Daou E. The elastomers for complete denture impression: a review of the literature. Saudi Dent J. 2010; 22:153-160
Guides to Standards in Prosthetic Dentistry – Complete and Partial Dentures. In: Ogden A (ed). London: Quintessence Publishing Co Ltd; 1996
Abree NS, Fleck S, Askinas SW. The results of a brief survey of complete denture prosthodontic techniques in predoctoral programs in North American dental schools. J Prosthodont. 1998; 5:219-225
Rao S, Chowdhary R, Mahoorkar S. Systematic review of impression technique for conventional complete dentures. J Ind Prosthodont Soc. 2010; 10:(2)105-111
Carlsson GE, Anders Ortorp A, Omar R. What is the evidence base for the efficacies of different complete denture impression procedures? A critical review. J Dent. 2013; 41:17-23
McCord JF, Grant AA. Impression Making. Br Dent J. 2000; 188:484-492
Sato Y, Tsuga K, Akagawa Y, Tenma H. A method for quantifying complete denture quality. J Prosthet Dent. 1998; 80:52-57
Hyde TP, McCord JF. Survey of prosthodontic impression procedures for complete dentures in general practice in the United Kingdom. J Prosthet Dent. 1999; 51:295-299
Duncan JP, Taylor TD. Teaching an abbreviated impression technique for complete dentures in an undergraduate dental curriculum. J Prosthet Dent. 2001; 85:121-125
Massad JJ, Cagna DR. Vinyl polysiloxane impression material in removable prosthodontics. Part 1: Edentulous impressions. Compend Contin Educ Dent. 2007; 28:(8)452-459
Rosentiel E. Rubber base elastic impression materials (a preliminary note). Br Dent J. 1955; 98:392-394
Smith DE, Toolson LB, Bolender CL One-step border molding of complete denture impressions using a polyether impression material. J Prosthet Dent. 1979; 41:347-351
Christensen GJ. Impression materials for complete and partial prosthodontics. Dent Clin North Am. 1984; 28:223-237
Appelbaum EM, Mehra RV. Clinical evaluation of polyvinylsiloxane for complete denture impressions. J Prosthet Dent. 1984; 52:537-539
Chaffee NR, Cooper LF, Felton DA. A technique for border moulding edentulous impressions using vinyl polysiloxane material. J Prosthodont. 1999; 8:129-134
Hayakawa I, Watanabe I. Impressions for complete dentures using new silicone impression materials. Quintessence Int. 2003; 34:177-180
Lynch CD, Allen PF. Management of the flabby ridge: using contemporary materials to solve an old problem. Br Dent J. 2006; 200:258-261
Terry ED, Winston WL. A review of contemporary impression materials and techniques. Dent Clin North Am. 2004; 48:(2)445-470
The purpose of the study was to use a simplified impression technique, which is an alternative to the conventional method for complete denture fabrication. This was introduced to reduce the number of patient visits, operator time, as well as to compare the efficacy of a simplified impression technique (single appointment impression) with the conventional method (two appointments – primary and final impression).
Clinical Relevance: The simplified edentulous impression technique reduces the number of patient visits when compared with the conventional technique, without compromising the principles of definitive impression-taking.
Article
An impression is a record of mouth tissues taken at an unstrained rest position or in various positions of displacement.1 The impression stage of constructing complete dentures is to design the denture bases to the optimum denture-supporting area and to ensure that the border form of the prostheses provides a functional peripheral seal. It is generally agreed by the British Society of Prosthodontics (BSSPD) in their guidelines that meeting these objectives achieves denture stability and retention, and enables effective function.2 Many different concepts and approaches have been described to achieve these goals, along with specific materials and techniques by which the given objectives might be accomplished. Even though there are wide variations in individual preferences for a particular material or method, most US dental schools believe that, for a successful outcome, a two-appointment (primary and final impression) procedure is required.3 However, there is a lack of strong evidence as to whether one material is superior or a particular technique would produce better long-term results in terms of complete denture performance.4
Improvements in the impression technique promote the need for new impression materials and, sometimes, the development of new material, leading to an improved impression technique.5 This paper describes a clinical study of taking a final impression directly using putty and light body rubber base materials.
Methods
This study was conducted in the Department of Prosthodontics at MS Ramaiah Dental College and Hospital. Ethical clearance was obtained. After obtaining informed consent, the study subjects included were 70 completely edentulous patients aged between 50 and 80 years of age with a completely healed denture-bearing area, moderate to well-formed ridges and adequate inter-arch space. Patients with pain in the denture-bearing area, resorbed foundations, flabby and hyperplastic tissues, poor neuromuscular control, unfavourable ridge relationships, uncontrolled diabetes, diseases related to calcium metabolism, xerostomia and temporomandibular joint disorders were excluded.
Complete denture patients were randomly divided into Group A (35 patients) and Group B (35 patients) and assigned to final year undergraduates and first year postgraduate students for treatment. The Group A patients were treated by undergraduates as well as postgraduates with a conventional impression technique (Control group) in which primary impressions were taken using impression compound in the first sitting. Custom-tray fabricated in acrylic with wax spacer and stoppers was used for border moulding with greenstick compound and wash impression was made using zinc oxide eugenol impression paste in the second sitting. The same students also treated another 35 patients with the simplified impression technique (Study group) using vinyl polysiloxane (Betasil Vario, Muller-Omicron Gmbh & Co KG) of two different consistencies:
soft putty; and
light body (light-bodied consistency) in a single sitting.
The simplified technique makes use of perforated stock trays of proper size for the edentulous arch (Figure 1). They are modified with pliers, so that they almost enclose all the required anatomical structures without impingement.6 Tissue stoppers of 5 mm length made using modelling wax are placed in the canine and molar region (Figure 2). These stops are developed to achieve an even space of about 3–4 mm between the tray and edentulous tissues and to keep the tray steady during impression-taking. The mandibular tray borders should cover the retromolar pad, external oblique ridge, and mylohyoid ridge. The deficient tray borders are extended with soft utility wax but fall well short of the sulcular tissues by 2–3 mm (Figure 3). After applying tray adhesive, equal amounts of base and catalyst of soft putty impression material is mixed and loaded on to the tray evenly. The impression is made by ensuring complete seating of the tray as practised previously and removed after complete setting (Figure 4). All the borders should are moulded according to functional sulcus depth and width. Once set, deficient borders are corrected by adding putty and remoulding (Figure 5). Bulky and overextended borders are marked (Figures 6 and 7) for trimming with a sharp knife. The tissue surface of the impression is reduced by 1 mm with a tungsten carbide trimmer to give adequate relief and make space for light body material except in the maxillary posterior seal area. Finally, all the borders of the maxillary and mandibular impression are reduced by 1 mm with the same trimmer, and frenum areas slightly opened with an acrylic fissure bur to make space for light body material (Figure 8). This is done, as the displaceability of the sulcular tissues varies and the development of physiologic borders with putty may be difficult to achieve due to its viscosity. When the maxillary palatal area is high vaulted, vent holes may be placed through the tray to prevent air entrapment. Light body elastomeric impression material is evenly loaded on the same tray and final impressions are taken (Figure 9).
Figure 1. Edentulous stock trays with flanges that can be altered with pliers.Figure 2. Tray orientation with wax stops.Figure 3. Tray borders extended with utility wax in deficient areas (arrows).Figure 4. Putty primary impressions showing deficient borders in maxillary anterior area.Figure 5. Addition of putty to deficient areas of maxillary impression (arrows).Figure 6. Overextensions marked with maxillary impression.Figure 7. Overextensions marked with mandibular impression.Figure 8. Borders of both impressions trimmed with a tungsten carbide trimmer; impression surface also modified.Figure 9. Definitive impressions.
Results
The mean number of visits required to fabricate the dentures by undergraduates and postgraduates is shown in Tables 1 and 2. Mann-Whitney and Wilcoxon tests showed that the number of visits required to make dentures was significantly less (p < 0.05) with the simplified impression technique for most of the undergraduates and some of the postgraduates (Tables 3 and 4).
Methods
Mean
N
Standard Deviation (SD)
Conventional
6.18
11
0.874
Simplified
4.82
11
0.751
Total
5.50
22
1.058
Methods
PG1
PG2
PG3
PG4
PG5
PG6
Conventional
MeanNSD
5.500040.5774
5.750040.9574
5.50040.5774
6.000040.8165
6.750040.9574
6.000040.8165
Simplified
MeanNSD
4.500040.5774
4.250040.5000
4.750040.5000
4.250040.5000
5.000041.1547
4.250040.5000
Total
MeanNSD
5.000080.7559
5.000081.0690
5.125080.6409
5.125081.1260
5.875081.3562
5.125081.1260
Ranks
Methods
N
Mean Rank
Sum of Ranks
VISITS
Conventional
11
15.64
172.00
Simplified
11
7.36
81.00
Total
22
Not corrected for ties.
Grouping Variable: Methods
The two methods differ significantly as p = 0.002 < 0.05
Methods for PG
N
Mean Rank
Sum of Ranks
PG1
ConventionalSimplifiedTotal
448
6.003.00
24.0012.00
PG2
ConventionalSimplifiedTotal
448
6.252.75
25.0011.00
PG3
ConventionalSimplifiedTotal
448
5.753.75
23.0013.00
PG4
ConventionalSimplifiedTotal
448
6.382.63
25.5010.50
PG5
ConventionalSimplifiedTotal
448
6.003.00
24.0012.00
PG6
ConventionalSimplifiedTotal
448
6.382.63
25.5010.50
Not corrected for ties.
Grouping Variable: Methods for PG
There is no significant difference between methods in the case of PG1, PG2, PG3, PG5 as p > 0.05. There is a significant difference between methods in the case of PG4 and PG6.
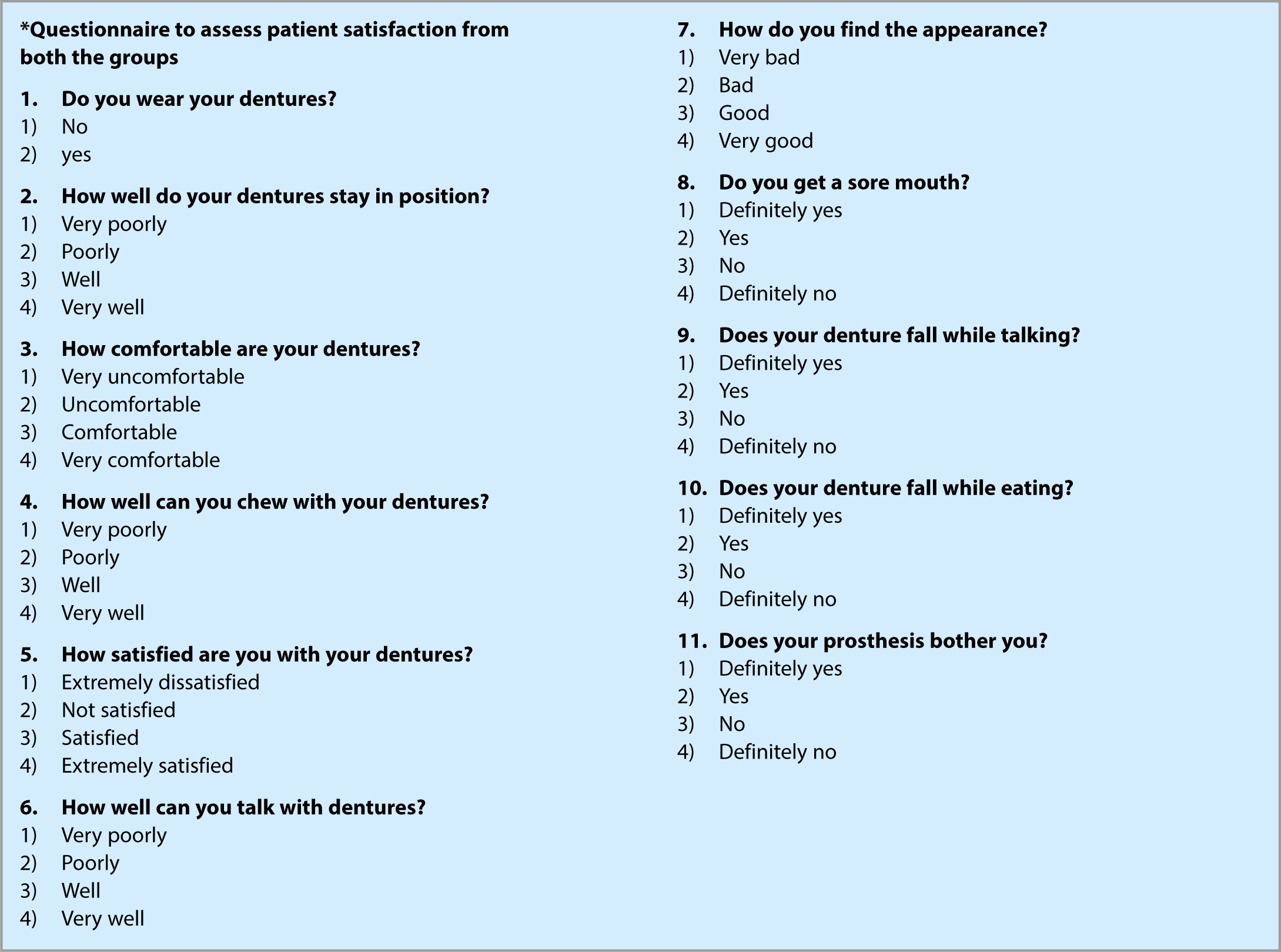
Patient satisfaction
This was assessed using a *Questionnaire (p848) after the new denture was worn for two months. Patients from both groups replied to the questionnaire and the interpretation is shown in Table 5. Answers to the questionnaires did not differ significantly between group A and group B patients. In answer to the first question, ‘Do you wear your dentures?’, around 91.4% of the study group and 94.3% of the control group, answered ‘Yes’. When asked ‘How well do your dentures stay in position?’, around 93.8% of the study group and 100% of the control group answered very well to well. In answer to the question ‘How well can you chew with your dentures?’, 87.6% of the study group and 90.9% of the control group could chew very well to well with their dentures. Around 100% of the study group and 97% of the control group were not getting any sore mouth symptoms with their new dentures.
Questionnaire
Putty impression(%)
Conventional(%)
Chi-squared value
p-value
1. Do you wear your dentures?
No
8.6
94.3
0.215
0.643
Yes
91.4
94.3
2. How well do your dentures stay in position?
Very poorly
0
0
2.137
0.343
Poorly
6.2
0
Well
43.8
45.5
Very well
50.0
54.5
3. How comfortable are your dentures?
Very uncomfortable
0
0
1.373
0.503
Uncomfortable
6.2
3.0
Comfortable
59.4
72.7
Very comfortable
34.4
24.2
4. How well can you chew with your dentures?
Very poorly
0
0
1.818
0.403
Poorly
12.5
9.1
Well
68.8
57.6
Very well
18.8
33.3
5. How satisfied are you with your dentures?
Extremely dissatisfied
0
0
0.007
0.997
Not satisfied
6.2
6.1
Satisfied
68.8
69.7
Extremely satisfied
25.0
24.2
6. How well can you talk with dentures?
Very poorly
3.1
0
6.759
0.080
Poorly
9.4
0
Well
53.1
78.8
Very well
34.4
21.2
7. How do you find the appearance?
Very bad
0
0
3.317
0.190
Bad
0
3.0
Good
50.0
66.7
Very good
50.0
30.3
8. Do you get a sore mouth?
Yes
0
3
5.933
0.051
No
59.4
81.8
Definitely no
40.6
15.2
9. Does your denture fall while talking?
Yes
3.1
3.0
4.729
0.094
No
46.9
72.7
Definitely no
50.0
24.2
10. Does your denture fall while eating?
Yes
6.2
0
3.893
0.143
No
65.6
84.4
Definitely no
28.1
15.6
11. Does your prosthesis bother you?
Yes
15.6
12.1
1.266
0.531
No
53.1
66.7
Definitely no
31.2
21.2
Retention and stability tests
An experienced operator, who was blindfolded in the trial, conducted retention and stability tests7 for all the patients participating in the study.
Test for denture retention
In the retention test the dentures are checked for dislodgement by a vertical pull on central incisors after the teeth are dried with gauze. Of both the study and the control groups 86%, with respect to maxillary dentures, were well retentive and 14% moderately retentive. For the mandibular denture, 12% of the study group and 26% of the control group was well retentive, whereas 83% of the study group and 74% of the control showed moderate retention. About 5% of the study group showed poor retention with mandibular dentures (Table 6).
Denture
Impression Technique
Retention (%)
Chi-Squared Value
p-Value
Poor
Retentive
Well Retentive
Maxilla
Simplified Impression
0
14.3
85.7
<0.0001
1.000
Conventional
0
14.3
85.7
Mandible
Simplified Impression
5.7
82.9
11.4
4.087
0.1
Conventional
0
74.3
25.7
Test for denture stability
In the stability test the dentures are checked for movement induced by index and middle finger pressure on the first molar teeth. (First, a direct pressure is applied equally on both sides; then a direct pressure is applied alternately on both sides; and then a rotational force is applied.) Around 94% of group A and 89% of group B, with respect to maxillary dentures, showed good stability, whereas 6% of group A and 11% of group B showed moderate stability. With mandibular dentures, about 60% of both group A and group B exhibited good stability and 40% of both the groups displayed moderate stability (Table 7).
Denture
Impression Technique
Stability (%)
Chi-Squared Value
p Value
Poor
Moderate Stability
Good Stability
Maxilla
Simplified Impression
0
5.7
94.3
0.729
0.3
Conventional
0
11.4
88.6
Mandible
Simplified Impression
0
40.0
60.0
<0.0001
1.000
Conventional
0
40.0
60.0
The values of retention and stability do not show any significant difference between the two groups.
Discussion
A precise complete denture impression is one of the most critical factors in determining success or failure of the dentures. Most textbooks advocate a two-stage procedure where a preliminary impression is taken, often with an irreversible hydrocolloid (alginate) in a stock tray and a final impression is recorded using a custom-tray, usually made of acrylic resin. There are many materials for the final impression, such as zinc oxide and eugenol (ZOE) paste, polysulphide rubber, polyether, polyvinylsiloxane and alginate. Preferences vary among dentists. These impression appointments are generally considered as more time consuming and technically difficult in the conventional treatment sequence for complete dentures.3, 8,9,10
Research has proved that, without increasing the number of post-insertion appointments or reline procedures, the abbreviated impression technique significantly reduces the number of visits for fabricating complete dentures.9,10 A retrospective study conducted in an undergraduate dental school compared the treatment results between edentulous patients wearing complete dentures made from a traditional two-stage technique, and another edentulous group whose impressions were taken from an abbreviated technique. The abbreviated technique involved taking overextended, irreversible hydrocolloid impressions in stock trays. Heat processed acrylic resin denture bases were fabricated on the casts obtained. In the second visit, jaw relation records were made using these bases after checking their retention, stability and border extensions using pressure-indicating paste. After the aesthetic try-in, the teeth were heat processed on to the denture base. The study concluded that teaching an abbreviated impression technique in an undergraduate clinic helped to decrease the number of patient appointments, without increasing the number of adjustment or reline procedures.9
In another recent technique, called a VPS Edentulous Impression Technique,10 vinyl polysiloxane of multiple viscosities were used in stock polystyrene-based polymer trays, which could be softened through a flame or easily trimmed with an acrylic trimmer for proper adaptation to the edentulous tissues. Border moulding was achieved by placing a rope of high viscosity VPS along the maxillary tray border and medium viscosity for mandibular tray borders. Definitive or final impressions were made using low viscosity VPS. The VPS technique has the inherent disadvantage of using specific trays that may not be readily available and are possibly expensive. The use of multiple viscosities also may be confusing to the general practitioner.
Today, two of the most popular elastomers used in dental practice are the polyethers and/or vinyl polysiloxane. The popularity of the elastomer materials is acceptable, given the combination of excellent physical properties, handling characteristics, and better dimensional stability.
The use of polyether11,12 or vinyl polysiloxane (VPS)13,14,15,16,17 impression materials for custom-tray border correction has been described extensively in the literature.
The introduction of these elastomers have made way for newer techniques of edentulous impression-taking, which has remained unchanged for decades. Vinyl polysiloxane offers a number of distinct advantages for making definitive impressions during complete denture therapy:18
The material is available in different viscosities;
Sequential addition of new impression material to existing cured material in the tray will effectively adhere when polymerized;
VPS can be cut back and laminated to improve contours similar to modelling plastic;
It has optimum material properties, such as accuracy, dimensional stability, elastic recovery, flow, flexibility, workability, hydrophilic nature, a long shelf life, patient comfort, taste and smell;
It is also the most accurate for second pour among all elastomers.
Polyvinylsiloxane putty and light-body impression material are well suited for taking complete denture impressions and good results were obtained with less expenditure of time, as well as less discomfort and inconvenience for the patient. In addition, the odour, taste and colour of the polysiloxane materials improved patient acceptability and gave an easy to use result.1
Fewer visits for treatment would mean improvement in patient compliance and motivation. This reduction in appointments improves clinical revenue, whether in a general or a specialty practice. Moreover the fabrication of custom-trays with autopolymerizing resin in undergraduate dental schools has the disadvantage of possible high levels of monomer release and concerns of health and occupational safety.5 Implementation of the simplified impression technique can be a good solution.
However, the application of the simplified technique should be restricted to well-formed and moderate edentulous foundations, since modification of stock metal trays to conform to resorbed edentulous ridges will be difficult. Custom-trays are to be used when the edentulous foundations are resorbed or demonstrate excessively flabby tissues.
Conclusion
Within the limitations of this study, there was no significant difference between the groups treated with either the conventional method or the simplified impression method in terms of patient satisfaction, retention and stability. Hence, dentures made using the simplified impression technique are probably less time consuming, which benefits both patient and operator. Therefore, for moderate to well-formed ridges, the simplified edentulous one appointment impression technique can be used in place of the traditional two-appointment technique, without compromising the principles of definitive impression-taking.