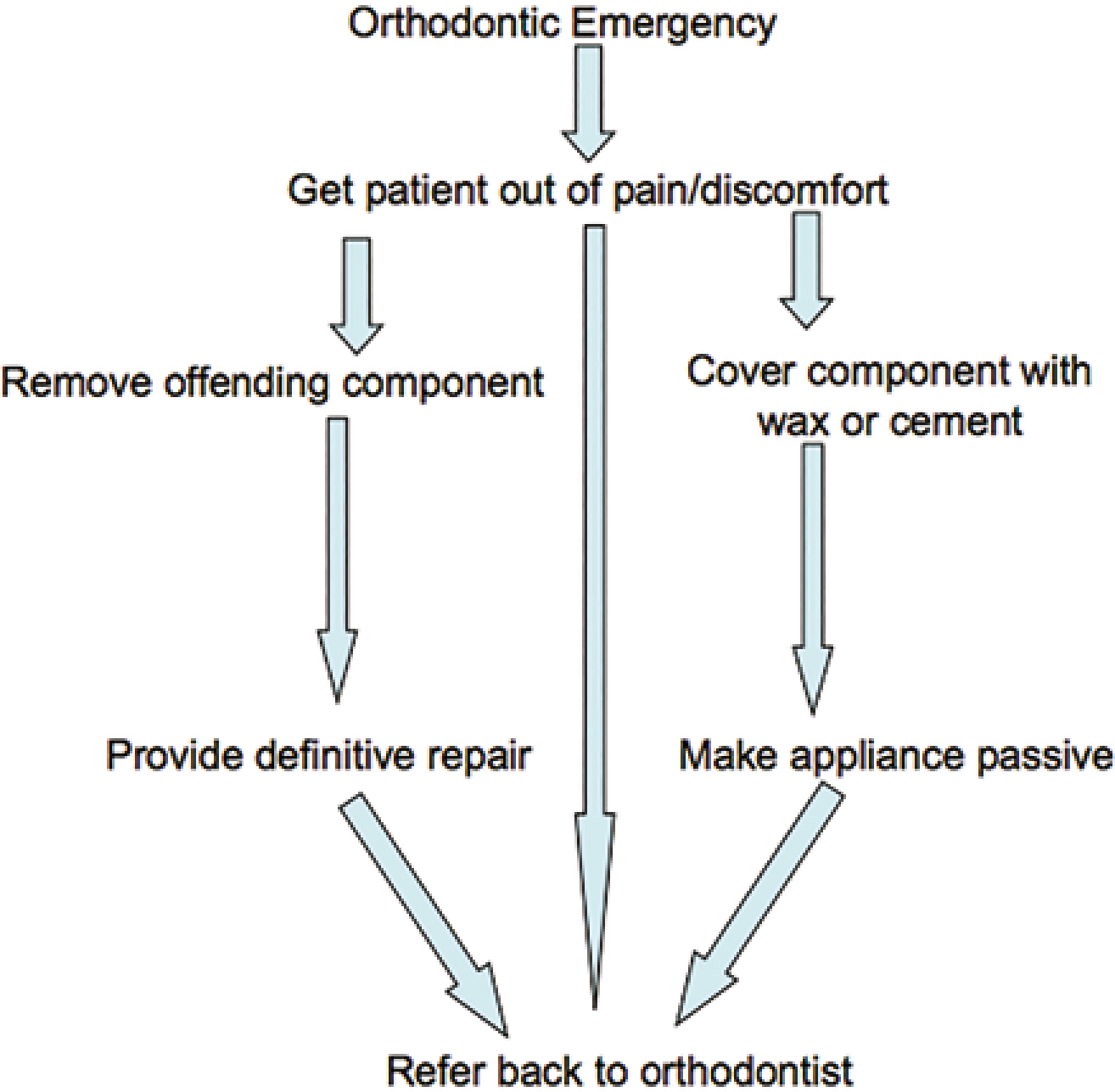
The main objectives for any patient who attends with an orthodontic emergency is firstly relief of any pain or discomfort, secondly to provide reassurance that things will get better and finally, where appropriate, to de-activate the appliance if it is not possible to carry out a definitive repair (Figure 1).
Figure 1. Flow diagram of orthodontic emergency care pathway.
Dental pain following appliance placement or adjustment
Some initial discomfort should always be expected following the placement or adjustment of any type of appliance.2 The patient and the parents must be given appropriate information, both verbally and in writing, as to how to deal with this initial period of discomfort. Over the first few days of orthodontic treatment all that is usually required is appropriate analgesia3 (ibuprofen or paracetamol) and plenty of reassurance and support from the parents. Specific instructions must be given to the patient about maximum doses of analgesics and they must be told never to exceed the doses written on the bottles.
Appliance rubbing on lips and cheeks
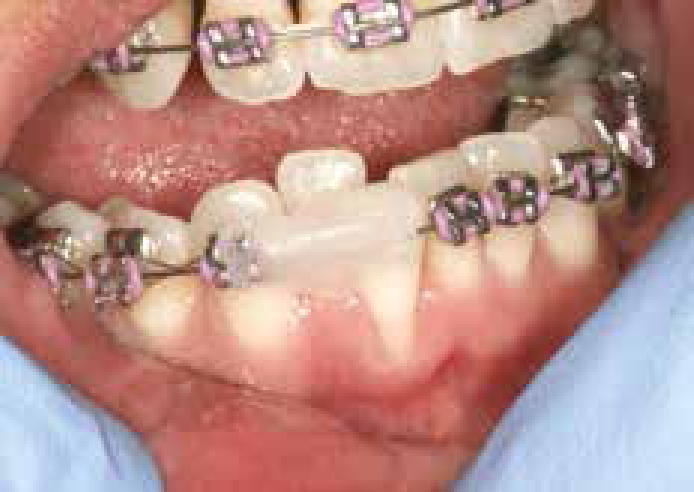
This is a very common complaint, particularly in the early stages of treatment before the patient becomes used to the appliance. Use of ‘relief wax’ is usually an effective measure to reduce discomfort caused by friction between components of the appliance and the soft tissues. The patient must be advised firstly to attempt to dry the area and then to soften the wax by manipulating it between finger and thumb, prior to pinching it together around the offending area (Figure 2). It may be difficult to stick the wax to the offending components and repeated attempts may be necessary.
Figure 2. Orthodontic relief wax applied to prevent further soft tissue trauma.
Demineralization of teeth
Poor oral hygiene and inappropriate diet can be the cause of the most commonly encountered conditions. The majority of potential problems can be avoided by ensuring that the patient receives sufficient information about minimizing sugar-containing foods and drinks, as well as specific instruction in cleaning food from the appliance once it has been fitted. A fluoride-containing mouthrinse should always be prescribed to orthodontic patients, and every time the patient visits a dental professional encouragement should be given to use it regularly.
Advice includes the avoidance of tough or sticky food that may dislodge appliance components, as well as a sensible dietary intake avoiding sugary or acidic food and drink, particularly between meals. There is always a risk that food debris can get stuck between the appliance components and this can usually be effectively removed with interdental brushes, superfloss or a Waterpik, once specific direction in their use has been given.
Soft tissue problems
Severe gingival inflammation may be seen in orthodontic patients and every opportunity must be taken to encourage patients to achieve an exemplary standard of oral hygiene. Gingival infections, such as acute necrotizing ulcerative gingivitis (ANUG), may also be encountered when a patient is receiving appliance therapy, combined with other exacerbating factors, such as students sharing toothbrushes with infected people and smoking. ANUG is diagnosed by the characteristic ‘punched out crater like lesions of the interdental papillae (Figure 3).
Figure 3. ANUG with typical punched out, crater-like lesions of interdental papillae.
Treatment of specific ANUG infections may require non-surgical root debridement, possibly in combination with appropriate antibiotics (Metranidazole 200 mg, TDS for 5 days), as well as specific advice about peroxide mouthwashes, if thought necessary. The need for exemplary oral hygiene procedures must again be stressed, to prevent recurrence of the problem and to re-establish full oral health.
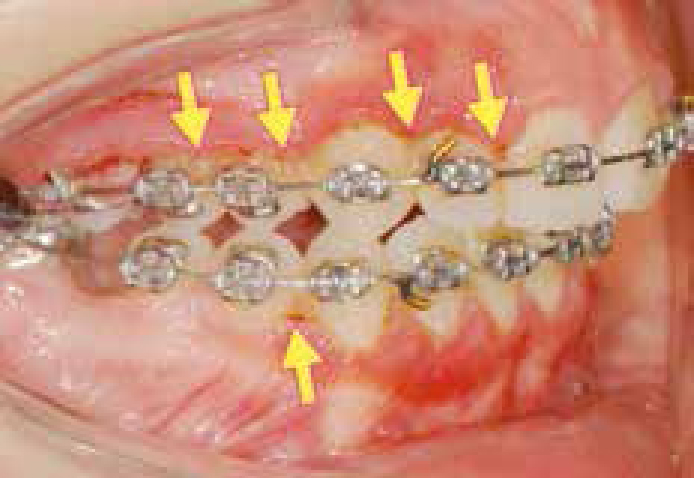
Ideally, all orthodontic treatment should involve an intensive course of oral hygiene instruction prior to placement of any appliances. The patient should be warned that, if oral hygiene is less than exemplary, it would be inadvisable to provide appliance therapy. If the patient is already in treatment when there is a marked downturn in gingival health, and if no marked improvement is forthcoming over the subsequent 2 or 3 visits, then the brace must be removed, otherwise there is a risk of severe permanent damage to the dentition (Figure 4). Ideally, this situation is best avoided by careful patient selection and comprehensive instructions given prior to embarking upon active treatment. If there is any doubt that the risks of treatment will outweigh the potential benefits, then treatment must be withheld.
Figure 4. Demineralization caused by poor oral hygiene and diet during treatment.
Excessive tooth mobility
A slight increase in tooth mobility (0.5–1 mm) is inevitable during most active orthodontic appliance therapy. In most cases, the patient will merely need to be reassured that this is a normal physiological consequence of treatment. Occasionally, during fixed appliance treatment the teeth can become extremely mobile (>2 mm movement on gentle pressure). If there is an obvious local cause, such as occlusal trauma directly on to the mobile tooth, then soft diet should be recommended, and an attempt made to relieve any further trauma on the affected teeth. A temporary ‘bite plane’ can be made from glass ionomer cement, often placed on the upper molar teeth (Figure 5). This will provide immediate removal of the occlusal trauma and within a few days the excessively mobile tooth should firm up again. Occasionally, there is direct tooth contact on to a part of the fixed appliance but the offending component of the appliance is only removed as a last resort.
Figure 5. Temporary glass ionomer bite plane to relieve traumatic occlusion on brackets.
In all cases of excessively mobile teeth, a visit to the orthodontist in the very near future is highly recommended.
Root resorption
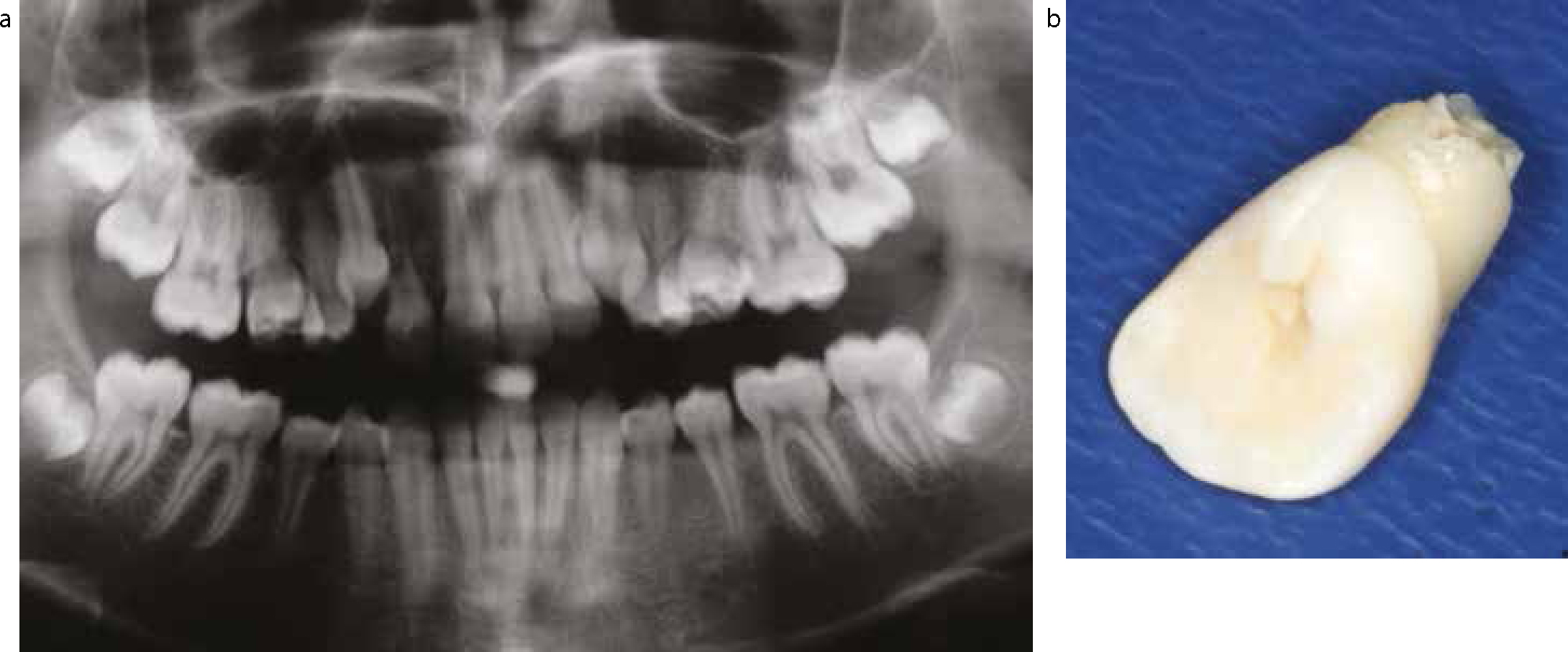
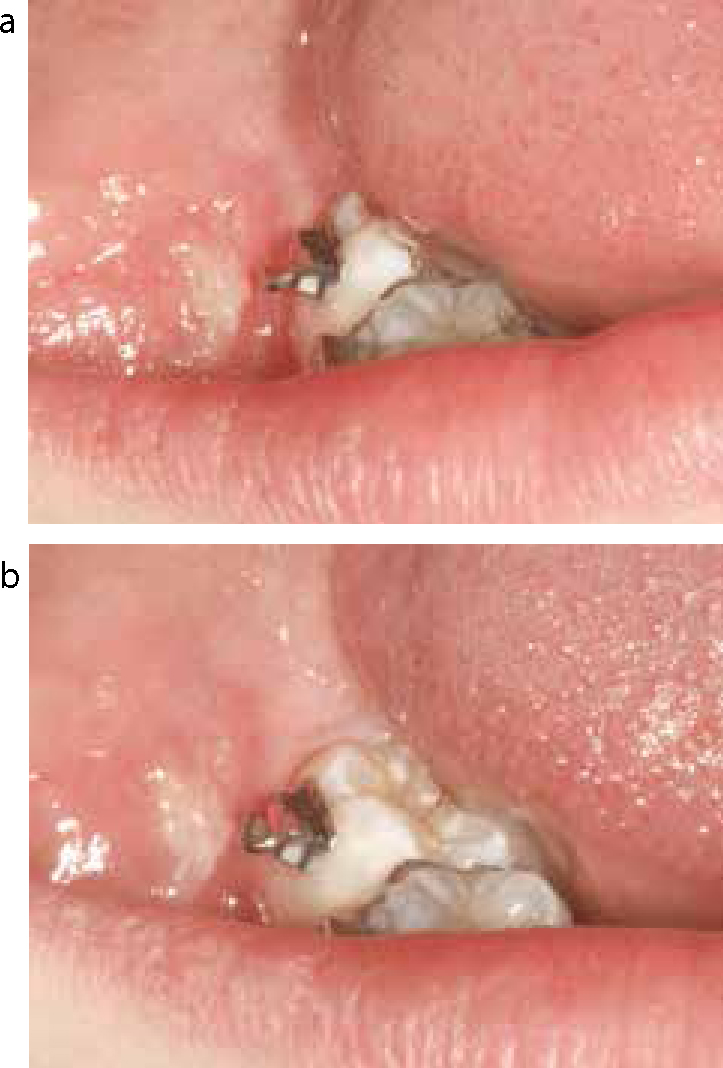
If excessive tooth mobility persists, despite the relief of the suspected contributory factor, then radiographic investigation may be indicated. Root resorption is an inevitable consequence of all orthodontic therapy4 and, in most circumstances, it is clinically insignificant. In a very small number of cases, however, there may be excessive root resorption occurring as a result of the orthodontic intervention. If there is a suspicion that root resorption is occurring, then the patient should be advised to contact the orthodontist immediately. Treatment may need to be halted temporarily, or occasionally permanently, depending on the extent of the problem (Figures 6a and b).
Figure 6.
(a) Root resorption seen on OPT. (b) Markedly shortened lateral incisor root.
Common types of orthodontic appliance
Undergraduate training may not have provided significant exposure to contemporary orthodontic appliances and techniques to give the practitioner sufficient confidence to deal with some of the common orthodontic ‘emergencies’. This next section will describe the most frequently used fixed orthodontic appliances, their individual components and the problems that may be encountered.
Fixed appliances
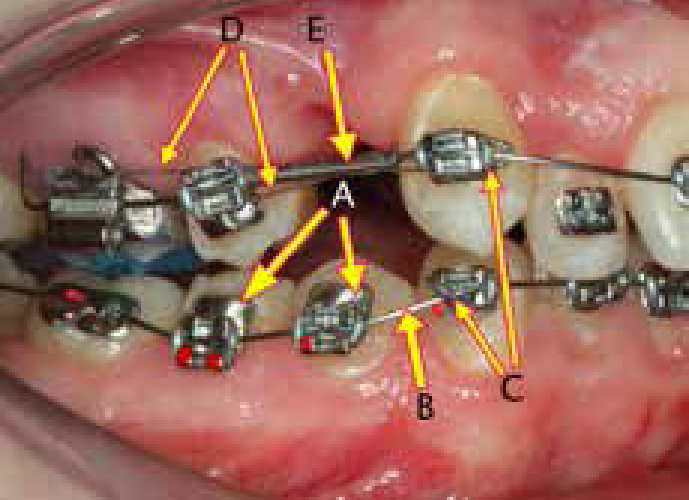
The pre-adjusted edgewise appliance (straightwire appliance) is the most commonly used fixed brace used by the contemporary orthodontist.5 Ideally, the GDP should be familiar with the main components of a fixed appliance that can be divided into (Figure 7):
Figure 7. Fixed appliance comprises: A – Brackets; B – Archwire; C – Modules; D – Laceback; E – Stainless steel tubing.
Bands and brackets;
Archwires;
Modules;
Lacebacks; and
Stainless steel protective tubing.
Familiarity with each of these components will be a distinct advantage when providing emergency treatment. The more commonly encountered problems are listed, and practical tips on how to resolve them are described.
Lost elastic or wire module
Occasionally during a treatment, an elastic module or wire ligature, which are merely used to hold the archwire into the bracket, may be lost (Figure 8). It is necessary to replace this ligature or module as soon as possible, as it is the primary means of providing control of the tooth position. If there are elastic or metal ligatures in the practice, it takes a matter of seconds to re-attach the bracket to the archwire. In the absence of ligatures, a referral back to the orthodontist is essential, to minimize the inevitable unwanted movements of the non-attached teeth.
Figure 8. Lost module with resultant unwanted tooth movement.
Archwire wire traumatizing soft tissues
Protruding distal ends of archwires can lead to soft tissue trauma and to large and painful ulcers. One cause may be that the main archwire was not trimmed correctly at the end of the last visit, with excessive wire being left protruding from the molar tube when the patient left the surgery (Figure 9). Excessive wire protrusion may also occur as a consequence of active tooth movement, such as space closure, or alternatively by the archwire sliding round from one side of the arch to the other. Occasionally during treatment there may be fracture of the main archwire caused by inappropriate foods or destructive habits, such as biting the end of a pen or pencil, which hardens the wire, leading to breakage. This may result in one or more sharp ends protruding into the soft tissues.
Figure 9. Wire protruding from distal of molar band causing traumatic cheek ulcer.
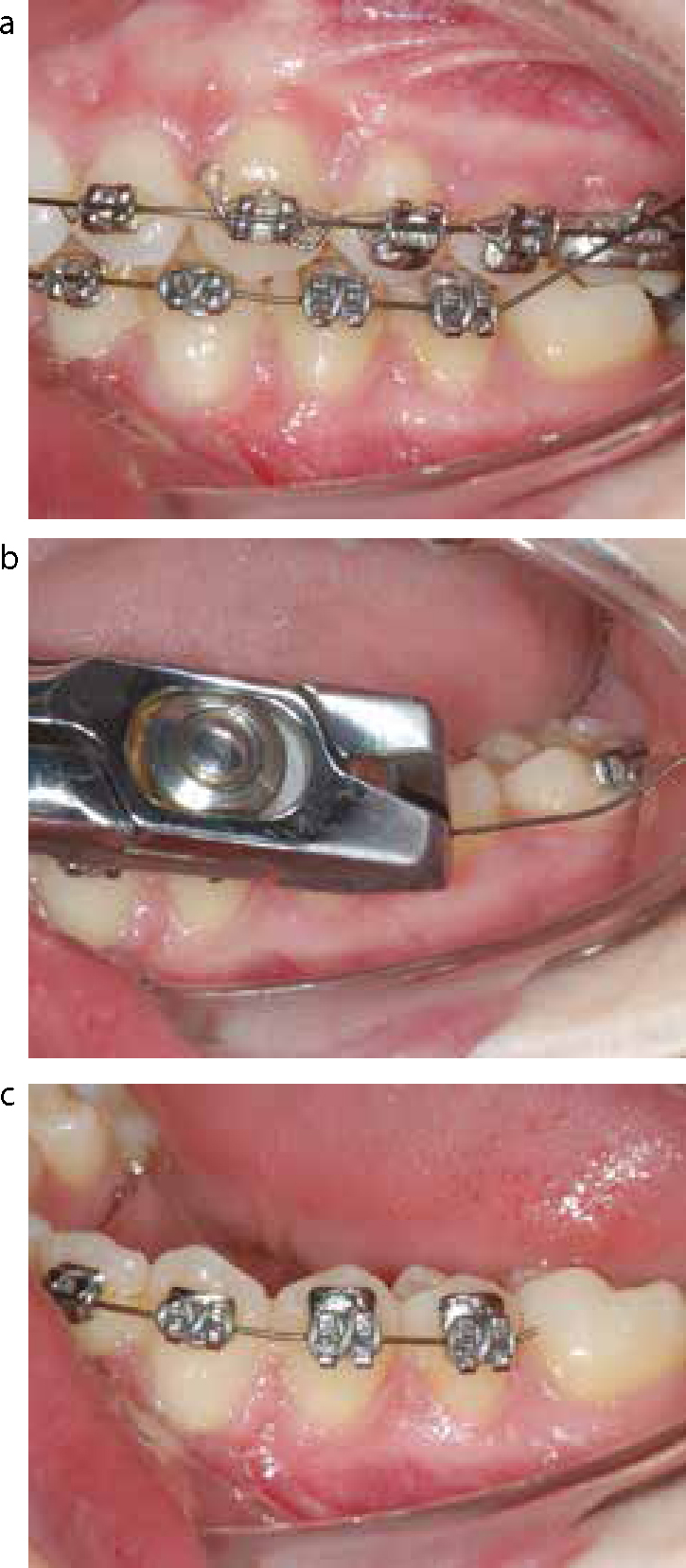
Distal end-cutters can be used if available to remove the offending bits of wire as they are specifically designed to resolve this problem (Figures 10 a–c). Alternatively, this problem can be resolved within seconds by removal of the protruding sharp end with either wire-cutters or an air-turbine (Figure 11). Care must be taken to hold on to the excess wire, to ensure that it doesn't become a loose foreign body, by placing a clip on the distal end to be cut. A piece of dental gauze to catch the loose fragment is a strongly recommended secondary precautionary measure.
Figure 10.
(a) Lost molar bond results in excess uncontrolled wire. (b) Sharp archwire cut safely with distal end-cutters. (c) Appliance made ‘safe’.Figure 11. Air turbine used to cut archwire if no cutters to hand.
Alternatively, the wire may be bent into a non-traumatic position but bending the wire may prove to be difficult with flexible archwires, such as those made from nickel-titanium. Bending is also best avoided where the wire protrudes through bondable tubes rather than bands, as wire manipulation often leads to the tubes being dislodged.
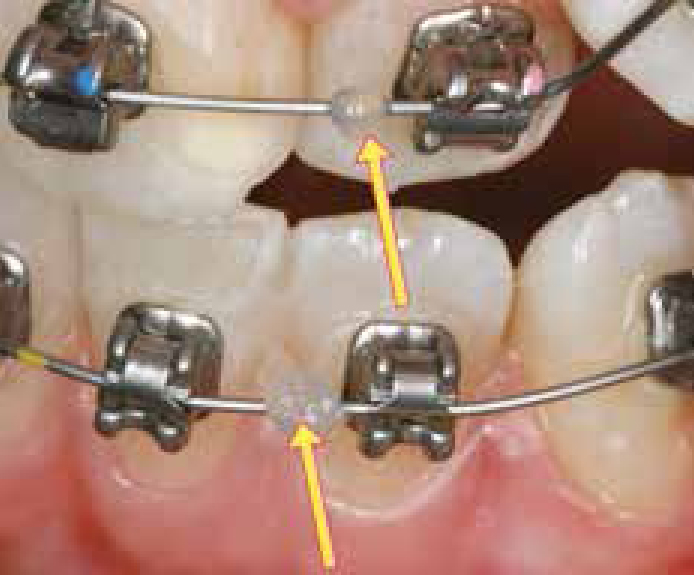
If the archwire has slid round to one side, then it may be possible to reposition it. The general practitioner can try to slide the wire distally on the side other than the one the patient is complaining about. The wire can sometimes be fed carefully through the molar tube and all the excess wire on the opposite side should be ‘taken up’; this is by far the simplest solution, which will provide immediate relief. The patient should then be referred back to the orthodontist. Archwires sliding round is an increasingly common occurrence with the burgeoning increase in use of self-ligating brackets. To avoid this happening the treating clinician should use some form of archwire stop, eg crimped stainless steel tubing or hooks on the wire, or placement of a composite or glass ionomer blob bonded to the wire, ensuring it cannot pass through the brackets (Figure 12).
Occasionally, the hook from the molar tube may be prominent enough to cause trauma to the soft tissues of the cheek (Figure 13a). Options to resolve this problem are: placement of wax over the hook, placement of GIC or composite over the hook (but avoiding the archwire) or bending the hook to an atraumatic position (Figure 13b). Great care will need to be taken, especially with bondable tubes, to ensure that the component is not detached from the tooth as an attempt to bend it is made.
Figure 13.
(a) Trauma to cheek mucosa caused by hook on bondable tube. (b) Very careful adjustment of the hook solves the problem.
Loose archwire/auxiliary wires
An auxiliary wire, such as a canine laceback or long ligature, may become loose, particularly in the early stages of treatment when rapid tooth movement is occurring. A decision will need to be made whether the wire can just be retied or whether it should be removed. If there is any doubt then removal is preferable and the patient should be told to revisit his/her orthodontist at the earliest opportunity.
Occasionally, an archwire may become loose, either due to loss of a number of modules or as a result of biting forces on a flexible section of the wire, causing it to be pulled out of the archwire slot or molar tube. Archwire deflection is particularly common if there is a large unsupported span of wire. This potential problem can be minimized by the orthodontist annealing then bending down the end of the flexible archwire, or preferably strengthening the unsupported span of wire with stainless steel tubing (Figure 14). For the GDP the challenge is to sort out the immediate problem of the archwire out of the tube. If the wire is sufficiently flexible, then it can normally be fed back through the molar tube (Figure 15), particularly if 3 or 4 modules are removed anterior to the dislodged archwire. The alternative is to cut the loose section of archwire flush with the distal end of the premolar bracket and again recommend the patient to visit his/her orthodontist as soon as possible.
Figure 14. Archwire bent in and tubing to support flexible archwire, to minimize archwire movement.Figure 15. Flexible archwire fed back into buccal tube if displaced.
Loose bracket
Brackets may become loose as a consequence of eating hard or sticky foods, possibly a premature contact leading to traumatic occlusion or occasionally by external trauma during contact sports. The bracket may remain flush with the tooth surface or may get pushed along the archwire. One option available to the GDP is to leave the loose bracket in situ, provided it is secured to the archwire and not causing or likely to cause any problems of trauma to either the soft tissue or dentition. If the loose bracket is causing soft tissue trauma or discomfort or inconvenience to the patient, then it can be removed by taking off the ligature holding it to the archwire (Figure 16). Care must be taken when doing this not to dislodge adjacent brackets.
Figure 16. Module removed, prior to loose bracket removal from the archwire.
Self-ligating brackets can also be problematic as each one has a different opening technique, sometimes requiring a specialized instrument. Occasionally, the clip holding the archwire may open inadvertently or fracture (Figure 17), causing the release of the archwire or trauma to the adjacent soft tissue. If it is not possible to close the clip again or remove the fractured component, orthodontic relief wax can be placed over the area causing the problem. In all cases, early specialist orthodontic attention is desirable and the need for an urgent appointment should be stressed to the patient.
Figure 17. Fractured clip removed from self-ligating bracket.
Loose orthodontic molar band/tube
Problems caused by a loose band include, loss of control of the tooth position, which is obviously the primary concern, but also soft tissue trauma from the mobile band, as well as potential food packing and, if prolonged, demineralization of the enamel. Loose bands can easily be re-cemented with glass ionomer after removing a ligature or two anterior to the band and sliding it off the archwire, then cleaning both the band and the tooth. If a band is loose and posing a possible threat of ingestion or inhalation, then it is certainly best removed. Occasionally, this may require cutting and removal of the archwire and possibly accessory wires that were attached to the band.
If a bondable molar tube comes away from the tooth surface then this should be removed, together with any associated wires, to minimize the chance of trauma to the surrounding soft tissues or ingestion or inhalation. The patient should then be referred back to the orthodontist in charge of the case.
Nance appliance/transpalatal arch/lingual arch
Soreness in the roof of the mouth may be caused by an ill-fitting Nance button or, alternatively, a loose band allowing undue movement of the acrylic against the palate (Figure 18). Options for a loose band include removal and re-cementation of the Nance palatal arch, that could be carried out by the GDP if he/she has some band-removing pliers. Re-adapting the appliance to improve the fit of the Nance button is possible using triple beaks, but is a technique only the orthodontist treating the patient should perform.
If palatal trauma and inflammation is severe, then removal of the Nance palatal arch may be the only reasonable option. The palatal soft tissues invariably recover very quickly over the next few days once the source of irritation has been removed.
If one of the soldered joints of one of the retaining bands has fractured, then the Nance button can be removed, leaving the other unaffected band in situ, by cutting the arch on the undamaged side free using an air rotor or heavy duty wire-cutters. In this case, a new band will need to be fitted and a further alginate impression taken by the treating orthodontist to allow a new appliance to be fabricated.
Complications caused by simple transpalatal arches or lingual arches are usually less common than with Nance palatal arches and tend to be limited to fractures of the soldered joint, retaining bands becoming loose or, occasionally, bands splitting (Figure 19). All these can be dealt with by cutting the arch close to the undamaged band and smoothing down the cut end with an air turbine. Very occasionally, a palatal or lingual arch or quadhelix may become so buried in the soft tissues that local anaesthetic is required to ensure comfortable removal of the arch (Figure 20). If a general practitioner was confident enough to do this for the patient then, if possible, a photograph of the problem prior to the surgical intervention would be of great benefit for the treating practitioner, for future reference.
Figure 19. Split of molar band on lingual arch.Figure 20. Removal of embedded quadhelix.
Quadhelix
Two types of quadhelices exist:
A soldered version, which is permanently attached to molar bands; or
A removable MIA quadhelix, which has attachments that slot into a sheath welded to the palatal surface of the molar bands.
Either quadhelix may lead to trauma from helices to either the tongue or palatal soft tissues. Some relief of tongue trauma can be provided by applying cement to the helix (Figure 21).
Figure 21. Cement on helix reduces trauma to soft tissues.
If there are obvious signs of pressure to the soft tissues of the palate, then it may be possible to re-adapt the quadhelix in situ using triple beaks. This is a job for the orthodontist providing treatment and the patient should be asked to make an appointment at his/her earliest convenience.
A fixed quadhelix suffers some of the same complications as a Nance appliance with regards to the soldered joints (Figure 22). If the appliance is causing the patient discomfort or inconvenience, it is often better to remove the offending part of the appliance and refer the patient straight back to the orthodontist for urgent attention (Figure 23).
Figure 22. Fracture of soldered joint on a Nance palatal arch.Figure 23. Nance button removed by cutting palatal arch.
A removable quadhelix may become loose because of failure of the retaining bands, in which case it should be dealt with as a soldered quadhelix. It may also become loose due to failure of the welded sheath into which the quadhelix fits. If the weld has failed then the quadhelix should be removed, as a new sheath will need to be re-welded to the band. If the quadhelix just becomes loose due to displacement from the sheath, then it can be re-seated and secured with an elastic or wire ligature if the GDP is happy so to do (Figure 24).
Figure 24. Reseated removable quadhelix secured with elastomers.
Hyrax or Hass appliance
One other appliance, which may occasionally be encountered, is that used for rapid maxillary expansion: namely the Hyrax or Hass type of appliance. Occasionally, there can be concern from patients regarding the pressure they are feeling in the teeth and jaws caused by this type of appliance. The patient is actively expanding the arch with a midline screw (Figure 25) which he/she will be turning, a quarter turn, on a twice daily basis. If the pressure becomes intolerable then it is possible to obtain immediate relief by turning the midline screw back by a quarter turn. During the early stages of active expansion it is inevitable that the patient will develop a large midline diastema (Figure 26). This will resolve spontaneously when expansion is stopped and therefore all that is required is reassurance to the patient that the increase in the midline gap will reduce to pre-treatment levels without any active intervention whatsoever.
Figure 25. Hyrax appliance with mid-line expansion screw.Figure 26. Mid-line diastema inevitable during rapid maxillary expansion.
Should a patient attend with a loose or split band on an RME device, then he/she should be referred immediately back to the orthodontist as, apart from dispensing ‘relief wax’ or smoothing down sharp band edges, there is little emergency treatment that can be carried out on these devices by a non-specialist.
Conclusion
The general dental practitioner, owing to the burgeoning increase in the popularity and usage of orthodontic appliances, may encounter problems relating to fixed appliances. This first article will hopefully familiarize the clinician with the main types of fixed appliances and their component parts, as well as giving valuable insight into the most common problems experienced by their patients. This will allow the general dentist to provide advice on appropriate management of problems, ensuring that there is minimal disruption to the treatment process. The second article will deal with problems that might arise with the other types of orthodontic appliance in use today.