Littlewood S, Russell JS, Spencer RJ Why do orthodontic cases relapse?. Ortho Update. 2:38-44
British Standards Institute.London: BSI; 1983
McNally M, Mullin M, Dhopatkar A, Rock WP Orthodontic retention: why when and how?. Dent Update. 2003; 30:446-452
Melrose C, Millett DT Toward a perspective on orthodontic retention?. Am J Orthod Dentofacial Orthop. 1998; 113:507-514
Abudiak H, Shelton A, Spencer RJ, Burns L, Littlewood SJ A complication with orthodontic fixed retainers: a case report. Ortho Update. 2011; 4:112-117
Barlin S, Smith R, Reed R, Sandy J, Ireland AJ A retrospective randomized double blind comparison study of the effectiveness of Hawley versus vacuum-formed retainers. Angle Orthod. 2011; 81:404-409
Meade MJ, Millett D Retention protocols and use of vacuum-formed retainers among specialist orthodontists. J Orthod. 2013; 40:318-325
Bibona K, Shroff B, Best AM, Lindauer SJ Factors affecting orthodontists' management of the retention phase. Angle Orthod. 2014; 84:225-230
Atack N, Harradine N, Sandy JR, Ireland AJ Which way forward? Fixed or removable lower retainers. Angle Orthod. 2007; 77:954-959
Little R, Sinclair P Clinical implications of the University of Washington post-retention studies. J Clin Orthod. 2009; 23:645-650
Singh P, Grammati S, Kirschen R Orthodontic retention patterns in the United Kingdom. J Orthod. 2009; 36:115-121
Valiathan M, Hughes E Results of a survey-based study to identify common retention practices in the United States. Am J Orthod Dentofacial Orthop. 2010; 137:170-177
Angle EH, 7th edn. Philadelphia: SS White Dental Mfg; 1907
Hawley C A removable retainer. Int J Orthod. 1919; 2:291-298
Bearn DR Bonded orthodontic retainers: a review. Am J Orthod Dentofacial Orthop. 1995; 108:207-213
Sheridan JJ, LeDoux W, McMinn R Essix retainers: fabrication and supervision for permanent retention. J Clin Orthod. 1993; 27:37-45
Rowland H, Hichens L, Williams A The effectiveness of Hawley and vacuum-formed retainers: a single-center randomized controlled trial. Am J Orthod Dentofacial Orthop. 2007; 132:730-737
Hichens L, Rowland H, Williams A Cost-effectiveness and patient satisfaction: Hawley and vacuum-formed retainers. Eur J Orthod. 2007; 29:372-378
Tynelius GE, Bondemark L, Lilja-Karlander E A randomised controlled trial of three orthodontic retention methods in Class I four premolar extraction cases – stability after 2 years in retention. Orthod Craniofac Res. 2013; 16:105-115
Tynelius GE, Lilja-Karlander E, Petrén S A cost-minimization analysis of an RCT of three retention methods. Eur J Orthod. 2014; 36:436-441
Taiyub AR, Littlewood SJ, Munyombwe T, Bubb NL Wear resistance of four types of vacuum-formed retainer materials: a laboratory study. Angle Orthod. 2014; 84:656-664
Bjering R, Birkeland K, Vandevska-Radunovic V Anterior tooth alignment: a comparison of orthodontic retention regimens 5 years posttreatment. Angle Orthod. 2014;
Tibbetts JR The effectiveness of three orthodontic retention systems: a short-term clinical study. Am J Orthod Dentofacial Orthop. 1994; 106
Rinchuse DJ, Rinchuse DJ Active tooth movement with Essix-based appliances. J Clin Orthod. 1997; 31:109-112
Lindauer S, Shoff R Comparison of Essix and Hawley retainers. J Clin Orthod. 1998; 32:95-97
Rinchuse DJ, Miles PG, Sheridan JJ Orthodontic retention and stability: a clinical perspective. J Clin Orthod. 2007; 41:125-132
Gill DS, Naini FB, Jones A, Tredwin CJ Part-time versus full-time retainer wear following fixed appliance therapy: a randomized prospective controlled trial. World J Orthod. 2007; 8:300-306
Kumar A, Bansal A Effectiveness and acceptability of Essix and Begg retainers: a prospective study. Aust Orthod J. 2011; 27:52-56
Meade MJ, Millett DT, Cronin M Social perceptions of orthodontic retainer wear. Eur J Orthod. 2014; 36:649-656
Demir A, Babacan H, Nalcaci R, Topcuoglo T Comparison of retention characteristics of Essix and Hawley retainers. Korean J Orthod. 2012; 42:255-262
Hoybjerg AJ, Currier GF, Kadioglu O Evaluation of 3 retention protocols using the American Board of Orthodontics cast and radiograph evaluation. Am J Orthod Dentofacial Orthop. 2013; 84:56-61
Jäderberg S, Feldmann I, Engström C Removable thermoplastic appliances as orthodontic retainers – a prospective study of different wear regimens. Eur J Orthod. 2012; 34:475-479
Thickett E, Power S A randomized clinical trial of thermoplastic retainer wear. Eur J Orthod. 2010; 32:1-5
Sauget E, Covell DA, Boero RP, Lieber WS Comparison of occlusal contacts with use of Hawley and clear overlay retainers. Angle Orthod. 1997; 67:223-230
Sun J, Yu Y, Liu M, Chen L, Li H, Zhang L Survival time comparison between Hawley and clear overlay retainers: a randomized trial. J Dent Res. 2011; 90:1197-1201
Agha RAQ, Ghaib NH Relapse during retention with Hawley and clear overlay retainers in Iraqi Adults. Iraqi Orthod J. 2005; 1:10-12
Ponitz RJ Invisible retainers. Am J Orthod. 1971; 59:266-272
Wong PM, Freer TJ A comprehensive survey of retention procedures in Australia and New Zealand. Aust Orthod J. 2004; 20:99-106
Gottlieb EL, Nelson AH, Vogels D 2008 JCO study of orthodontic diagnosis and treatment procedures. Part 1. Results and trends. J Clin Orthod. 2008; 42:625-640
Wang F A new thermoplastic retainer. J Clin Orthod. 1997; 31:754-757
Pithon MM A modified thermoplastic retainer. Prog Orthod. 2012; 13:195-199
Birdsall J, Robinson S A case of severe caries and demineralisation in a patient wearing an essix-type retainer. Primary Dent Care. 2008; 15:59-61
Xu XC, Li RM, Tang GH Clinical evaluation of lingual fixed retainer combined with Hawley retainer and vacuum-formed retainer. Shanghai Kou Qiang Yi Xue. 2011; 20:623-626
Mai W, He J, Meng H Comparison of vacuum-formed and Hawley retainers: a systematic review. Am J Orthod Dentofacial Orthop. 2014; 145:720-727
Little RM The Irregularity Index: a quantitative score of mandibular anterior alignment. Am J Orthod. 1975; 68:554-563
Richmond S, Shaw WC, O'Brien KD The development of the PAR Index (Peer Assessment Rating): reliability and validity. Eur J Orthod. 1992; 14:125-139
Casko J, Vaden J, Kokich V Objective grading system for dental casts and panoramic radiographs. Am J Orthod Dentofacial Orthop. 1998; 114:589-599
Littlewood SJ, Millett DT, Doubleday B, Bearn DR, Worthington HV Retention procedures for stabilising tooth position after treatment with orthodontic braces. Cochrane Database Systematic Review. 2006;
Ge ZL, Jiao X, Tian JH, Yang KH Clinical effectiveness of vacuum-formed versus Hawley retainers: a systematic review. Chin J Evid Based Med. 2012; 12:596-601
Professor of Orthodontics/Consultant, Orthodontic Unit, Cork University Dental School and Hospital, University College Cork, Wilton, Cork, Republic of Ireland
The need for long-term retention following orthodontic treatment is now considered essential to prevent post-orthodontic treatment relapse. The vacuum-formed retainer (VFR) has gained popularity in recent times. This paper describes briefly the characteristics of VFRs and summarizes the evidence in relation to their effectiveness.
Clinical Relevance: VFRs are now widely used after orthodontic treatment and it is important that clinicians adopt an evidenced-based approach to their use.
Article
Retention is the phase of orthodontic treatment that attempts to maintain teeth in their corrected positions after active tooth movement.1 It aims, therefore, to prevent relapse which is defined as the return, following correction, of the features of the original malocclusion.2 Although, rather erroneously, patients may consider relapse to include age changes unrelated to orthodontic treatment,1,3 this is not what is regarded here for the purposes of retention.
The rationale for maintaining the teeth in their treated position is to:
Allow for reorganization of the gingival and periodontal tissues;
Minimize changes due to growth;
Permit neuromuscular adaptation to the corrected tooth position; and
Maintain teeth in unstable positions (sometimes necessary owing to compromise in treatment objectives or for aesthetic reasons).1,3,4
The principal method of retention involves the use of an orthodontic retainer. The choice of retainer depends on many factors, such as:
Research has shown that relapse occurs in patients with and without orthodontic retainers.9,10 There appears to be agreement that lifetime retention is necessary if relapse is to be minimal.7,11 Wide variation exists, however, in the retention regimes prescribed by orthodontists.7,11,12
Angle described the first retainer type, based on banded fixed appliances.13 Removable retainers, such as the Hawley retainer14 constructed from acrylic and stainless steel wire, were subsequently developed.3 With the advent of the acid-etch technique in dentistry, bonded fixed retainers (BRs) became another method used to minimize relapse.15 Most recently, the vacuum-formed retainer (VFR) has been introduced16 (Figures 1–3).
Present a brief overview of the scientific evidence available in relation to the effectiveness of VFRs.
Characteristics of VFRs
Development
In the literature, the terms ‘drawn down retainer’,3 ‘vacuum retainer’,11 ‘vacuum-formed retainer,6,17,18,19,20,21,22,23,24,25 ‘Essix retainer’,16,26,27,28,29,30,31,32,33,34 ‘thermoplastic retainer’,12,35,36 ‘(clear) overlay retainer’,37,38,39 ‘invisible retainer’40,41 and ‘(clear) slipover’42 appear to be interchangeable. For the purposes of this article, the term ‘VFR’ will be used.
The VFR is a removable thermoplastic retainer and was introduced by Ponitz40 in 1971 and further developed by Sheridan.16 Although minor tooth movement can be achieved by modifying VFR design,27 this article will focus on its use as a retainer. The VFR has increased in popularity and is the most commonly chosen retainer by orthodontists in the Republic of Ireland,7 Australia41 and in the National Health Service (NHS) and hospital practices in the United Kingdom.11
Manufacture
A VFR may be manufactured on two types of plastic thermoforming machine:
Pressure machines – ‘which are superior’16 and force the heat-softened ‘plastic’ over the end of treatment plaster mould with positive pressure (eg Biostar™) (Figure 4).
Vacuum machines – which adapt the heat-softened plastic to the mould by negative pressure (Figure 5).
Examples of material types used in its manufacture include:
*Essix type ’A’ co-polyester (which is reportedly more aesthetic, but tends to crack and fracture more easily); and
*Essix type ‘C+‘ polypropylene or ethylene co-polymer (supposedly more resilient, but less retentive).24,29 (*RaintreeEssix, Sarasota, FL, USA).
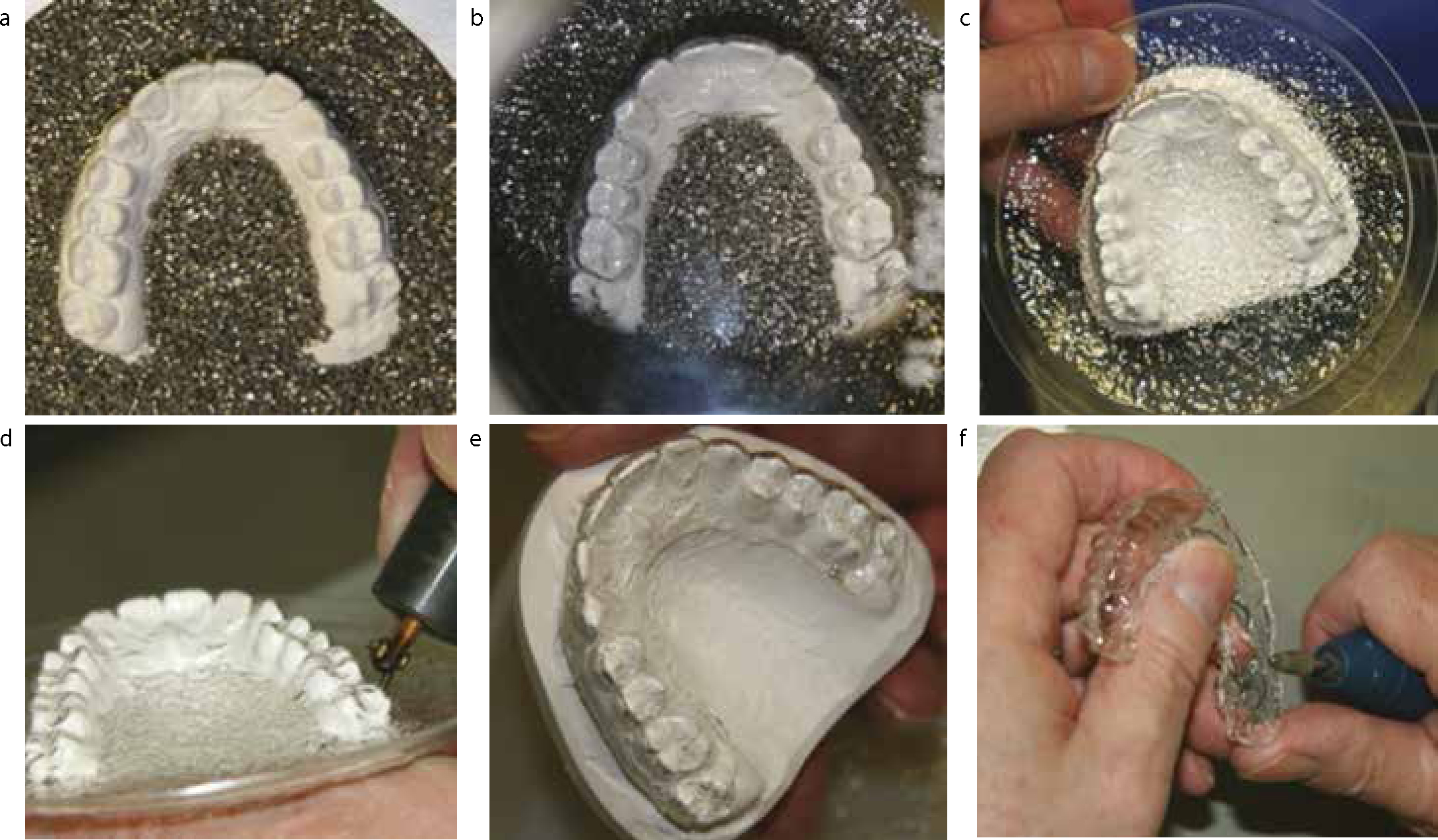
Rectangular and round blanks are available (Figure 6). ‘Blank thicknesses’ ranging from 0.63 to 2.0 mm have been described.17,21,22,37,38 Processing of the blanks reportedly reduces the thickness by half,16 although a recent study suggested that thickness reduction may not be uniform.35Figure 7 outlines the main stages in manufacture of a VFR in the Biostar™ machine.
Figure 6. A rectangular and round blank prior to retainer fabrication.Figure 7.
(a–f) The main stages in the manufacture of a VFR: (a) plaster cast positioned in Biostar™ machine; (b) after the heat-softened ‘blank’ has been ‘forced’ over the plaster cast with positive pressure; (c) removal of plaster cast with ‘adapted blank’ from Biostar™ machine; (d) gross trimming of VFR; (e) after gross trimming of VFR; (f) fine trimming with acrylic bur.
Design
Two main retainer designs have been described. The original ‘Essix’ retainer was canine-to-canine coverage only16,22,28,35 and is still popular in the United States, whereas the VFR tends to describe full occlusal coverage6,17,21,30 or coverage extending to halfway across the most terminal molar37,43 (Figures 8–10). The marginal extension in each design is commonly 1–2 mm buccal and 3–4 mm lingual to the gingival margins.16 Additional designs have been described.38,43,44
Figure 8.
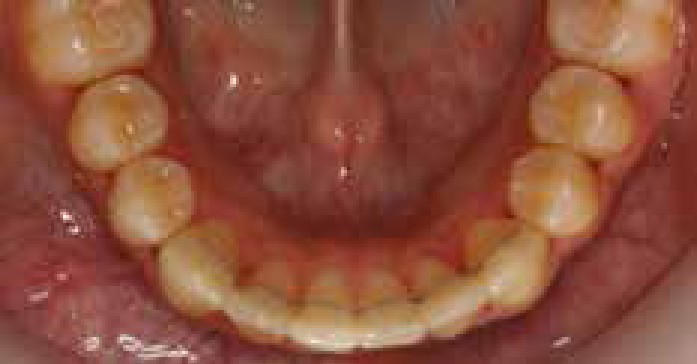
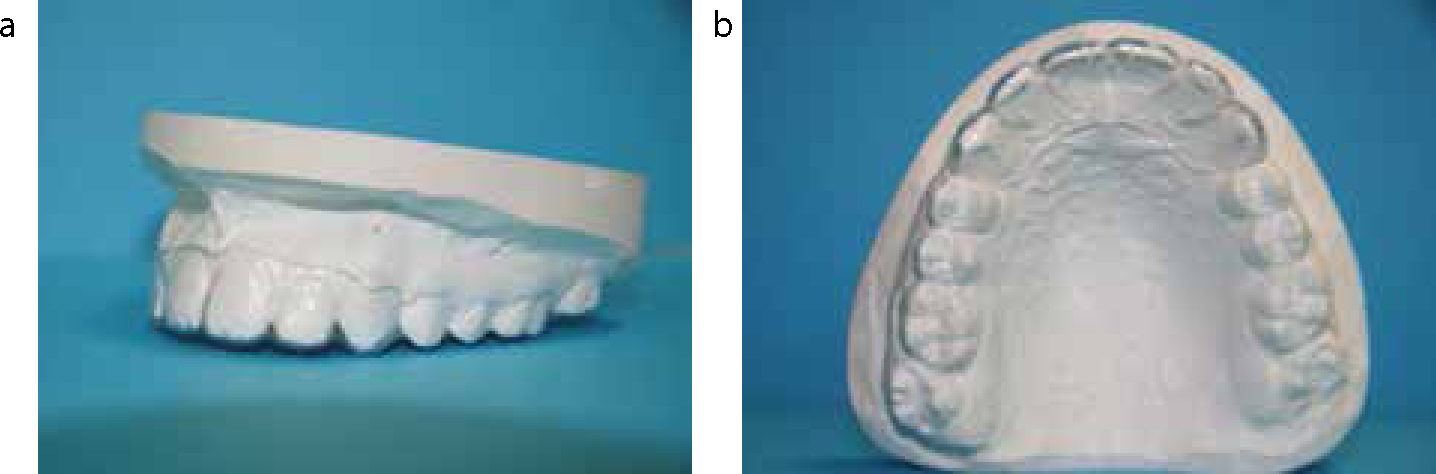
(a, b) Upper canine-to-canine VFR. Note notched margin at canines – this facilitates removal of the VFR with the fingernail.Figure 9. Upper full occlusal coverage VFR.Figure 10. Lower VFR with occlusal coverage extending to halfway across the most terminal molar.
VFR fit and maintenance
A VFR must be a precision fit. It clicks into place and is not easily removed.16 The appliance is retained in the mouth by engagement in the undercuts gingival to the contact points of the teeth. The fit may be adjusted at chairside by increasing or reducing the depth of the undercuts in the plastic. Blanching will be evident if the retainer is engaging too tightly on the gingiva. Adjustment with scissors and/or a greenstone in a slow speed handpiece may be required.
Patients are advised to refrain from using toothpaste to clean a VFR as this will ‘dull’ the appearance. Regular cleaning with a soapy cotton-tip swab and/or a proprietary cleaning agent (eg Retainer BriteTM*) has been recommended.16
Advantages
Proposed advantages of the VFR include:
Aesthetic appearance;
Patient comfort and acceptability;
Speed, ease and low cost of fabrication.3,12,16,32,41
Disadvantages
Proposed disadvantages include:
Compromised appliance retention where there is hyperplastic gingivae, poor oral hygiene or a spaced dentition;
Loss, breakage (Figure 11) and poor wear resistance (particularly along the occlusal and incisal surfaces – this may be a concern with bruxism);
A possible inability to maintain expanded arches (Figure 12 shows a modified VFR that attempts to overcome this45) and to maintain alignment of previously severely rotated and/or displaced teeth due to its lack of rigidity;
Inhibition of any desired vertical ‘settling-in’ of the occlusion subsequent to active orthodontic treatment;
The potential for demineralization, caries and poor gingival health if a careless dietary lifestyle with frequent ‘fizzy’ drink intake is adopted while the VFR is being worn;
Reliance on patient compliance with instructed wear in view of the retainer being removable.3,5,6,28,29,37,46
Figure 11. VFR after patient ‘stepped on it’.Figure 12. Modified upper VFR incorporating 0.8 mm stainless steel wire to maintain expanded arch.
Evidence in relation to VFR effectiveness
Several studies have compared the effectiveness of VFRs with other retainer types.6,17,18,19,20,21,22,23,25,26,28,31,33,34,37,38,39,47 Prospective randomized controlled trials (RCTs) are considered the gold standard for study design18,48 and will provide the focus in this article's assessment of the evidence available in relation to the effectiveness of this retainer type.
Effectiveness of VFRs compared with other retainers in maintaining stability after orthodontic treatment
When assessing stability after orthodontic treatment, most retention studies have focused on changes in lower incisor alignment, as this is a highly noticeable site of relapse and often complained of by patients.18 Little's Irregularity Index (LII)49 is most commonly used to assess incisor irregularity; it is usually measured directly from plaster models but may also be applied to digital models (Figure 13). Additional measurements assessed in retention studies include intercanine width, intermolar width, overjet, overbite, arch length, the PAR Index50 score and the American Board of Orthodontics discrepancy index and cast and radiograph evaluation.51 Measurements at the time of fixed appliance removal are compared with those taken after a period of retainer wear. Patients who require orthognathic surgery and/or have craniofacial anomalies, intellectual impairment, hypodontia, single arch treatment or require a specific retainer type because of periodontal consideration or arch expansion, tend to be among the exclusion criteria in retention studies.6,17,22,30,35,36
Figure 13. Little's Irregularity Index (LII)49 – measurement of the summed contact point displacements.
Table 1 shows the mean changes in LII recorded in recent RCTs comparing the effectiveness of VFRs with other retainer types. In one study,31 all patients were also fitted with BRs. Outcomes were measured between 6 and 24 months after active orthodontic treatment.
Canine-to-canine coverage 2.0 mm thickness F/T followed by P/T
VFR
pre-fabricated positioner
Maxilla
0.5–0.8
1.1
KEY:
: statistically significant;
BR: bonded retainer; F/T: full-time; N: number of subjects; P/T: part-time; VFR: vacuum-formed retainer; vs: versus.
All subjects had completed a course of upper and lower fixed appliance treatment with one study17 including patients who had received upper removable appliance and/or functional appliance treatment prior to fixed appliances, with or without extractions. Two studies detailed the ‘pre-orthodontic treatment’ clinical characteristics of their subjects. One22 included patients who had ‘normal skeletal and dento-alveolar sagittal, vertical and transverse relationships’ and required extraction of four premolar teeth as part of their orthodontic treatment. Another17 included patients from all incisor2 and skeletal classifications, with or without missing incisor or premolar teeth.
The prescribed VFR wear protocol differed in all studies. Two adopted a full-time wear protocol; one21 required removal for eating while the other31 did not. Another study17 required full-time wear (except eating and toothbrushing) for the first week after provision of the retainer and 12-hour daily wear thereafter. Patients in a Swedish study22 were instructed to wear their VFRs 22–24 hours per day for 2 days and nights, followed by ‘during the night’ for 12 months, and then alternate nights for the next 12 months.
Significant differences were noted between the retainers in LII, but not in any of the additional measurements assessed. Some relapse occurred in all measurements. The evidence suggests that VFRs were slightly more effective than Hawley retainers in maintaining incisor alignment in the mandible but less effective than BRs. No significant differences appear to exist between the VFR, Hawley retainer and pre-fabricated positioner in maintaining incisor alignment in the maxilla.
Part-time vs full-time wear of VFRs
Three recent studies have investigated whether the effectiveness of VFRs differs with regard to the amount of daily wear of the retainer.30,35,36Table 2 outlines the median or mean changes in LII recorded at 6–12 months into the retention phase in patients adopting full-time or part-time wear of VFRs. All subjects had completed a course of upper and lower fixed appliance treatment, with a Swedish study35 also including patients who had single arch fixed appliance treatment. All subjects were treated with extraction of four premolars in another study.36 Gill et al30 included subjects who were treated with or without extractions. That study also provided a breakdown of subjects by ‘molar classification’. ‘Pre-orthodontic treatment’ clinical characteristics or the number of subjects who were treated with extractions were not specified in the Swedish study.35
Reducing from 10 hours daily in the first six months to one or two nights weekly.36
There were no clinically significant differences between the changes in LII or in the additional parameters measured. Part-time wear of a VFR appears to be sufficient in maintaining post-orthodontic treatment stability. Greater pre-treatment crowding than that recorded in these studies, however, may warrant a different VFR protocol.30,36
Adverse effects on dental and periodontal health
It is essential that any prescribed retainer is not responsible for adverse health effects.52 Data from one study20 indicated that a VFR may be less harmful to dental and periodontal tissues than a BR. After 12 months in retention, no caries or periodontal pocketing was found related to the lower six anterior teeth in patients wearing either retainer. There was, however, significantly more gingival bleeding in those wearing a BR.
Quality of life assessment
There has been an increasing emphasis on assessment of patient satisfaction in healthcare provision; this is usually conducted via self-reported questionnaires.18 In a study comparing full- and part-time VFR wear, patients reported difficulty with speech (22%), soreness (13%), bad taste (10%) and difficulty with cleaning (10%). Most (97%), however, found their VFRs ‘easy to get used to’.35
Patients also found BRs significantly more ‘acceptable to wear’ than VFRs,19 but VFRs were significantly better than Hawley retainers in terms of speech and appearance (92.8% vs 82.6%).18 In addition, VFRs were significantly more comfortable and aesthetic than Begg retainers but eating/chewing was easier with Begg retainers.31 Retainer wear during eating was instructed for both types of removable retainer in that study which is contrary to the wear protocol for VFRs that is currently recommended.16,17,21
Survival of retainers
The survival rate of retainers is an important consideration as it may have an impact on cost, patient satisfaction and effectiveness. In the six months following orthodontic treatment, significantly fewer breakages were reported with VFRs (6.6%) compared to Hawley retainers (19.4%), although loss rates were similar.18 At 12 months, however, Sun et al found no significant difference in survival times between VFRs and Hawley retainers.38 In that study, patients were advised to wear their retainers ‘day and night’. VFR thickness was 0.75 mm and fracture (17%) followed by loss (15%) were the most common reasons for VFR ‘breakage’. Mandibular VFR fracture was most common in the midline.38
In the first 12 months post-orthodontic treatment, more problems have been reported with VFRs compared with BRs. Fractures (28%), wear (28%) and loss (14%) were the most common problems with VFRs and composite loss (5%) and de-bond (12%) were most commonly reported with BRs.19
Cost-effectiveness
As a trend for advising life-time wear of retainers now exists,7,11,12 the cost implications of prescribing a particular retainer is an important factor in retainer choice. In the UK, VFRs were found to be more cost-effective than Hawley retainers in the six months after orthodontic treatment.18 This was not only from the perspective of the patient (mean difference in cost per patient: €4.71) but particularly the NHS (mean difference in cost per patient to the NHS: €31.34) and the orthodontic practice (mean difference in cost per patient to the practice: €32.60).
A Swedish study,23 however, showed that a pre-fabricated positioner was more cost-effective than either an upper VFR and lower BR combined or upper VFR and lower stripping of the incisors and cuspids combined in the two years after orthodontic treatment. The ‘societal costs’ per patient for scheduled appointments/unscheduled appointments were €420/€0 for a pre-fabricated positioner, €497/€807 for an upper VFR and lower BR combined, and €451/€303 for an upper VFR and lower stripping of the incisors and cuspids combined.
Clinician perceptions
Not surprisingly, clinicians have found VFRs significantly easier to fit than BRs. One study19 found that 97% of VFRs took less than 10 minutes to fit compared with ‘up to 20 minutes’ for 96% of BRs.
Compliance
A limitation with removable appliances is patient compliance.35 If the retainer is not worn as instructed, relapse is inevitable. Patient-reported compliance with instructed VFR wear was found in 35–95% of patients at 6–12 months after orthodontic treatment;18,21,35 one study21 reported that stability of mandibular incisor alignment was proportional to patient reported wear.
Discussion
In this article, we have described the characteristics of VFRs. In addition, we have provided a summary of the evidence in relation to the effectiveness of VFRs. Although only clinical trials with the best quality research design (RCTs) were considered, these included a variety of VFR designs and retention protocols. The studies also differed in clinical setting, the number, age, ‘pre-orthodontic treatment’ clinical characteristics (such as presenting malocclusion) of subjects, orthodontic treatment carried out and time-points of outcome measurements. In addition, the value at which changes of LII was considered to be statistically significant varied from 0.2 to 2.0 mm. This lack of standardization should be taken into account when interpreting the outcomes assessed in this overview. Also, not all studies provided data on the age of subjects but most appear to have concentrated on adolescents. Conclusions from these studies, therefore, may not be relevant to older patients.
There are, however, some suggestions from these trials that can offer evidence-based guidance to the clinician with regard to retainer choice and wear protocol:
A VFR is at least as effective as a Hawley retainer at maintaining post-treatment stability but less effective than a BR at maintaining mandibular incisor alignment;
Part-time wear of a VFR is as effective as full-time wear in maintaining the end of orthodontic treatment result, although patient factors such as severe crowding may warrant an alternative wear protocol;
More retainer-related problems are reported by those wearing a VFR compared to a BR but less than those wearing a Hawley retainer;
A VFR does not have adverse effects on dental and periodontal health and is more cost-effective than Hawley retainers.
Retainer design, however, must be tailored for the individual patient. The patient's pre-treatment situation and end of orthodontic treatment result should be important factors in retainer choice. Further investigation and evaluation of VFRs is required in those malocclusions which require special consideration. Patients presenting with periodontally compromised or severely rotated and/or displaced teeth prior to orthodontic treatment may not be suitable for a VFR. Without modification, a VFR may not be sufficiently rigid to maintain an expanded maxillary arch.45 In addition, the relatively high fracture and wear rates reported in the trials may suggest that further investigation is required to develop a more robust VFR material. The concern, however, that a VFR may be associated with an anterior open bite does not appear to be borne out in the studies reviewed here.17,30,35,36
As there appears to be agreement among orthodontists that life-time wear of a retainer is necessary to minimize relapse,7,11,12,41 and all RCTs in this review evaluated retainer effectiveness 6–24 months into retention, future research is also required to assess the following over the long-term:
The effectiveness of a VFR in maintaining end of orthodontic treatment stability compared with other retainers in adolescents and adult patients;
Optimal VFR design and wear protocol;
Effects of wear of a VFR on quality of life;
Cost-effectiveness of a VFR;
Dental and periodontal health effects of VFR wear.48,52,53
Conclusion
Based on the available evidence, the VFR appears to be a popular orthodontic retainer because of its clinical and cost-effectiveness and patient and clinician acceptability. VFR design characteristics, dependence on patient compliance and other patient-related factors, such as presentation of severely rotated and/or displaced teeth prior to orthodontic treatment, however, may limit the VFR as the optimal retainer choice for all orthodontic patients. Further research is necessary to determine whether the advantages of VFRs are maintained over the long-term.