Kershaw S, Newton J, Williams D The influence of tooth colour on the perceptions of personal characteristics among female dental patients: comparisons of unmodified, decayed and ‘whitened’ teeth. Br Dent J. 2008; 204
Tjan A, Miller G, The J Some esthetic factors in a smile. J Prosthet Dent. 1984; 51:24-28
Riskwise UK ‘Veneers’. Risk management from Dental Protection. 2001; 41:2-4
Chalifoux P Practice made perfect; perception esthetics: factors that affect smile design. J Esthet Dent. 1996; 8:189-192
Jornung J, Fardal O Perceptions of patients' smiles. A comparison of patients' and dentists' opinions. J Am Dent Assoc. 2007; 138:1544-1553
Fradeani M ‘Facial Analysis’.London: Quintessence Books; 2004
Ricketts R Planning treatment on the basis of the facial pattern and an estimate of its growth. Angle Orthod. 1957; 27:14-37
Ahmad I Anterior dental aesthetics: facial perspective. Br Dent J. 2005; 199:15-21
Davis N Smile Design. Dent Clin N Am. 2007; 51:299-318
Vig R, Brundo G The kinetics of anterior tooth display. J Prosthet Dent. 1978; 39:502-504
Aiamon J Assessment of periodontal treatment needs. Adaptation of the WHO Community Periodontal Index of Treatment Needs (CPITN) to European conditions. Public health aspects of periodontal disease in Europe.Berlin: Quintessence Verlag; 1983
Mehta SB, Banerji S, Millar BJ, Saures-Fieto JM Current concepts in tooth wear managements. Part 1: Assessment, treatment planning and strategies for the prevention and passive monitoring of tooth wear. Br Dent J. 2012; 212:(1)17-27
Dong J, Jin T, Cho H, Oh S The esthetics of the smile: a review of some recent studies. Int J Prosthodont. 1999; 12:9-19
Moore T, Southard K, Casko J, Qian F, Southard T Preliminary study on Invisalign tray fabrication. Am J Orthod Dentofacial Orthop. 2005; 127:208-213
Ahmad I Anterior dental aesthetics: dentofacial perspective. Br Dent J. 2005; 199:81-88
Dias N, Tsingene F SAEF – Smile's Aesthetic Evaluation Form: a useful tool to improve communication between clinicians and patients during multidisciplinary treatment. Eur J Esthet Dent. 2011; 6:160-175
Fradeani M ‘Gingival Analysis’.London: Quintessence Books; 2004
The flux of patients seeking to make changes to the appearance of their smile zone appears to be on a pathway of continual increase. This is possibly due to an increase in awareness towards oral health, and perhaps social, peer and media pressures, respectively. Cohorts of dental practitioners have thus responded to the latter demands by attending a plethora of educational courses, often focusing on either restorative techniques or other disciplines, notably orthodontics and clear aligners in particular. Consequently, treatment planning and thus treatment provision may carry the risk of being biased or indeed ‘outcome driven’, whereby the skills and knowledge of any clinician towards a particular faculty may significantly influence the ultimate treatment plan, with the unfortunate tendency sometimes to overlook the role of the interdisciplinary approach of concomitant restorative and contemporary techniques. The role of orthodontics to facilitate the provision of such treatment, along with predictable enamel bonding, has the distinct advantage of providing an acceptable aesthetic result with minimal biological intervention. However, to achieve an optimal result in such cases requires meticulous treatment planning and patient selection to avoid pitfalls with regards to long-term stability and function. This article suggests a standardized approach to patient assessment, with an interdisciplinary perspective in mind.
Clinical Relevance: With the growth of patient demand for improving the appearance of the smile, a meticulous assessment protocol is required along with effective interdisciplinary communication. This enables a comprehensive treatment plan to be developed with the correct priorities.
Article
The term ‘Aesthetics (esthetics)’ is derived from the Greek ‘aisthanomai’ meaning ‘I perceive, feel, sense’ and has been defined as ‘a branch of philosophy dealing with the nature of beauty, art and taste, and with the creation and appreciation of beauty’. (Webster Dictionary).
The appearance of the smile and teeth (perhaps collectively better referred to as the’ aesthetic zone’ or the ‘smile zone’) are clearly important factors in determining the attractiveness of a face,1 as well as having a key role with non–verbal communication.2 Indeed, it has been postulated that any given individual with a more beautiful external appearance may have a clear advantage over his/her peers and colleagues when considering acceptability in a social and/or occupational setting.1 It therefore comes as little surprise that there has been a surge in demand by patients seeking treatments, which have been commonly referred to in the broader medias as ‘smile makeovers’.
Dental practitioners have responded to the demands placed on them by their patients by acquiring the necessary restorative and or orthodontic skills so as to carry treatments to the aesthetic zone.
However, all too often when planning smile enhancement, the temptation to resolve any given issue by attempting to best fit a clinical problem to a ‘pre-determined solution’ (be that of either restorative or orthodontic variety, whichever may appeal to the strengths of a given operator), carries the consequences of poor functional and thus prognostic outcome, without often giving due consideration to all of the possible treatment options. Indeed, it was reported in 2011, by Dental Protection Limited, that there had been a significant increase in the number of complaints involving smile makeover treatments since 2006, with one case being reported to be settled for £150,000.00 (excluding legal costs)!3
Ambiguity also exists over what may be considered to be the ‘aesthetic dental ideal’, as the latter encompasses the concepts of beauty. Beauty is a highly subjective concept, influenced by a multitude of factors. It is beyond the scope of this article to discuss these factors, however, there are some ‘universally agreed concepts’ relating to the appearance of the smile zone, which include the features of morphology, proportion, symmetry, harmony, tooth position(s), colour variations and, of primary importance, the need to eliminate disease, which the dental practitioner should have a clear appreciation of when planning smile enhancements.
The aim of this article is to propose such a universal assessment protocol, the aim being to assist practitioners to plan the provision of care in a problem-based manner on the basis of the derived diagnosis. The role of interdisciplinary treatment planning and provision, respectively, will also be discussed.
Patient assessment: history and examination
There are three categories of ‘dental aesthetic imperfections’ for which the patient may seek dento-facial aesthetic intervention; these relate to anomalies in tooth colour, shape and position.4 With patients having increasing knowledge over possible facial aesthetic treatments, it may not be considered unusual for a patient to attend a dental practice expressing a concern relating to a facial aesthetic anomaly. The use of a preliminary aesthetic evaluation template, as described by Jornung and Fradal,5 may prove to be a highly beneficial tool in evaluating patients' perceptions of their dento-facial aesthetics. A detailed history relating to unstable dental disease should also be noted.
A contemporaneous medical history must be recorded. A patient's medical history may not only have an aetiological role for the underlying dental pathology observed, but it may also prohibit the provision of various dental treatments or, indeed, require modification of the treatment plan. The patient's dental history (including as assessment of attitudes towards dentistry and motivational levels), social and family history, respectively, must be attained and recorded.
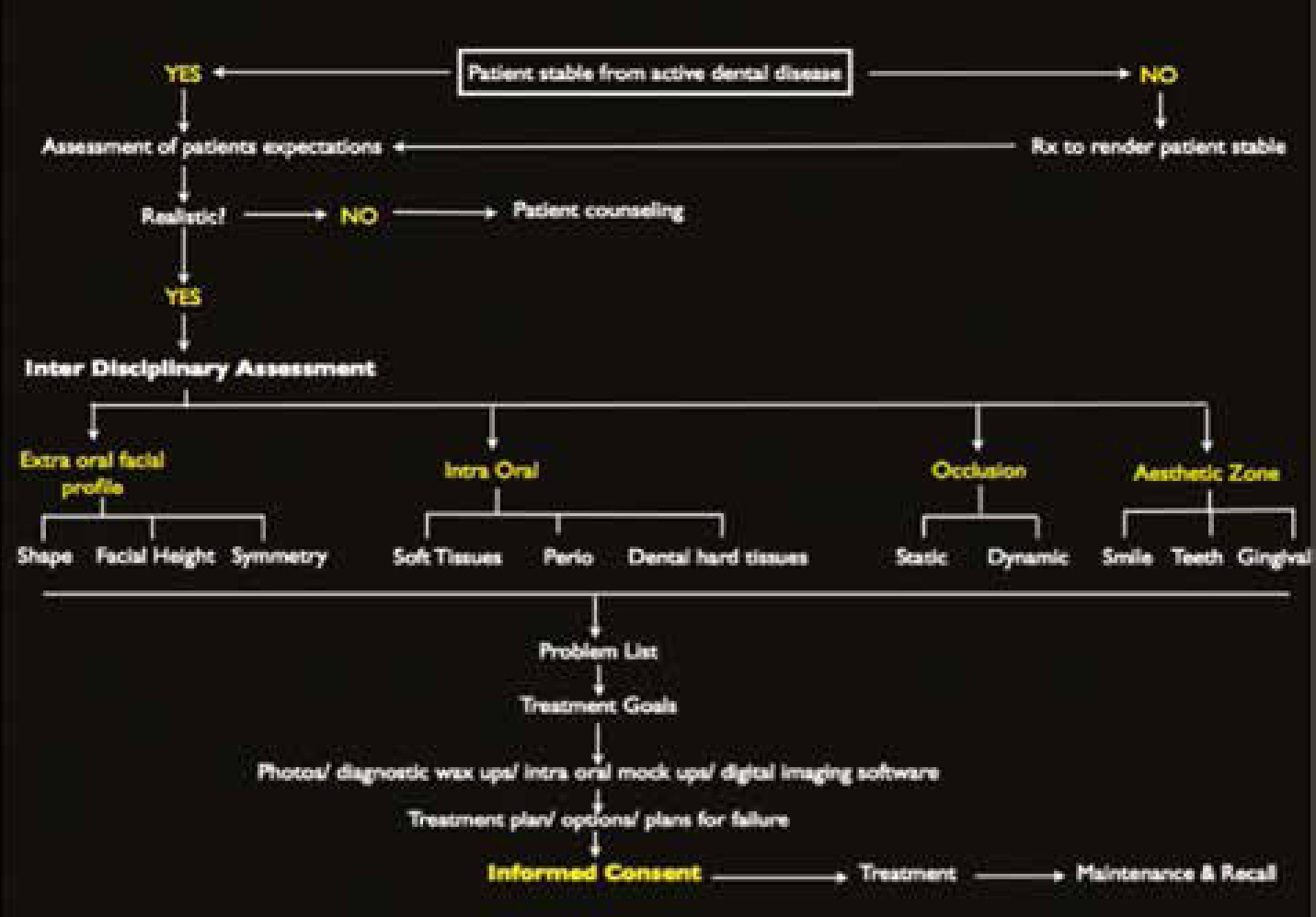
A detailed extra-oral examination should include an evaluation of the temporomandibular joints and associated musculature, cervical lymph nodes, facial features, lips (morphology and mobility) and facial skin. Figure 1 is an example of a flow diagram which may prove helpful when undertaking a comprehensive patient assessment.
Figure 1. A template flow diagram for undertaking a patient assessment.
The facial features which should be assessed as part of a comprehensive dental assessment include the:
Vertical facial proportions;
Facial symmetry;
Facial profile;
Facial shape and width.
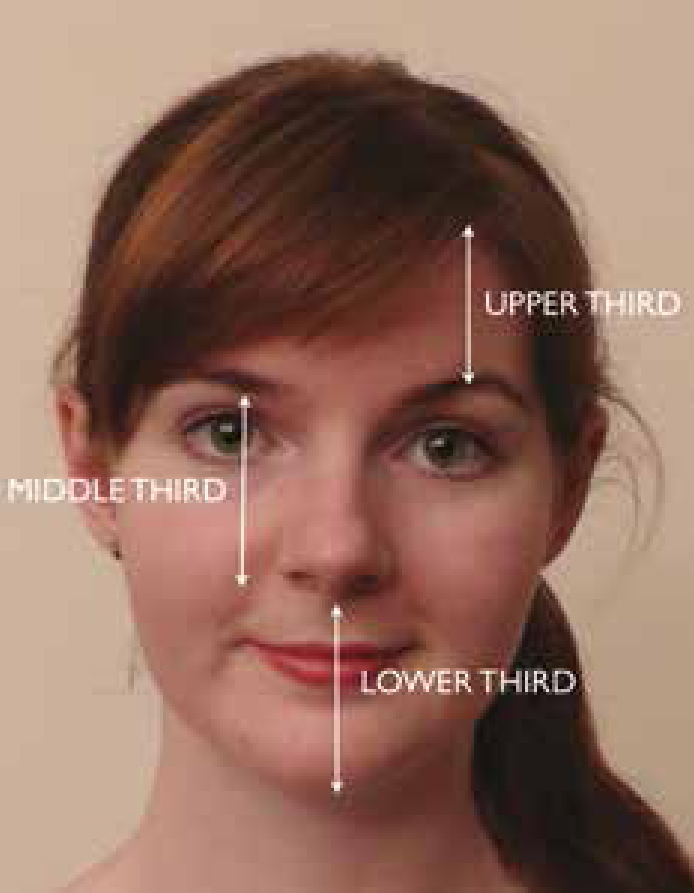
As depicted in Figure 2, the human face when viewed from a frontal direction can be divided into three zones; the ‘upper third’, which includes the area between the hairline and the ophriac line (brow line); the ‘middle third’, which ranges from the ophriac line to the interalar line (base of the nose); and the ‘lower third’, which includes the area between the interalar line and the tip of the chin.6 The lower third region appears to be the most significant in determining the overall facial appearance, and is the zone over which the dental operator has the most control.6
Figure 2. The zonal division of the face when viewed from the front. Three zones: upper, middle and lower.
When considering facial symmetry, the facial midline (imaginary line connecting the nasion to the base of the philtrum) and the interpupillary line are the most commonly applied vertical and horizontal reference planes, respectively. It is generally accepted that aesthetic harmony is attained where the vertical and horizontal reference planes are perpendicular to each other, and that the dental midline is co-incident with the facial midline.6 The interpupillary line provides the operator with a key reference axis in determining the ultimate position of the incisal, gingival and occlusal planes, respectively. However, caution needs to be exercised where the interpupillary line may be canted, where the horizon is better applied as the horizontal reference plane.6
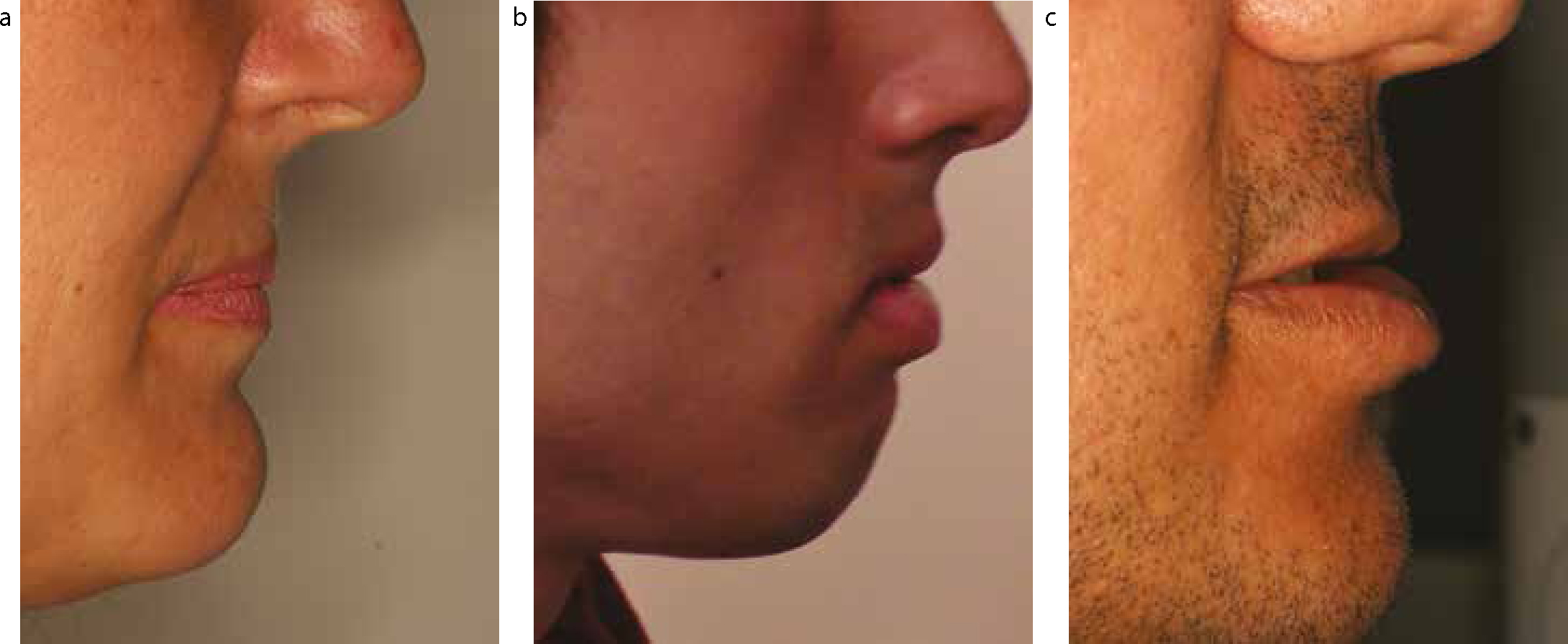
The lateral facial profile is most appropriately assessed with the patient adopting a natural head posture. Three forms of facial profile have been described in the contemporary literature, as shown by Figure 3:
It is important to develop the information regarding the forms of the facial profile with the skeletal relations of the maxilla and mandible. This allows for a comprehensive overview of the facial form in terms of the skeletal relationship as Class I, Class II and Class III. Combining this classification with information such as the naso-labial angle and chin (pogonion) point allows the clinician to be thinking of orthodontics to compensate for any skeletal discrepancies or to realize the limitations of an ideal result.
The ‘E-line’ (formed by connecting the tip of the nose to the tip of the chin) is also commonly applied to determine facial profile. A’ normal profile’ is thought to exist where the upper lip and lower lip are 4 mm and 2 mm, respectively, posterior to the E-line;7 however, it is necessary to accommodate the impact of racial and gender variations to such numerical guidelines.
Classically, four types of basic facial shape had been described in the literature:
Ovoid;
Square;
Tapering;
Square-tapering (Leon Williams Classification).
The above classification system has historically been used to determine appropriate moulds for removable denture prosthesis, albeit on a purely arbitrary basis. Ahmad,8 in more recent times, has described four typological categories to which to ascribe a particular facial shape. These are:
Lymphatic (rounded full features with a timid personality);
Sanguine (prominent thick well-defined features associated with intransigence and spontaneity);
Nervous (large forehead, thin delicate features with an anxious disposition);
Bilious (rectangular and muscular features coupled with a dominant persona).
Facial width may be assessed crudely by estimating this dimension in accordance with the typical width of an eye; with the width of ‘5 eyes’ often accepted as that of a normal facial width.9
The lips should be analysed for their morphology and level of mobility, noting the width, fullness (thin, medium or thick) as well as symmetry of the lips. In general, wide lips make way for a wide smile; a smile that is at least half the width of the face is considered to be aesthetically pleasing.9 Associations have been made between fullness and personality traits.
Lip mobility refers to the amount of lip movement that occurs when a patient smiles. The amount of anterior tooth display should be determined with the lips both in a rest position and dynamic position. The rest position of the lips has been classically used to determine the position of the incisal edges of the anterior maxillary teeth, particularly with regards to complete denture prosthetics, and the level of incisal edge display has been shown to reduce with age.10
Phonetic tests, such as the enunciation of the ‘F’ and ‘V’ sounds, can help to verify the correct spatial relationship between the incisal edges of the anterior maxillary teeth and the lower lip. The length of the philtrum should also be determined; in general the philtrum height should be 2–3 mm shorter than the height of the commissures; younger patients often have a shorter philtrum height.
Facial skin types should be classified according to pigmentation, tendency to burn, and likelihood for reaction to treatment (in particular heat-based treatments such as that of lasers).
The intra-oral examination should include an assessment of:
The soft tissues;
The periodontal tissues;
The dental hard tissues;
Occlusion and arch form;
The aesthetic zone;
Any edentulous spaces.
The soft tissues of the oral cavity should be carefully analysed for the presence of any anomalies. The presence of a tongue thrust habit and/or a high frenal attachment may be of relevance when conducting a systematic assessment with a bias towards achieving ideal dento-facial aesthetics and stability.
Periodontal tissues should be carefully evaluated for the presence of any active disease and also to assess the potential impact any restorative care or orthodontic treatment may have upon the periodontal tissues. A patient's overall standard of oral hygiene should be ascertained (as being good, moderate or poor) as should the presence and extent of any plaque and calculus deposits. Orthodontic alignment can improve the ability to maintain better oral hygiene. The presence of any local factors which may further encourage plaque and calculus stagnation should also be noted (such as overhanging and defective restorations, respectively). It may also be worthwhile noting the presence and extent of extrinsic tooth stains.
A Basic Periodontal Examination (BPE)11 should be conducted on a routine basis. Where a score of 3 is recorded for two or more sextants, the undertaking of a full depth, six point periodontal chart is often indicated. It may also be worthwhile documenting the levels of attachment to determine the amount of periodontal destruction which may have taken place. Other periodontal features to note include:
The presence of any tooth mobility;
Presence and extent of gingival recession;
Furcation involvement(s);
Bleeding on probing, loss of stippling, swelling, erythema;
Plaque scores, bleeding scores;
Pus discharge and presence of any exudates.
Charting of the dental hard tissues should record the presence (or absence of teeth), dental caries, dental restorations (including failed restorations), tooth fractures, cracks, wear lesions (of an abrasive, erosive, attritional or abfractive variety), presence of food traps and any tooth malformations which may be present.
It is paramount to carry out a detailed occlusal and arch form assessment, noting not only static features, but also dynamic occlusal. The ultimate success of treatment by restorative, orthodontic or interdisciplinary intervention is in part based on providing the patient with a functionally stable occlusal scheme. The static occlusal examination should take note of the presence of any of the following features in a systematic manner which can be reproduced easily:
Incisor relationship (Class I, Class II div 1, Class II div 2, Class III);
Overjet measured in mm;
Overbite (normal, increased deep bite, decreased complete, open bite);
Molar and canine relationships;
Upper and lower centrelines in relation to facial midlines;
The assessment of the features listed will help to establish the presence of any malocclusions, and further categorize the inter-arch occlusal relationships (such as the incisor, canine and molar segment classifications).
A freeway space (FWS) assessment should be undertaken, particularly where the patent presents with a worn dentition.
The dynamic occlusal examination should commence with first establishing the intercuspal position (ICP), also commonly referred to as the maximal intercuspal position (MIP) or centric occlusion (CO) in the dental literature.
The ease with which the mandible can be manipulated into its retruded arc of closure should also be established. Centric relation (CR) refers to the maxilla-mandibular relationship at the point where the condyles are located in the most anterior-superior position in the glenoid fossae. The retruded contact position (RCP) in this context refers to the first tooth contact that occurs in CR.
It is generally accepted that CR offers a fixed occlusal position that can be repeatedly reproduced on an appropriate form of dental articulator. Whilst, physiologically, a small proportion of cases will display no disparity between ICP and RCP, for the majority of patients there will exist a slide between these two occlusal positions. The presence of such a slide, together with its magnitude (in both the horizontal and vertical dimensions) and the RCP contact itself should be documented.12
It is important to document the anterior guidance. Where the occlusal scheme is considered to be stable (mutually protective), when the patient displays a protrusive mandibular movement, the contact formed between the palatal surfaces of the anterior maxillary teeth and their antagonists, coupled with the inclination of the condylar path, should collectively aim to separate (or disclude) the posterior teeth from each other, thereby avoiding any harmful occlusal contacts. The steepness of the anterior guidance provided by the anterior teeth should also be recorded, as being steep, moderate or shallow.
Occlusal contacts when undertaking mandibular lateral excursive movements should also be determined. Lateral guidance may be provided by the canine teeth ‘canine guidance’ or by the posterior teeth ‘group function’. The presence of any occlusal interference on either the working side or non-working side should also be noted. The use of articulated study casts to analyse the patient's occlusion may serve as an invaluable tool.12
The aesthetic zone
Analysis of the aesthetic zone should aim to evaluate the following features:
Dento-labial relationships;
Dental midlines;
Tooth colour, texture and form;
Tooth size, proportion, shape, symmetry, position and axial inclination;
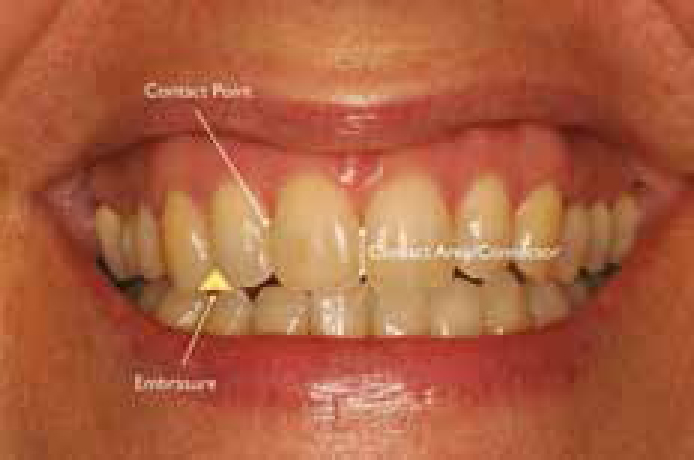
Contact areas, connectors and embrasures (Figure 8);
Gingival aesthetics;
Diagnosis and treatment planning.
Dento-labial relationships
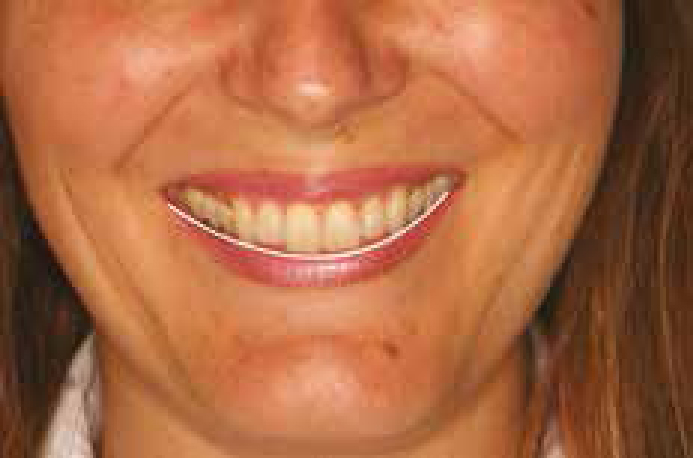
The term ‘lip line’ or ’smile line’ refers to the relationship that exists between the inferior border of the upper lip and the teeth and gingival soft tissues on smiling (or when asked to make the ‘E’ sound). Three types of lip line are commonly described (Figure 4):2
‘Low smile line’: where the motility of the upper lip exposes the anterior teeth by no more than 75%, with no display of gingival tissue; (low smile lines can be the most forgiving in cases of restorative imperfections);
‘Medium smile line’: where lip movement culminates in the display of between 75% and 100% of the anterior teeth as well as the interdental papillae;
‘High smile line’: which exposes the teeth in full in display as well as the gingival tissues beyond the gingival margins, often referred to as ‘gummy smile’.
Figure 4. Examples of ‘low’, ‘medium’ and ‘high’ smile lines.
The ‘width of the smile’ should also be analysed. It is has been reported that a smile displaying 10 maxillary teeth (up to and including the second premolar teeth) is the most observed common smile width pattern.13 It has been shown that, for optimum aesthetics, the dental hard tissues should fill the corners of the mouth to produce a ‘full smile’, thus avoiding the presence of ‘negative buccal corridors’.14
The ‘smile arc’ should also be evaluated. The latter refers to the relationship between curvatures of the lower lip to the curvature of the incisal edges of the maxillary incisor teeth in a posed smile (Figure 5). Ideally, the curvature of the lower lip should be parallel to that of the incisor edges and the superior border of the lower lip should be spatially positioned slightly inferior to the incisal edges.
Figure 5. The concept of the smile arc.
Dental midlines
Ideally, the dental midline should coincide with the facial midline. The maxillary centreline is best assessed against the midpoint of the philtrum. It has been shown that the labial frenum and facial midline are co-incident in approximately 70% of the population.14 A discrepancy of up to 2 mm between the maxillary midline and facial midline is generally considered to be aesthetically acceptable. The mandibular midline should ideally be coincident with the maxillary midline. However, the latter has been observed to occur physiologically only amongst 25% of the population.15
Tooth colour, texture and form
Tooth colour and texture
Teeth should be evaluated for variations in colour, thus their:
Hue – basic colour;
Chroma – saturation of the basic colour;
Value – brightness.
Features such as surface texture and lustre should also be documented, particularly when planning indirect restorations. A colour assessment is most effectively undertaken at the beginning of the visit whilst the teeth are hydrated and to avoid eye fatigue. The patient should be at eye level, as such to make optimal use of the colour sensitive part of the retina. Natural daylight is ideal, following an initial assessment using incandescent or fluorescent lighting.
Tooth form
The form of the maxillary central incisors (ovoid, square or triangular) has been suggested (without any scientific basis) to reflect on the personality, sex, age, and strength index of a particular individual. Tooth form may also alter with age as a result of toothwear.
Tooth size, proportion, shape, symmetry, position and axial inclination
The size, shape and the arrangement of the maxillary anterior teeth are considered by many to be the most significant factors in contributing to a harmonious anterior dentition.
Tooth proportion, shape and size
The maxillary central incisor teeth are generally accepted as the most dominant teeth in the aesthetic zone, with reported average lengths and widths of between 10 and 11 mm and 8 to 9 mm, respectively;16 suggestive of height to base ratio of 1.2:1. It is also frequently stated that the central incisor length should be approximately one-sixteenth of the facial height. In cross-sectional profile these teeth usually present with two or three planes on the labial face. Over-contouring in the labial-gingival portion (frequently seen as consequence of restorative intervention) results in not only poor aesthetics, but also the initiation of periodontal disease. Attention should also be given to the morphology of the central incisors in the frontal plane; seldom are central and lateral incisors ‘flat’ when viewed facially.
Symmetry, position and axial inclination
The concept of the ‘Golden Proportion’ was first introduced to the dental profession by Lombardi in 1973.17 The latter mathematical concept suggests an ideal proportion of 1:1.618. In the context of the anterior maxillary dentition this would imply that the maxillary central incisor should be 1.618 times wider than the maxillary lateral incisor, which in turn would be 1.618 times wider than the maxillary canine when viewed from a frontal direction18 (Figure 6). The width of the maxillary canine according to this concept should be 62% of the width of the lateral incisor, which itself would be 62% of the width of the maxillary central incisor, respectively. However, the Golden Proportion has been shown to exist in just under a fifth of all natural dentitions examined,19 and thus this concept must be applied with extreme caution when planning dental treatment.
Figure 6. The Golden Proportion.18
Minor levels of asymmetry between the maxillary central incisors are more commonly observed to occur than the existence of perfect symmetry. It is also desirable for the morphology of the disto-incisal line angles of the anterior maxillary teeth to have a symmetrical appearance. The presence of peg-shaped lateral incisors or, indeed, absent teeth may have a profound effect on the symmetrical arrangement of the anterior maxillary region.
When viewed from a front direct, the anterior maxillary teeth have a tendency towards a mesial tilt or inclination towards the vertical midline (Figure 7). The angle of inclination increases in moving laterally from the central incisors to the canines. A noticeable lack of symmetry in the axial inclination of the anterior teeth may culminate in a poor aesthetic appearance.
Figure 7. Axial inclination of anterior maxillary teeth, displaying symmetry about the midline.
Contact areas, connectors and embrasures (Figure 8)
Figure 8. The concept of ‘contact areas’, ‘connectors’ and ‘embrasure spaces’.
Embrasure spaces should ideally increase in size in progressing distally away from the midline.20 Similarly, contact points should be positioned in a more apical location when moving distally from the midline in a symmetrical manner. The connector may be defined as the ‘area between two adjacent teeth that seem to touch in a frontal view.’20 Dias and Tsingene21 have suggested the application of the ‘50-40-30’ rule in defining the aesthetic relationship between the anterior maxillary teeth, whereby the ideal connector area between the central incisors is 50% of the length of their clinical crowns, between the central incisor and lateral incisors is 40% of the length of the crown of the central incisor, and 30% of the length of the central incisor tooth between the lateral incisor and canine teeth, respectively. Connectors should ideally be symmetrical across the dental midline.
Gingival aesthetics
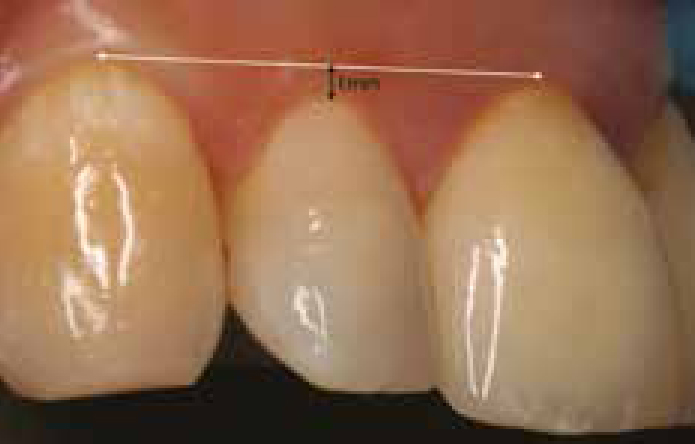
The gingival levels of the anterior maxillary segment should ideally be symmetrical about the midline, with the horizontal gingival levels of the central incisor and canine teeth being placed slightly more apical (by approximately 1 mm) than that of the lateral incisors (Figure 9). The gingival biotype should also be determined (sub classified as being thick or thin), as this may influence how the gingival tissues may respond to surgical procedures or to the placement of future dental restorations. In general, thin biotypes are associated with triangular tooth forms, whilst thick biotypes are commonly associated with the presence of square tooth forms.22
Figure 9. The concept of the desired horizontal gingival levels.
Diagnosis and treatment planning
Having undertaken a comprehensive patient assessment, the next stage involves the formulation of a diagnosis or a ‘problem list’. The latter should include details beyond pathological anomalies which the patient may present with, such as the presence of any aesthetic parameters which may display deviation from ‘universally accepted concepts’ relating to dento-facial aesthetics, eg symmetry, proportion, size, shape and position (as discussed above). It should also take into consideration subjective matters relating to concepts such as colour.
On the basis of the established problem list, the dental operator can begin to assemble an appropriate treatment plan. An aesthetic assessment in current practice requires a thorough foundation understanding of not only restorative dentistry, but also in orthodontics, periodontology and implantology. Only then can a comprehensive overview be assembled which will allow the aesthetic dentist to warrant the need of other specialist involvement or assess whether the case can be handled by a single clinician.
Effective treatment planning for any given scenario is often dependent on the clinician adhering to well established protocols. In this instance, priority should be given to the management of any acute conditions, followed by preventive advice and care, stabilization, simple definitive restorations, complex definitive restorations and, finally, the monitoring and maintenance phase, with periodic reviews between each phase to assess the efficacy of care and patient compliance.
The operator should aim to attain the desired agreed aesthetic outcome, whilst maintaining the patient in a functionally stable state of oral health, so as to optimize longevity of care. Where possible, the least invasive treatment protocols should be adopted. It is at the latter juncture where orthodontic treatment for the adult patient is all too often overlooked by the operator. Orthodontic intervention may be able to fulfil the aims of treatment with minimal irreversible biological cost (without the need for any invasive subtractive restorative involvement) or, indeed, may act as a very suitable adjunct to definitive restorative care, so as to attain optimal outcome with concomitant conservation of the dental hard and soft tissues, respectively. Table 1 includes a list of scenarios where pre-restorative orthodontics may help to attain the most desirable outcome with a view to optimal function, aesthetics and biological conservation.
Group 1:Indications for Pre-RestorativeAdult Orthodontics
Spacing, crowding and alignment corrections;
Opening spaces for restorations including implants;
Uprighting of tilted teeth;
Intrusion of over-erupted teeth;
Extrusive movements.
Group 2:General Malocclusions
Large overjet corrections;
Vertical discrepancy management; deep bite.
Group 3:Improving and Maintaining Occlusal Stability
Orthodontics can be used alone or in conjunction with occlusal equilibration and prosthodontic correction to aid in fulfilling requirements for long-term occlusal prosthodontic correction to aid in fulfilling stability.23
It is at this point that alternative treatment options will be offered to the patient. The pros and cons can be discussed and, with informed consent, a treatment plan can be chosen. It is important to appreciate that the treatment goals in adults may be compromised if only a restorative approach or only a short-term orthodontic solution is offered.
Conclusion
The need to conduct a detailed patient assessment is absolutely pivotal in helping to create a holistic problem list. The latter should be approached in a logical manner, aiming to stabilize pathology in the first instance. The desire to fulfil the expectations of any patient, when concerning aesthetic changes, should involve the need to consider all possible treatment regimens, and an appropriate, consented choice made, based on what is most likely to achieve the desired result with optimum function, stability and biological tissue conservation in mind. The temptation to apply a premeditated solution to a given situation should be avoided where possible.