Bernard JP, Schatz JP, Christou P, Belser U, Kiliaridis S Long-term vertical changes of the anterior maxillary teeth adjacent to single implants in young and mature adults. A retrospective study. J Clin Periodontol. 2004; 31:1024-1028
Cronin RJ, Oesterle LJ, Ranly DM Mandibular implants and the growing patient. Int J Oral Maxillofac Implants. 1994; 9:55-62
Strietzel FP, Reichart PA, Kale A Smoking interferes with the prognosis of dental implant treatment: a systematic review and meta-analysis. J Clin Periodontol. 2007; 34:523-544
Van der Weijden GA, van Bemmel KM, Renvert S Implant therapy in partially edentulous, periodontally compromised patients: a review. J Clin Periodontol. 2005; 32:506-511
Tarnow DP, Magner AW, Fletcher P The effect of the distance from the contact point to the crest of bone on the presence or absence of the interproximal dental papilla. J Periodontol. 1992; 63:995-996
Heitz-Mayfield LJ, Huynh-Ba G History of treated periodontitis and smoking as risks for implant therapy. Int J Oral Maxillofac Implants. 2009; 24:39-68
Hebel KS, Gajjar R Achieving superior esthetic results, parameters for implant and abutment selection. Int J Dent Symp. 1997; 4:42-47
Woelfel JB, 4th edn. Philadelphia: Lea and Febiger; 1990
Hammerle CH, Chen ST, Wilson TG Consensus statements and recommended clinical procedures regarding the placement of implants in extraction sockets. Int J Oral Maxillofac Implants. 2004; 19:26-28
Schropp L, Wenzel A, Kostopoulos L, Karring T Bone healing and soft tissue contour changes following single-tooth extraction: a clinical and radiographic 12-month prospective study. Int J Periodont Restor Dent. 2003; 23:313-323
Araújo MG, Lindhe J Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005; 32:212-218
Esposito M, Grusovin MG, Polyzos IP, Felice P, Worthington HV Timing of implant placement after tooth extraction: immediate, immediate-delayed or delayed implants? A Cochrane systematic review. Eur J Oral Implantol. 2010; 3:189-205
Evian CI, Rosenberg ES, Coslet JG, Corn H The osteogenic activity of bone removed from healing extraction sockets in humans. J Periodontol. 1982; 53:81-85
Evans CD, Chen ST Esthetic outcomes of immediate implant placements. Clin Oral Implants Res. 2008; 19:73-80
Buser D, Halbritter S, Hart C Early implant placement with simultaneous guided bone regeneration following single-tooth extraction in the esthetic zone: 12-month results of a prospective study with 20 consecutive patients. J Periodontol. 2009; 80:152-162
Choquet V, Hermans M, Adriaenssens P Clinical and radiographic evaluation of the papilla level adjacent to single-tooth dental implants. A retrospective study in the maxillary anterior region. J Periodontol. 2001; 72:1364-1371
Kourkouta S, Dedi KD, Paquette DW, Mol A Interproximal tissue dimensions in relation to adjacent implants in the anterior maxilla: clinical observations and patient aesthetic evaluation. Clin Oral Implants Res. 2009; 20:1375-1385
Patients who suffer dento-alveolar trauma present a unique challenge for the dentist. There are numerous options to consider when attempting to restore the dentition. This article reviews the role of dental implants and how thorough planning and execution of such treatment could result in an optimal outcome.
Clinical Relevance: Knowledge of the role of dental implants and factors imperative for a successful treatment outcome will assist the clinician in achieving optimal restorative results.
Article
To date, there are no research studies that have specifically looked at the success and survival rates of implants in trauma patients. It is therefore assumed that the success rates are similar to implants placed in non-trauma patients. With that, the variables to take into account are identical to regular implant placement. There may, however, be an increased likelihood for the requirement of supplemental surgical techniques if anatomical deficiencies still exist after trauma, which have been discussed in the previous article.
Implant treatment planning considerations
When dental implants are contemplated in patients, the clinician should consider the following clinical parameters which will guide the treatment process and influence the outcome. These include:
Age;
Patient expectations;
Smoking habits;
Height of the smile line;
Gingival tissue biotype;
Shape of the teeth (missing and present);
Presence of infection;
Hard and soft tissue width and height availability;
Character of the edentulous space.
Age
The age of the patient is important when considering implants in young and still growing individuals. With increasing age there is continued vertical growth of the alveolar processes. Unlike a tooth, a dental implant osseointegrates and essentially is ankylosed to the bone. Therefore, implants placed in the growing patient will suffer from relative infra-occlusion1 where the surrounding structures continue their normal growth while the implant maintains its original position and appears to submerge.
For this reason, it is generally recommended that dental implants are not placed until substantial cranio-facial growth has completed up until around 18 years of age, though male growth tends to finish at a slightly later stage compared with females.2,3 It must be emphasized that facial growth tends to continue into later years, albeit minimally, yet it may have aesthetic consequences which should be discussed with the patient prior to placing implants, particularly in the aesthetic zone.
Owing to the reasons discussed in the previous article, it is our view that extraction of anterior teeth in a growing patient, which mainly tend to result as a consequence of trauma, should be considered with extreme caution. Therefore, every attempt at preserving the alveolar ridge to facilitate future implant placement should be given due consideration. Intervention at the time of extraction, as illustrated in the previous article, might avoid reliance on block bone grafting, thereby minimizing patient morbidity and the cost of treatment.
Patient expectations
Patient expectations should be evaluated from the outset. If expectations are unrealistic, the patient may be considered a ‘high aesthetic risk’. A thorough assessment will identify the risks and clinicians may be best served by discussing all limitations and complications that may occur during the procedure in an attempt to lower expectations to a more realistic level. These can include inability to reproduce lost hard or soft tissues fully, potential scarring and the recovery after an oral surgical procedure.
Smoking habits
The evidence clearly shows that smoking has a negative impact on the long-term success of dental implants.4 It is imperative that patients are at least aware of the biologic complications that may occur with continued smoking, and these should be part of a written consent. It is up to the dentist's clinical opinion whether to refuse dental implant treatment altogether.
Height of the smile line
The smile line can be low, medium or high (Figure 1) and will dictate to what extent the surgical site will be visible. High smile lines will display both the teeth and a large portion of the surrounding soft tissues and so are considered a higher aesthetic risk. Low smile lines will cover most of the surgical site and afford the clinician some leeway.
Figure 1. Low, medium and high smile lines.
Gingival tissue biotype
Gingival biotype (thin, medium or thick) has become increasingly more important to observe during evaluation. Thin biotypes are considered higher risk given an increased propensity for gingival recession. Thicker biotypes are more resistant to recession and can assist in masking the metallic hue of the underlying implant abutment. Clinical assessment is carried out using a periodontal probe. A thin biotype is one where the probe is easily visible through the gingival margin and also has a tendency to have a highly scalloped gingival contour (Figure 2).
Figure 2. Thin gingival biotype with high scalloping of gingival contour and probe shine through.
Shape of the teeth (missing and present)
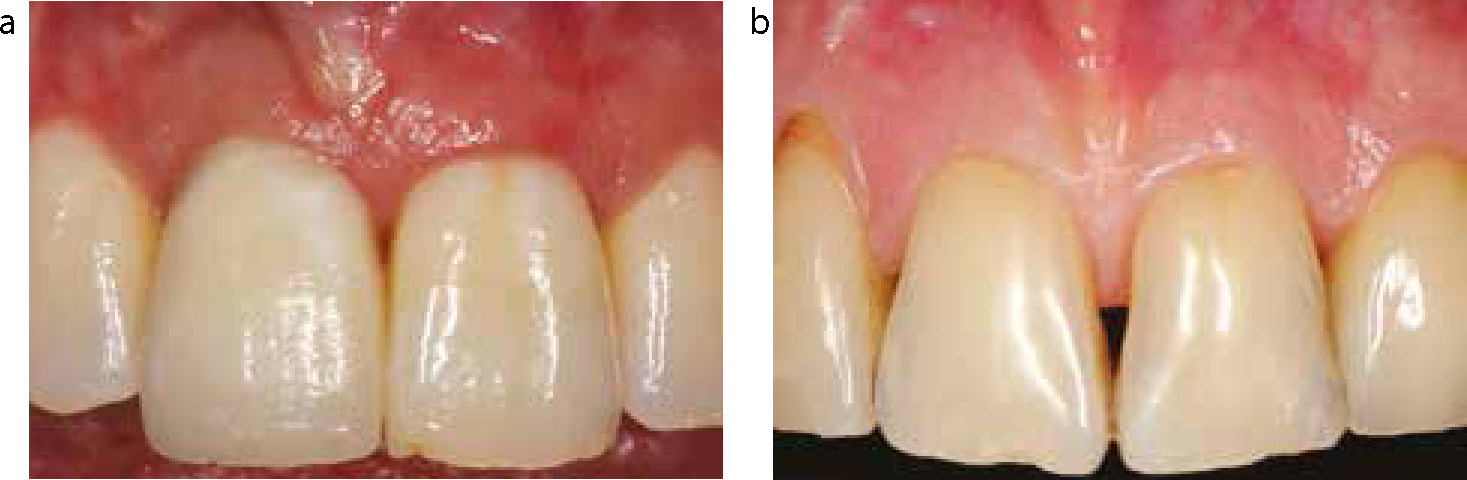
The shape of the teeth will affect the potential for an aesthetically pleasing result. Triangular-shaped teeth, with a coronal contact point and a long papilla are considered more of a risk as there is an increased likelihood of losing the interproximal papillae and so black triangles may become evident. On the other hand, square-shaped teeth have a longer, more cervical contact and a smaller papilla is needed to fill the embrasure space (Figure 3).
Figure 3.
(a) Square teeth with long contact and short papillae. (b) Triangular teeth with more coronal contact and expected long papillae.
Presence of infection
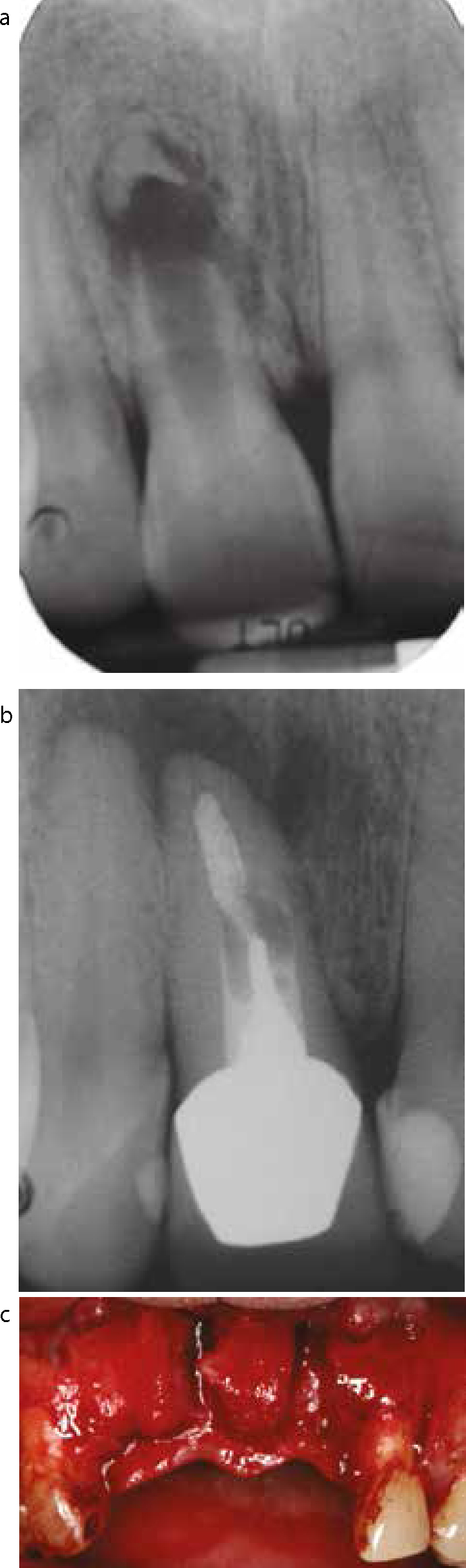
Infection can either be of endodontic or periodontal origin. Both must be assessed as they are considered potential risk factors for complications.5 Therefore, a thorough clinical and radiographic examination must be incorporated into the assessment. Infection causes bone resorption and, in the anterior maxilla, peri-apical infection tends to resorb labial bone, which can present as an apical fenestration or, at times, a large dehiscence may be present which further complicates implant treatment (Figure 4).
Figure 4.
(a) UR1 with root resorption and a large peri-apical infection. (b) UR1 with a failing post-crown and peri-apical infection. (c) Complete labial bone resorption as a result of chronic endodontic infection.
Periodontitis results in apical migration of the supporting alveolar bone and resorption of inter-proximal bone on adjacent teeth will consequently lead to loss of inter-dental papilla6 (Figure 5), which is impossible to regain. Besides, implant treatment is contra-indicated in patients with active periodontal disease and, furthermore, evidence seems to suggest a higher incidence of peri-implantitis in patients with a history of periodontitis,5 even if the disease process has been treated and stabilized.7
Figure 5. Periodontal disease with extensive loss of interproximal tissue.
Hard and soft tissue width and height availability
As mentioned in part 1, every effort should be made to maintain the hard and soft tissue width and height. These factors should again be assessed to determine if augmentation procedures are required prior, during or sometimes after implant placement.
Character of the edentulous space
Implant planning should be restoratively-driven and the examination should assess whether the space (in 3-dimensions) is adequate for replacement with a prosthetic tooth in an optimal position. Mesio-distal, bucco-palatal and the inter-occlusal space are the 3-dimensions of the edentulous space that should be assessed. Implant positioning based on availability of bone is a common reason for aesthetic and functional failure. A mesio-distal measurement will ascertain if the space is too wide or narrow, thus necessitating orthodontic intervention. If buccal alveolar ridge loss is not adequately augmented, it may result in an incorrect and more palatally positioned prosthesis. The occlusion will indicate if the space has been encroached upon by the opposing dentition, which may require tooth movement or adjustment by minor odontoplasty.
Implant treatment plan
After the above information has been elucidated, a definitive treatment plan can start to be formulated based on the following questions:
What?;
When?; and
Where?
What
Once the decision to replace the missing tooth with an implant has been made, the clinician has to choose what implant to place. The most important factors are the implant width and length.
Other factors include:
Surface characteristics (machined/smooth or rough implant surface)
- Machined implants have a reduced surface area compared with rough variants;
- Rough implants have higher survival compared with machined implants;
- Peri-implantitis is more prevalent and difficult to treat in rough implants.
Shape of the implant (parallel or tapered)
- Use of a tapered implant may allow placement in sites with adjacent root convergence;
- Tapered implants are indicated for placement in extraction sockets and offer greater primary stability.
Presence or absence of a collar (also referred to as ‘tissue level’ or a ‘bone level implant’)
- The machined collar of tissue level implant offers smooth surface for soft tissue attachment;
- The presence of a collar can compensate for vertical bone deficiency as the collar does not need to be surrounded by bone;
- The collarless implant can facilitate implant placement when mesiodistal space is limited.
Width
- Appropriate diameter implants allow for more favourable emergence profile production and optimal aesthetics, facilitate patient performed plaque control and reduce the chances of biologic complications. In certain circumstances the surrounding dentition may encroach on the residual space either coronally or apically, necessitating consideration of a smaller diameter implant or orthodontic treatment to recreate ideal space;
- Table 18,9 outlines the average mesio-distal width of the teeth as well as the mesio-distal width of the tooth 2–3 mm below the cemento-enamel a junction. These values should be taken into account when making a choice of implant diameter;
For example, a central incisor 2–3 mm below the cemento-enamel junction (CEJ) has a mesio-distal width of 5.5 mm. When replacing this tooth with an implant, a similar diameter should be used (eg 4–5 mm) in order to maintain at least 1–2 mm distance to adjacent teeth
Length
- Longer implants allow greater implant to bone surface contact and improved implant:crown ratios;
- Surrounding anatomic factors (eg floor of the nose, maxillary sinus, ID canal) will usually be the limiting factor for obvious safety reasons.
MAXILLA
Mesio-distal width at crown
Mesio-distal width 2–3 mm below CEJ
Central Incisor
8.6
5.5
Lateral Incisor
6.6
4.3
Canine
7.6
4.6
1st Premolar
7.1
4.2
2nd Premolar
6.6
4.1
1st Molar
10.4
7.0
2nd Molar
9.8
7.0
MANDIBLE
Mesio-distal width at crown
Mesio-distal width 2–3 mm below CEJ
Central Incisor
5.3
3.5
Lateral Incisor
5.7
3.5
Canine
6.8
4.1
1st Premolar
7.0
4.5
2nd Premolar
7.1
4.7
1st Molar
11.4
9.0
2nd Molar
10.8
8.5
When
If the patient is of an appropriate age for implants, the next decision to make is the timing of the surgery relative to the removal of the tooth. A consensus report10 classifies the timing of implant placement after extraction into four types:
Type 1 – implant is placed immediately following tooth extraction;
Type 2 – implant is placed 4–8 weeks post extraction in a site where soft tissues have healed and the mucosa covers the socket. Early bone remodelling would have occurred with resorption of the bundle bone;
Type 3 – implant is placed 12–16 weeks post extraction where an extraction site has considerable amounts of newly formed bone;
Type 4 – implant is placed more than 16 weeks after extraction when a site is fully healed.
The decision on timing should be based on a thorough understanding of the changes that occur to the hard and soft tissues following tooth loss. After a tooth has been removed, the alveolar walls of the socket resorb while the centre of the socket fills with cancellous bone. Ultimately, the volume of bone will reduce markedly. This reduction occurs not only in a bucco-lingual direction but also in a corono-apical dimension.11 As discussed in the previous article, up to 50% of ridge width reduction can be expected in a year with 30% being reported within the first three months after extraction.11
Soft tissue changes will involve an increased connective tissue volume which epithelializes and keratinizes and eventually covers the socket opening.
Advantages and disadvantages of different placement protocols:
Type 1 (extraction socket): Placement of an implant immediately after extraction reduces the number of surgical procedures and the overall treatment time. The amount of bone present is optimal as long as all the alveolar socket walls are maintained at the time of extraction. The morphology, however, may complicate placement and primary stability of the implant. This type of placement is technique-sensitive and achieving primary stability may be difficult given that the extraction socket will be larger than the implant diameter in most areas and primary stability is usually limited to an apical few mms above the root apex. An adjunctive surgical procedure may also be required.
Placement of an implant in an immediate extraction socket was previously thought to reduce the amount of bone resorption. However, studies12 have shown that this is not the case, and higher aesthetic complications have been reported.13 Immediate implant placement is at a higher risk of failure to integrate, aesthetic failure, and bundle bone resorption seems to interfere with successful guided bone regeneration (GBR).
Type 2 (4–8 weeks post extraction): There is an increase in the amount of soft tissue that would have now covered the socket entrance. This can facilitate precise soft tissue management and aid easier tension free primary closure at the time of implant placement. The extra time also allows for resolution of any pathology associated with the extracted tooth that may have been present. The amount of new bone formed in the socket will be limited and so difficulties in achieving primary stability is much like Type 1 placement. The bundle bone by now should have resorbed12 with an assumed decline in osteoclastic activity. This type of placement increases treatment time, particularly if simultaneous guided bone regeneration (sGBR) is carried out. Type 2 placement does, however, offer a much more predictable aesthetic outcome.
Type 3 (12–16 weeks post extraction): A substantial amount of new bone has formed within the extraction socket in the weeks between removing the tooth and implant placement.14 However, as discussed earlier, around 30% reduction of alveolar ridge width is to be expected. This facilitates implant placement by making the morphology of the site more homogeneous, allowing the implant to be placed more easily, although an ideal position may not be achievable. The soft tissue is generally mature and easier to manage during the surgical procedure. Like Type 2 placements, the treatment time is prolonged further and the additional waiting time will allow further reduction in hard and soft tissue volume. Type 3 placement, in the author's opinion, is best suited for replacement of premolars and molars.
Type 4 (>16 weeks post extraction): The extraction site has fully healed and there is plenty of time for soft tissue maturation, which is often well keratinized while hard tissues are dense and well corticated. This will also facilitate soft tissue management during the procedure while the problems of socket placement are avoided. Treatment time is extended substantially and there will likely be further reduction in the overall volume of bone with unfavourable external ridge contour that may require augmentation procedures. For this reason, Type 4 placement is generally avoided in most cases, except for the posterior teeth.
It should be remembered that other factors, apart from the timing of implant placement, should be considered in conjunction with the above (ie aesthetics, location, function).
Where
Implant placement is a surgical procedure used to solve a restorative problem and thus should always be restoratively driven. Regardless of the type of implant used or the timing of placement, the clinician should always aim for ideal 3-dimensional placement which will allow the creation of a harmonious restoration without compromising the longevity of the implant.
The 3-dimensions are:
Mesio-distal plane
Clearly, if a single tooth is to be replaced there is minimal scope for error but the surgeon should always avoid the temptation of placing an implant where good bone width is present to the exclusion of ideal placement. Implants placed too mesially or distally can result in unaesthetic restorations or even endanger the adjacent teeth and supporting structures either by direct damage or encroaching on supporting tissues, leading to unnecessary interdental bone loss and subsequent recession. A minimum of 1.5 mm distance to the adjacent tooth should be maintained in order to prevent resorption of the interposing bone, with consequential apical shift of the interdental papilla and resultant aesthetic complications.
Bucco-lingual/palatal plane
As above, if the surgeon opts for bone-driven implant placement there is a risk of creating poor aesthetics or compromising the final restoration. A buccally positioned implant will inevitably result in a longer clinical crown,15 whilst an implant placed too palatally will compromise ideal emergence and may interfere with the occlusion. We recommend a screw-retained restoration anteriorly, as a cingulum access to the screw head will ensure most optimal implant position. The majority of studies indicate the bucco-palatal dimension to have most significant impact on aesthetic outcome.
Apico-coronal plane
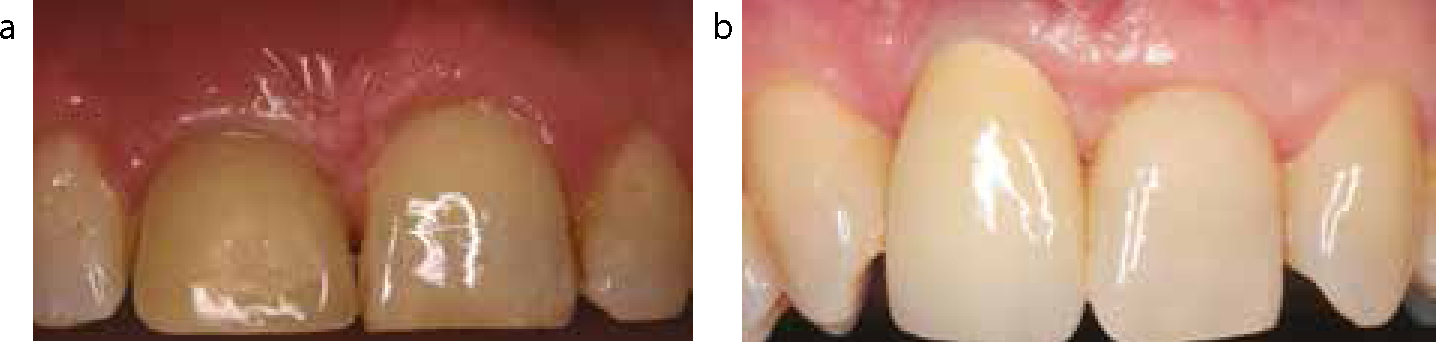
More subtle than the above parameters, if apico-coronal plane is ignored during the planning phase, it can create further issues (Figure 6). The restoration on an implant requires 3–3.5 mm of soft tissue attachment to emerge through. Similar to a tooth, this apico-coronal soft tissue dimension is termed the biologic width. If insufficient biologic width is present, bone resorption around the implant will occur to establish minimum dimensions.
Figure 6.
(a) Implant placed too shallow with resultant short clinical crown in UR1. (b) Implant placed too deep with eventual recession and poor aesthetics in UR1.
Thus an implant that is placed too shallow impedes the chances of creating an ideal emergence profile and also runs the risk of exposing the collar of the implant with resultant poor aesthetics.
On the other hand, an implant placed too deep will result in a longer clinical crown due to soft tissue recession. Further, the patient will not be able to remove continually accumulating plaque which will increase the likelihood of biologic complications.
Thorough pre-surgical restorative planning will allow for construction of a surgical template or stent which, when used, will facilitate ideal implant positioning. Various designs of surgical templates have been recommended. The authors favour a simple, cost-effective, but accurate vacuum-formed template (Figure 7).
Figure 7. Vacuum-formed surgical template.
Surgical correction of hard and soft tissue deficiencies
There is the possibility of correcting small hard and soft tissue anatomical deficiencies before, during or after implant placement.
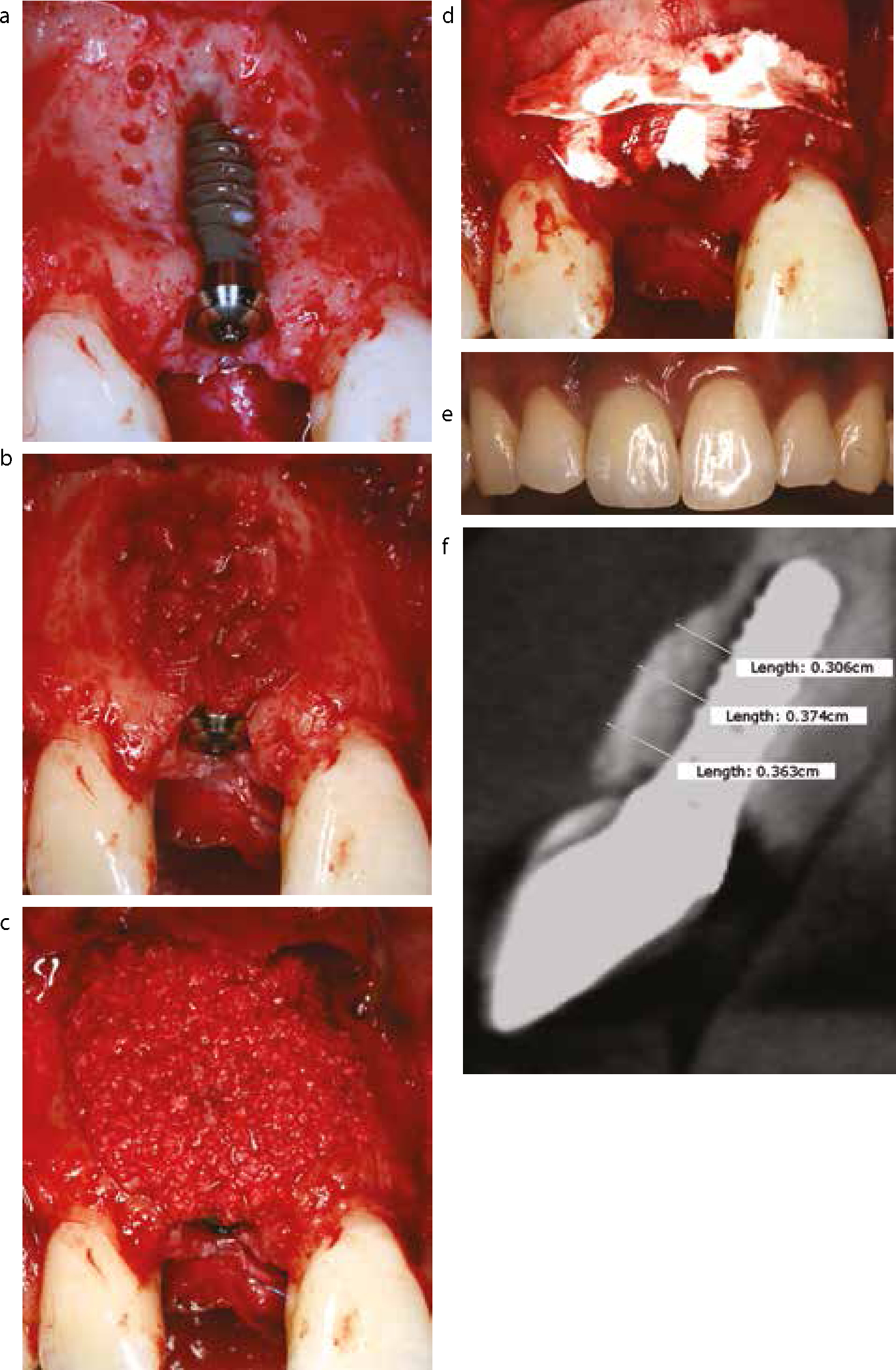
Given that the placement of dental implants is restoratively driven, if an optimal aesthetic outcome is desired, implants should be placed in an ideal 3-dimensional position. Such a protocol necessitates correction of underlying bone or soft tissue deficiencies. As mentioned previously, the alveolar ridge can be reconstructed either using a block bone graft or simultaneous guided bone regeneration (sGBR) in which particulate bone is covered by a membrane at the time of implant placement (Figure 8). In such circumstances, autogenous bone chips in combination with a particulate bone substitute are used to cover the entire surface of the implant, followed by placement of a barrier membrane.16
Figure 8.
(a) Labial bone dehiscence at implant site with corticotomies performed using a small diameter rose-head bur. (b) Implant covered with autogenous bone scrapings collected from adjacent site. (c) Subsequent coverage with xenograft material, which has been mixed in patient's blood collected locally from the surgical site. (d) Porcine collagen membrane placement using a bi-layer technique. (e) Post-op clinical outcome. (f) CBCT scan showing hard tissue regenerated and maintained.
There are biologic limitations with this technique and the previously existent bone envelope is considered a good determinant of this, which is why palatal rather than buccal position of the implant is favoured.
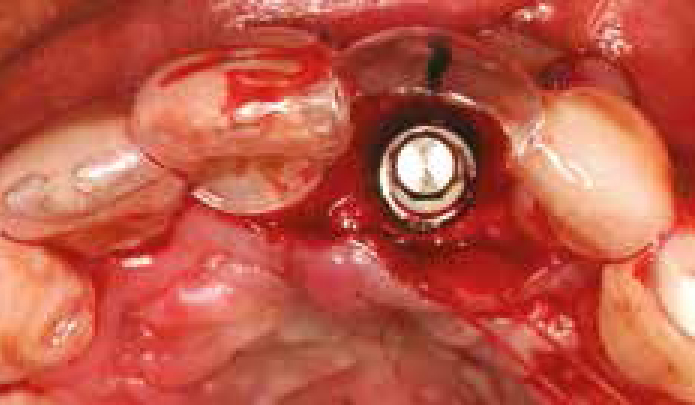
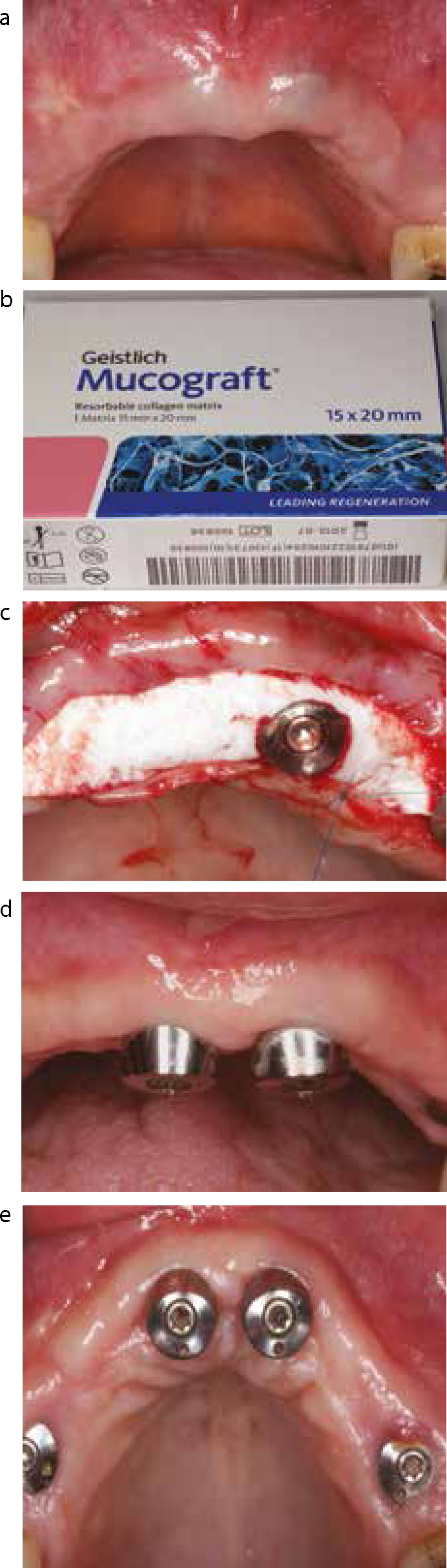
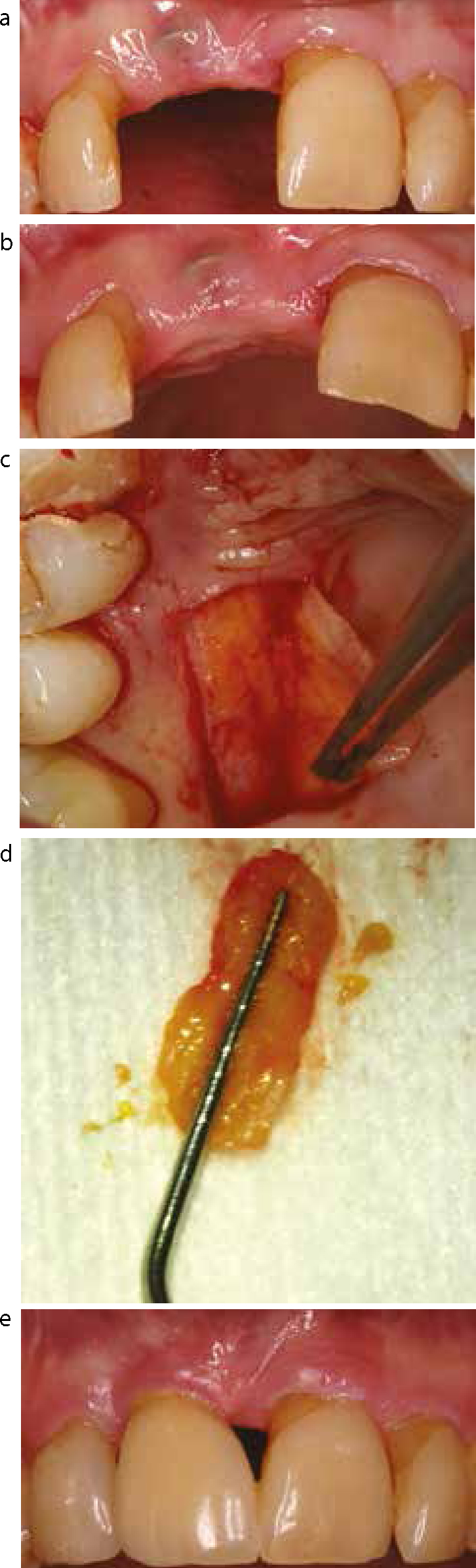
Further minor correction of anatomical deficiencies may be achieved with the use of soft tissue grafts or soft tissue graft substitutes such as Geistlich Mucograft®. These types of procedures can be used to bulk out local concavities or increase the band of attached gingiva present in an effort to achieve harmonious soft tissue framing (Figures 9 and 10).
Figure 9.
(a) Implants seen through alveolar mucosa. (b) Collagen matrix material. (c) Matrix placement. (d) Facial view of healed site. (e) Occlusal view of healed site with obvious increased band of keratinized tissue.Figure 10.
(a) Facial view of implant seen through non-keratinized alveolar mucosa. (b) Occlusal view. (c) Connective tissue graft harvesting. (d) Harvested graft, which was inserted using a pouch technique. (e) Final aesthetic result with keratinized tissue.
A common challenge to overcome with implant restorations is the loss of interproximal papillae. In teeth, when the distance from the contact point to the crest of interdental bone is 5 mm or less, the papilla almost fills the whole embrasure. If, however, the distance is greater than 5 mm, the likely occurrence of black triangles increases dramatically.6
Similar studies on papillae in single unit implant restorations showed comparable results,17 however, the height of the papilla between two adjacent implants is reduced (on average 4 mm). Therefore, the contact point between two adjacent implants needs to be shifted apically to prevent unaesthetic black triangles.18
The literature does mention techniques that could be employed in efforts to recreate lost papillae. These, however, have been found to be largely unpredictable and thus the above literature should be borne in mind.
Conclusions
Implants should not be seen as an automatic choice for the replacement of teeth after dento-alveolar trauma and other restorative options should always be considered. Only after careful analysis of the parameters mentioned above can a well structured definitive treatment plan be instituted.
Implant provision, particularly in the aesthetic zone, is not a straightforward procedure and much information needs to be gathered and considered before any final treatment decisions are made. Even if implants are to be the definitive treatment solution, patient factors may necessitate delay in their provision. If any of these facets are overlooked, reconstituting oral tissues will be less predictable and unaesthetic results may occur.