Wheeler RC., 7th edn. Philadelphia: W B Saunders Company; 1993
Hua F, He H, Ngan P, Bouzid W. Prevalence of peg-shaped permanent lateral incisors: a meta-analysis. Am J Orthod Dentofacial Ortho. 2013; 144:97-109
Thesleff I. Genetic basis of tooth development and dental defects. Acta Odontol Scand. 2000; 58:191-194
Fleischmannova J, Matalova E, Tucker AS, Sharpe PT. Mouse models of tooth abnormalities. Eur J Oral Sci. 2008; 116:1-10
Hobkirk JA, Goodman JR, Jones SP. Presenting complaints and findings in a group of patients attending a hypodontia clinic. Br Dent J. 1994; 177:(9)337-339
Brook AH. A unifying aetiological explanation for anomalies of human tooth number and size. Arch Oral Biol. 1984; 29:(5)373-378
Brook AH. Variables and criteria in prevalence studies of dental anomalies of number, form and size. Community Dent Oral Epidemiol. 1975; 3:(6)288-293
Brin I, Becker A, Shalhav M. Position of the maxillary permanent canine in relation to the anomalous or missing lateral incisors: a population study. Eur J Ortho. 1986; 8:(1)12-16
Becker A, Smith P, Behar R. The incidence of anomalous maxillary lateral incisors in relation to palatally displaced cuspids. Angle Orthod. 1981; 51:24-29
Nixon PJ, Robinson S, Gahan M, Chan MF. Conservative aesthetic techniques for discoloured teeth: 2. Microabrasion and composite. Dent Update. 2007; 34:(3)160-166
Carter NE, Gillgrass TJ, Hobson RS, Jepson N, Meechan JG, Nohl FS, Nunn JH. The interdisciplinary management of hypodontia: orthodontics. Br Dent J. 2003; 194:361-366
Maxillary microdont lateral incisors can have significant implications on the development of the permanent dentition in terms of the eruption of maxillary permanent canines, as well as on the aesthetics of the upper labial segment and the overall occlusion, depending on the extent of microdontia. This paper describes the aetiology, clinical implications and management of the maxillary microdont lateral incisor.
Clinical Relevance: The definitive management of the maxillary microdont lateral incisor may involve either a restorative or orthodontic approach or, in some cases, a combined orthodontic-restorative approach.
Article
The term ‘microdont teeth’ or microdontia refers to teeth that are developmentally small, often in three dimensions. The normal crown height of the maxillary lateral incisor is 9 mm, the length of the root is about 13 mm, the mesiodistal crown diameter is about 6.5 mm and the labiolingual crown dimension is about 6 mm.1 The term ‘microdont’ or peg-shaped lateral incisors refers to lateral incisor teeth that have either a reduced mesiodistal width and/or a reduction in the vertical height. These teeth are more often maxillary lateral incisors as opposed to mandibular and may be unilaterally or bilaterally microdont. The overall prevalence of peg-shaped maxillary permanent lateral incisors is 1.8%.2 The occurrence rates are higher in Down's syndrome (3.1%) than in Afro-Caribbean (1.5%) and Caucasian (1.3%) patients, and in orthodontic patients (2.7%) than in the general population (1.6%) and dental patients (1.9%). Women are 1.35 times more likely than men to have peg-shaped maxillary permanent lateral incisors. The prevalence rates of unilateral (0.8%) and bilateral peg-shaped maxillary permanent lateral incisors are approximately the same.
Aetiology
Tooth development is a complex process which occurs as a result of interactions between the oral epithelium and ectomesenchyme derived from the neural crest. This process involves growth factors, transcription factors, signalling pathways and other morphogens.3 As a result of such complex interactions, disturbances can occur in the process which can lead to disorders of tooth morphology, such as microdontia, which can affect the maxillary lateral incisors and any other teeth. In addition, defects in these pathways can result in disorders of tooth number (hypodontia or supernumerary teeth) and tooth mineralization (amelogenesis imperfecta or dentinogenesis imperfecta).4 Microdont lateral incisors, in the majority of cases, have a genetic basis and may be identified by a familial trait, although the genetic mechanisms are not well understood. Diminutive or microdont teeth can also present as an isolated diagnosis which suggests that it may occur spontaneously. Microdontia is often an accompanying feature of hypodontia5,6,7 and often a diminutive lateral maxillary incisor may present alongside the developmental absence of the contralateral lateral incisor. This association of hypodontia with microdontia is further evidence to support a genetic basis for microdontia affecting tooth morphology.
Dental development
The maxillary lateral incisor is the second tooth of the incisor series and commences its calcification at about 12 months of age. These teeth then generally erupt into the mouth at about 8 years of age, with a 6 month window either side. They tend to erupt in a more palatal position to the central incisor because they erupt after the central incisors and before the loss of the deciduous canines. Following eruption, root completion of the lateral incisors occurs 2–3 years later.
Classification
The authors have classified microdont lateral incisors as:
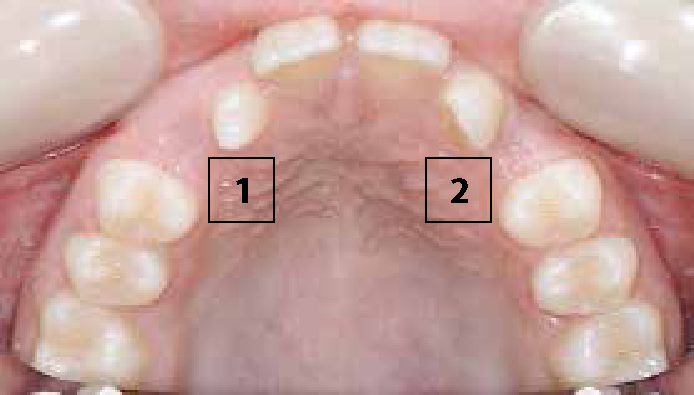
Mildly microdont upper lateral incisors where the mesiodistal width of the crown is about 2/3 the average width of an upper lateral incisor (Figure 1 – 2).
Significantly microdont or ‘peg laterals’ where the mesiodistal width of the crown is < 2/3 the average width of an upper lateral incisor (Figure 1 – 1).
Figure 1. An upper occlusal view showing a significantly microdont lateral incisor (1) and a mildly microdont lateral incisor (2).Figure 2. A spaced upper arch with diminutive upper lateral incisors.
Clinical presentation
Diminutive lateral incisors may have a number of effects on the overall malocclusion. They may cause:
Figure 3. A reduced overjet as a result of diminutive upper laterals.
Association with impacted maxillary canines
Microdont or developmentally absent lateral incisors may also be associated with impacted upper canines.8 The guidance theory of canine eruption suggests that the maxillary canine is guided in its path of eruption by the root of the maxillary incisor. In situations where the lateral incisor is diminutive or microdont, this guidance may be disrupted and the canine may be more likely to erupt into an ectopic position.9
An example of this association between diminutive lateral incisors and ectopic maxillary canines is shown in Figure 4, in which a patient with bilaterally diminutive upper lateral incisors has presented with bilaterally ectopic upper canines.
Figure 4. OPG radiograph of patient with diminutive upper lateral incisors with ectopic canines.
Association with hypodontia
As mentioned above, diminutive maxillary lateral incisor teeth may be associated with a developmental absence of teeth (Figure 5).
Figure 5. Developmental absence of UR2 associated with a diminutive UL2.
Management
The options for management can be divided according to the degree of microdontia and patient expectations from treatment and can be summarized as follows:
Mildly microdont
– No treatment;
– Orthodontics alone.
Significantly microdont
– No treatment;
– Orthodontics + restorative build-ups with:
– Resin-composite;
– Veneers;
– Crowns.
– Extraction and orthodontic space closure (in patients in whom there is a space requirement and where canines can be accepted as lateral incisors);
– Extraction and prosthetic replacement where none of the above is possible.
The degree of microdontia
Mildly microdont upper lateral incisor (2/3 the normal width of an upper lateral incisor)
If the upper lateral incisors are only slightly diminutive then a satisfactory clinical and aesthetic outcome may be achieved by accepting the lateral incisors in their presenting microdont state. Orthodontic treatment carried out to close residual space resulting from the microdont lateral incisors will, however, result in a tendency to a Class II buccal segment relationship as the maxillary posterior teeth move mesially to take up the space resulting from the diminutive lateral incisor. Alternatively, orthodontic treatment to close all the space in the upper arch in cases of bilaterally diminutive lateral incisors may cause a reduction in the overjet (Figure 3). This will occur if there is a genuine tooth size discrepancy.
A Kesling set-up can be done prior to starting any orthodontic treatment to determine the effects of closing the upper arch space on the overall malocclusion. One of the other methods of taking up the extra spacing resulting from the diminutive upper lateral incisor teeth is to increase the torque in the upper labial segment either by using super torque brackets or by adding additional palatal root torque in the finishing stages of treatment.
Significantly microdont or ‘peg shaped’ (< 2/3 the average width of an upper lateral)
In such situations the treatment options include the following.
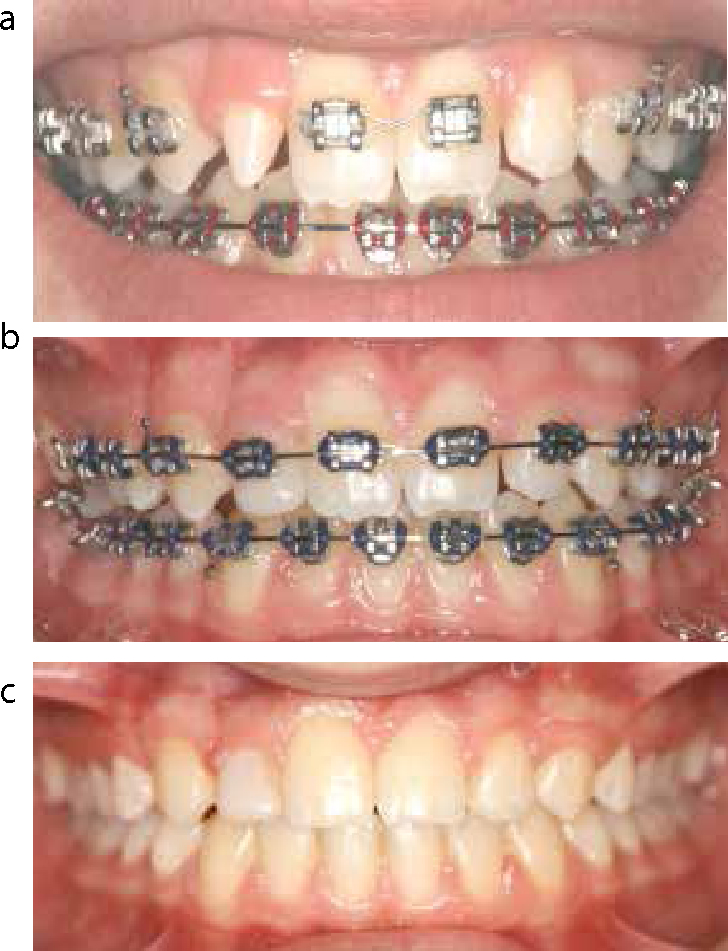
Composite build-up of the diminutive upper lateral incisor can be carried out to increase its mesiodistal width to allow it to be the equivalent width of an average lateral incisor. This can be done by adding composite to the mesial and distal aspects of the microdont tooth. This will provide an improved aesthetic appearance and may also allow for correction of the buccal segment relationship to Class I (Figure 6 a–c).
The microdont tooth could be orthodontically moved into the middle of the space (Figure 7) with an equal amount of space mesial and distal to the lateral incisor if the mesial and distal axial walls are parallel.
Should one axial wall flare out, then it is often preferable to abut this wall to the adjacent tooth and then build-up the other axial wall. The limit to the increase in mesiodistal width that can be achieved is usually the emergence profile of the composite build-up at the cervical margin of the microdont lateral incisor tooth. Care needs to be taken to ensure that a plaque trap is not created at this point by an over-ambitious build-up, leading to an over-contoured restoration at the cervical margin. If excess space exists then it may be possible to add composite to the central incisor or canine teeth, particularly if they are also microdont. It is advisable to bond to as wide an area as possible, which can involve most of the surface area of the crown of the microdont lateral incisor.10 This also allows easier blending of the restorative-tooth margin.
The ideal labio-palatal and vertical position depends to a degree on the position of the contralateral tooth and the proposed anterior guidance at the end of treatment. Often it is desirable to provide symmetry to a smile as this is perceived to be aesthetic and so the final restored microdont lateral incisor should usually be similar in size, position and shape to the contralateral side. However, the desired position prior to restorative build-up can differ depending on the type of restoration that is planned. For example, if the microdont tooth is being built-up with composite resin, the vertical position of the incisal edge should be at the correct level so that there is reduced risk of fracture or chipping of the composite. Natural tooth structure would then form most of the incisal edge of the tooth rather than the weaker composite material. However, if an indirect veneer is to be constructed, then the incisal edge of the microdont lateral incisor should ideally be placed 1–2 mm apical to the final incisal level to allow sufficient space for the veneer without having to remove sound tooth structure. Of course, the gingival margin level will also need to be taken into account so that it is harmonious with the rest of the anterior teeth and a balance may need to be achieved between the optimal incisal position and the desired gingival margin level. In terms of anterior guidance, the microdont lateral incisor is usually kept out of any excursive movements, and thus should not be positioned in such a way that guiding contacts exist.
Accepting the moderately microdont upper lateral incisor and opting for orthodontic space closure but carrying out adjunctive interdental stripping of the lower labial segment. This will ensure that the decreased tooth tissue in the upper labial segment (resulting from the microdont lateral incisor) is compensated for by a corresponding reduction of the combined mesiodistal width of the lower incisor teeth. If sufficient interdental stripping is carried out to compensate for the microdont lateral incisor(s) then, in the absence of any other tooth size discrepancy, this should result in a Class I buccal segment.
As described previously, another method of taking up the extra spacing resulting from the diminutive upper lateral incisor teeth is to increase the torque in the upper labial segment either by using super torque brackets or by adding additional palatal root torque in the finishing stages of treatment. In the lower arch, use of McLaughlin, Bennett and Trevisi (MBT) brackets with six degrees of lingual crown torque can help reduce overproclination of the lower incisors and thereby minimize the effects of the diminutive upper lateral incisor teeth.
Accepting the moderately microdont upper lateral incisor teeth and opting for orthodontic space closure. This will again result in a tendency to a Class II buccal segment if there is a tooth size discrepancy or a reduced overjet.
Increasing the mesial angulation of the microdont lateral incisor tooth by adjusting the bracket position. This ensures that the microdont tooth occupies a greater mesiodistal width as it is mesially angulated as opposed to if the orthodontic bracket was placed at the correct FA (Facial-axis point). The FA point on a tooth has been proposed as a reference point for bracket positioning. A bracket positioned on the FA point of a microdont lateral incisor would allow for the crown to be more upright and thereby occupy less mesiodistal space. This orthodontic adjustment can be done at either of two stages of treatment:
At the time of the bracket placement. Placing the upper lateral incisor bracket on a microdont lateral incisor, to face distally by about 25°, will allow for greater mesial tip when an aligning archwire is engaged.
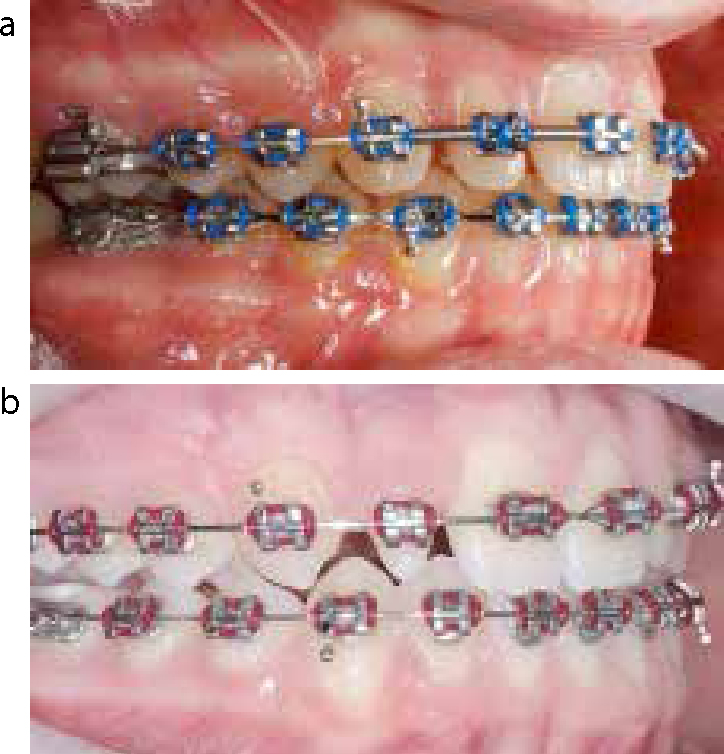
In the finishing stages of treatment a gable second-order bend can be placed in rectangular stainless steel wire on the microdont lateral incisor to allow it to tip mesially and thereby again result in the tooth occupying a greater mesiodistal width as opposed to if it was at its average inclination (Figure 8 a and b).These options for the management of a diminutive lateral and its effects on the buccal segment relationship are summarized in Table 1.
Extraction of the microdont tooth. This treatment approach may be considered if there is a space requirement or if the long-term prognosis of the significantly microdont lateral incisor tooth is poor. An assessment based on the clinical and radiographic features can be used to make this decision following discussion with the patient. If the lateral incisor has a small crown and is significantly tipped and rotated, or has a short thin root that is likely to undergo significant apical resorption during orthodontic treatment, then consideration can be given to its extraction. Extraction may also be considered if there is an additional morphological deformation, such as a dens invaginatus with pulpal disease. If the lateral incisor is to be extracted, then the options for management are canine substitution, a tooth-supported restoration and an implant-supported crown.
Orthodontic and restorative interdisciplinary treatment planning is important if consideration is given to extracting the microdont lateral incisor and masking the canine as a lateral incisor.11 Orthodontic treatment can position the teeth in the optimal functional and aesthetic position. A variety of factors are important when assessing the suitability of disguising a maxillary canine tooth as a lateral incisor. These include the anteroposterior relationship, the degree of crowding, the lip line, buccal segment interdigitation and orthodontic and restorative implications, such as the gingival margin relative to adjacent teeth, the colour, shape and bulbosity of the canines.
Figure 6.
(a) Diminutive upper laterals following orthodontic positioning. (b) Composite build-ups of the diminutive upper laterals. (c) Completion of orthodontic treatment.Figure 7.
(a) Microdont lateral incisor is moved into the middle of the space to allow for its build-up with composite resin. (b) Orthodontic treatment carried out to position the lateral incisor in the middle of the space.Figure 8.
(a) Gable bend to tip the diminutive upper lateral mesially. (b) Gable bend to tip the maxillary canine mesially to take up remaining space between UR3 and UR2.
Options
Possible Resulting Buccal Segment
Composite resin build-ups
Class I
Orthodontic space closure with interdental stripping of the lower incisors
Class I
Orthodontically tipping the diminutive lateral and canine to occupy greater mesiodistal dimension
Class I
Increasing palatal root torque in the upper labial segment
Class I
Orthodontic space closure alone without interdental stripping, palatal root torque or mesially tipping the maxillary canine and lateral
Class II
The anteroposterior incisor relationship
This is a factor in deciding whether to extract a diminutive lateral incisor as opposed to building it up with composite. For example, in a Class II malocclusion, if a diminutive upper lateral incisor is extracted, the resulting space can be utilized for overjet reduction or to provide space to torque the upper labial segment. However, in Class III malocclusions, closure of upper arch space following the extraction of a diminutive lateral incisor may worsen the incisor relationship by retracting the upper labial segment. In such circumstances, it may be better to maintain the diminutive upper lateral incisor in its current position and maintain the upper labial segment in a forward position to allow camouflage of the Class III malocclusion.
The degree of crowding
The space for the relief of moderate to severe crowding may be gained from an extraction approach. In situations where there is moderate crowding with a uni- or bilateral diminutive lateral incisor, consideration can be given to the extraction of the diminutive lateral incisor(s) to relieve the crowding. However, in situations where the maxillary arch demonstrates generalized spacing, it may be appropriate to localize this space in the lateral incisor region and allow a restorative build-up of the diminutive lateral incisor, or a prosthetic replacement if the lateral incisor is not suitable for a build-up.
The lip line
If the patient has a high smile line and reveals a greater gingival show on smiling, this is a factor to consider if the diminutive lateral is to be extracted and the canine masked as a lateral incisor (Figure 9). The gingival margin of the natural canine should, in such cases, be positioned more incisal to the central incisor gingival margin in order to mask it as a lateral incisor. This assumes the gingival margins of the teeth are visible on smiling and, in patients with a low smile line, the gingival level may be less important.12 It may be possible to alter the gingival margin by extruding the canine.13 However, both the palatal cingulum and cusp tip will need to be extruded and the extent to which this can be done is often a limiting factor on how much extrusion is feasible.
Figure 9. A high smile line revealing the gingival margins of the canines.
Buccal segment interdigitation
The occlusion in the buccal segment is another factor to be considered when deciding on extracting a diminutive lateral incisor and closing the space. Where the posterior teeth interdigitate well and the canine teeth are in a Class I relationship, it may be better to accept the diminutive lateral rather than opt to extract it and close the space.
Orthodontic implications
Orthodontic fixed appliances are indicated in cases of masking a canine as a lateral incisor in order to achieve 3-dimensional tooth movements. In such situations, either a lateral incisor bracket may be placed on the canine in order to torque the tooth root in a palatal direction, or an inverted canine bracket may be bonded to the canine in order to change the torque available from buccal to palatal root torque. These changes in bracket positioning are indicated in order to reduce the buccal emergence profile usually seen in maxillary canines to the more palatal lateral incisor profile. Thereafter, the canine cusp tip can be reduced or equilibrated over a sequence of visits.14
In addition, as the canine is being masked as the lateral incisor, similarly, the upper first premolar will need to be masked to appear like an upper canine. In such situations, the bracket in the upper first premolar can be placed more disto-gingivally in order to rotate the premolar so that it occupies a greater mesiodistal width and hence appears more like a maxillary canine. In addition, disto-gingival bracket placement on a maxillary first premolar will allow extrusion of the buccal cusp in order to make it appear more like a canine tip. Finally, during finishing, buccal root torque may be added to the first premolars.
Restorative implications
There are various restorative techniques that can be utilized to ‘convert’ the canine into a lateral incisor. The width of the canine can be reduced interproximally and reshaped by composite resin build-ups.15 According to the golden proportion philosophy of aesthetics, the maxillary lateral incisor teeth should be about 2/3 the size of the upper central incisors.16 It may therefore be necessary to reduce the size of the canine teeth but, ideally, any such recontouring should be confined within the enamel. If the canine is very large it may not be possible to achieve good aesthetics by moving it next to the central incisor.
The labial contour of canines is often bulbous therefore, in a canine substitution, the labial surface may need to be recontoured. Again this recontouring should be confined to enamel to avoid the need for restorations, such as veneers or crowns. More substantial reshaping can be achieved with composite, and modern restorative composite materials can provide an excellent and durable result. A degree of maintenance will be necessary, but this is often preferable to removing additional tooth structure for veneers or crowns. Again, the principle of bonding to a wide surface area should be applied to reduce the risk of delamination of the material and also to allow the material to blend into the tooth.
Maxillary canines are naturally darker in shade than incisors. If the colour of the canine needs to be lightened with bleaching techniques, the patient should be made aware of the need to repeat this periodically in the future. However, if bleaching is required it must be done prior to the composite build-ups.
Symmetry is another factor that needs to be considered if a canine tooth is to be disguised as a lateral incisor following extraction of the latter. The overall appearance may be compromised if it is carried out unilaterally, as there will be an asymmetric labial segment, with a large canine on the one side and an average-sized lateral incisor on the other. In such cases, a more aesthetically pleasing and symmetrical result may be achieved from extracting both diminutive lateral incisors and closing space, or by maintaining both diminutive lateral incisors and allowing for their restorative build-up.
Patient expectations from treatment
This very important factor in the management of microdont lateral incisors must not be overlooked. Involvement of the patient in developing informed consent is an integral aspect to carrying out successful treatment. This is particularly important in cases of microdont lateral incisors as a decision to build-up microdont teeth is likely to involve life-long restorative maintenance. Equally, extraction of a diminutive lateral incisor tooth needs to be taken in consultation with the patient because the ensuing replacement of the microdont lateral incisor tooth by an upper canine again has restorative implications and is not the treatment of choice in all cases.
This decision depends on taking into consideration the factors listed above that are required to camouflage the canine successfully as a lateral incisor, along with the patient's choice.
The factors to be considered when extraction of the diminutive lateral incisor is an option are summarized in Table 2.
Factors to consider
Spacing or crowding in the maxillary arch
The effect on the incisor relationship
The lip line
The suitability of masking the canine as a lateral incisor in terms of colour, bulbosity, gingival margin
The effect on the buccal segment relationship
The patient expectations
Summary
This paper has discussed the many aspects that should be considered when managing microdont lateral incisor teeth. Such teeth may be subclassifed as mildly microdont upper lateral incisors, where the mesiodistal width of the crown is about 2/3 the average width of an upper lateral incisor, or significantly microdont ‘peg laterals’, where the mesiodistal width of the crown is < 2/3 the average width of an upper lateral incisor. The effects of microdont lateral incisors may be spacing in the upper labial segment, a tendency to a Class II buccal segment relationship, an upper centre line shift to the side of the microdont tooth (if there is a single microdont lateral incisor), a reduced overjet and also a possible association with impacted upper canines. The management of microdont lateral incisors also needs consideration of the following factors: