Hulsmann M Dens invaginatus: aetiology, classification, prevalence, diagnosis, and treatment considerations. Int Endod J. 1997; 30:79-90
Reddy YP, Karpagavinayagam K, Subbarao CV Management of dens invaginatus diagnosed by spiral computed tomography: a case report. J Endod. 2008; 34:1138-1142
Oehlers FA Dens invaginatus I. Variations of the invagination process and associated anterior crown forms. Oral Surg Oral Med Oral Pathol. 1957; 10:1204-1218
Gomel M, Seckin T An erupted odontoma. J Oral Maxillofac Surg. 1989; 47:999-1000
Ĉuković-Bagić I, Macan D, Dumanĉić J Dilated odontome in the mandibular third molar region. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 109:e109-e113
George R, Moule A, Walsh L A rare case of dens invaginatus in a mandibular canine. Aust Endod J. 2010; 36:83-86.237
Tüzüm MS Orofacial pain associated with an infected complex odontoma. Case report. Aust Dent J. 1990; 35:352-354
Schulze C [Unusual forms of coronal invagination (dens in dente) and similar appearing twin formations]. Dtsch Zahn Mund Kieferheilkd Zentralbl Gesamte. 1972; 58:73-101
Tsurumachi T, Hayashi M, Takeichi O Nonsurgical root canal treatment of dens invaginatus type II in a maxillary lateral incisor. Int Endod J. 2002; 35:68-72
Sashi Nallapati Clinical management of a maxillary lateral incisor with vital pulp and type 3 dens invaginatus: a case report. J Endodont. 2004; 30:726-731
The value of cone beam CT in assessing and managing a dilated odontome of a maxillary canine Aoibheann Wall Suk Ng Serpil Djemal Dental Update 2024 42:2, 707-709.
Authors
AoibheannWall
BDS, MFD RCSI
Senior House Officer, King's College Hospital, Dental Institute, Denmark Hill, London SE5 9RS, UK
A case of an unusual anomaly in a maxillary canine is described. A deep enamel invagination resulted in pulpal necrosis, longstanding infection and development of an associated radicular cyst. Diagnostic X-ray imaging was invaluable in demonstrating the complex root anatomy of the dilated odontome. In particular, a cone beam CT scan helped in the formulation of an appropriate treatment plan.
Clinical Relevance: Three-dimensional imaging using cone beam CT was valuable in this case to demonstrate the complicated anatomy of a rare dental anomaly, and to help plan treatment.
Article
Developmental anomalies in teeth cover a wide spectrum of complexity of anatomy, which can sometimes be challenging to diagnose and manage. Dilated odontomes are also known as dens invaginatus, gestant odontome and dens in dente.1 The different names represent the varied opinions on the aetiology. Dens invaginatus is a well known tooth anomaly which is the result of an infolding of the enamel epithelium during tooth development. The deformity in the crown, and sometimes the root, acts as a channel and brings oral bacteria much closer to the pulp, frequently causing early pulpal necrosis. The most commonly affected tooth is the maxillary lateral incisor, followed by the maxillary central incisor, while other teeth, including the maxillary canine, are occasionally invaginated.2 A review of the literature has identified only six published cases of dilated odontomes occurring in maxillary canines.
The most regularly used classification system for dens invaginatus is that by Oehlers who described three forms of the anomaly:3
Type 1 – the enamel-lined invagination is limited to within the crown of the tooth, not extending beyond the cemento-enamel junction.
Type 2 – the enamel-lined invagination extends apically past the cemento-enamel junction, but remains within the root.
Type 3 – the enamel-lined invagination extends apically beyond the cemento-enamel junction and perforates apically to create an apical or periodontal foramen. In the most severe form, Type 3, also named dilated odontome, the tooth has a circular or oval shape with a radiolucent interior.
The pathogenesis of dilated odontomas has been associated with incidents of trauma during the primary dentition stage, hereditary anomalies, as well as with inflammatory and infectious processes.4 The malformation typically occurs during the morpho-differentiation stage of tooth development, but the exact aetiology and genesis are still unknown.5 Owing to their unusual radiographic appearance, such teeth are often incorrectly diagnosed as a double root, a radicular invagination, or a toothtwin.
Dens invaginatus has a prevalence of between 0.04% and 10%.6 Most odontomes are diagnosed in the second decade of life and are typically found on clinical and radiographic examination for some other complaint.7 The coronal opening is called the orificium and the exit, either apically or laterally, is known as the pseudoforamen apicale sive laterale.8
Various treatment choices are available for dilated odontomes, depending on the anatomy of the odontome and the pulpal status. Early sealing of the coronal defect, with regular monitoring, may reduce the need for further treatment (either extraction or root canal treatment) in the future.1 Owing to the presence of enamel invagination, bacterial ingress is common, and rapidly results in necrosis of the pulp. At this point, one possible treatment method is by non-surgical root canal therapy,9 depending on the anatomy of the pulp chamber and root canals. Another reported treatment modality is by combining both non-surgical and surgical endodontic techniques.10 Sometimes, due to complex anatomy, extraction is the only viable treatment option.
Case report
A fit and healthy 14-year-old school boy was referred to King's Dental Institute by his general dental practitioner who had started root canal treatment on the UL3, but this was aborted as a result of ‘unusual anatomy’. The patient had experienced three episodes of facial swelling associated with the tooth over the past 2 years, each time being managed with antibiotics (Penicillin V, amoxicillin and metronidazole). The most recent flare up was 3 days prior to the hospital consultation appointment. There was no history of trauma nor of any known pre-disposing genetic association. Extra-oral examination revealed a diffuse swelling affecting the left side of his face, lower eyelid, zygoma and cheek.
Intra-oral examination revealed a fluctuant swelling in the buccal sulcus of the UL2 and UL3 region. He had a Class 2 division II malocclusion with moderate crowding in the lower labial segment. His dentition was unrestored and there was a retained lower left second deciduous molar tooth which was firm. The appearance of the upper left canine was similar to the contralateral canine from the facial aspect and had a pronounced cingulum palatally (Figure 1). Unfortunately, there was an access cavity and temporary restoration already present so that the enamel invagination was not seen.
Figure 1. Upper left canine with pronounced palatal cingulum. Temporary restoration conceals any possible enamel invagination.
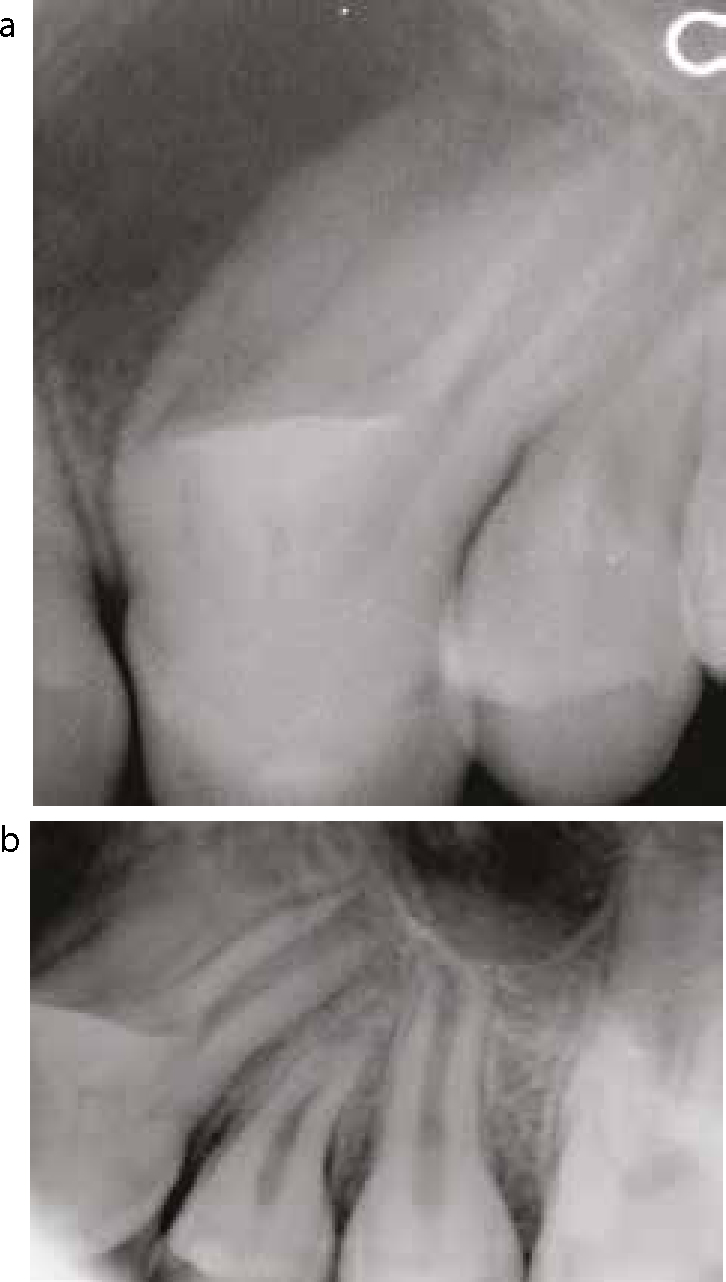
Periapical radiographs of the UL3 showed a double enamel shadow in the crown, two distally curved roots, and a marked concavity beginning 3–4 mm from the cemento-enamel junction on the mesial aspect. There was a well defined, unilocular, radiolucent area surrounding the root of the UL3 which extended beyond the periapical image receptor (Figures 2a, b).
Figure 2.
(a) Periapical radiograph of UL3. Note abnormal morphology and crown-root alignment. The radiolucency mesial to the roots is pathological. (b) Periapical radiograph of UL3. The development of UL4 is being affected by the abnormal UL3 root. Note radiolucent normal maxillary antrum above UL5.
At this stage, a diagnosis of endodontic abscess UL3 was made and the fluctuant swelling was incised and drained. Arrangements were made for a cone beam computed tomography (CBCT) scan to be carried out.
The CBCT scan (Accuitomo, J Morita Mfg Corp, Japan) showed an abnormal shaped canine with enamel invagination in the crown, and two divergent roots (Figures 3a, b, c). The coronal sections show tortuous enamel invagination and identified the buccal root as the larger, with an inward-pointing hook at the tip (Figure 3b). A unilocular, round, radiolucent lesion of size 16 x 10 x 10 mm with a well-defined margin was present associated with the roots. The sagittal sections show the deep, tortuous enamel invagination extending to the bifurcation area, while the axial sections show a ring of invaginated enamel in the centre of the crown (Figure 3a). There appeared to be perforation or extreme thinning of the buccal plate adjacent to the apical third of the root (Figure 3b).
Figure 3.
(a) CBCT scan: one of the axial sections. Note the enlarged crown of the canine, the ring of enamel in the centre, surrounded by an annulus of radiolucent pulp tissue. (b) CBCT scan: one of the coronal sections. The enamel invagination is well demonstrated. Note the two hooked roots and the bone perforation near the tip of the larger, buccal root. The radiolucency associated with the roots is a radicular cyst. The radiolucent area above that is the normal nasal air space. (c) CBCT scan: one of the sagittal sections. This view most closely resembles the conventional periapical radiograph. The canine crown alone appears almost normal. Its two-angled roots give the erroneous impression of resorbing the UL4 root. The maxillary antrum is showing a slightly thickened mucosal lining, which is a frequent observation.
The definitive diagnosis of an erupted dilated odontome UL3 with an associated radicular cyst was made. Owing to the complex root anatomy, the patient was advised that the prognosis of the UL3 was poor and arrangements were made for extraction under general anaesthetic.
Surgical extraction of the UL3 was carried out by raising a full thickness buccal flap with a relieving incision distal to the UL4. There was obvious perforation of the buccal plate. The odontome was divided into three pieces and elevated (Figure 4). The cyst was enucleated and cyst cavity irrigated with saline. The flap was closed with 4/0 vicryl rapide sutures. The tooth fragments and soft tissue were sent for histopathology.
Figure 4. The dilated odontome was surgically sectioned and removed.
At the post-operative review 2 weeks later the area was healing well. Histopathological analysis confirmed a diagnosis of a dilated odontome together with a radicular cyst.
Four months after healing a resin-bonded bridge was provided using the UL4 as the abutment tooth to replace the UL3 (Figure 5). Although this is a definitive restoration it allows the patient to consider osseointegrated implants after his teenage years.
Figure 5. A resin-bonded bridge was provided at 4 months after surgery to replace the UL3.
Discussion
The assessment of the odontome, its pulpal morphology and relationship to surrounding structures, is not easy from conventional dental radiography, ie periapical, occlusal and panoramic radiographs. Being two-dimensional images, they do not provide enough information about this 3D structure, thereby preventing the clinician from making an accurate appraisal. A CBCT scan has, in this case, proved invaluable by allowing visualization of the complex anatomy in numerous thin slices in different planes of section. Not only did the scan help diagnose the type of dens invaginatus but, by showing the complex root shape, it confirmed the futility of further attempts at endodontic treatment. The scan facilitated the planning of surgical treatment by showing the location of divergent roots, whether root curvatures were favourable, and alerting to the possible presence of perforation of the buccal bone. Such accurate pre-operative assessment helped to minimize surgical trauma and to shorten operation time.
Although CBCT imaging has the disadvantage of increased radiation dose compared to conventional radiography, the additional information obtained here justifies its use in a young patient.
Conclusion
This case is of an unusual Type 3 dilated odontome of a canine and its management. CBCT imaging was extremely useful in accurately assessing the complex root anatomy and the adjacent structures.