Miles DA, Lovas JL, Cohen MM. Hemimaxillofacial dysplasia: a newly recognised disorder of facial asymmetry, hypertricosis of the facial skin, unilateral enlargement of the maxilla, and hypoplastic teeth in two patients. Oral Surg Oral Med Oral Pathol. 1987; 64:445-448
Danforth RA, Raymond JM, Abrams AM, Handlers JP. Segmental odontomaxillary dysplasia. Report of eight cases and comparison with hemimaxillofacial dysplasia. Oral Surg Oral Med Oral Pathol. 1990; 770:81-85
Prusack N, Pringle G, Scotti V, Chen S. Segmental odontomaxillary dysplasia. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90:483-488
Kahn M. Basic Oral and Maxillofacial Pathology. 2001; 1
Cahuana A, Gonzalez Y, Palma C. Clinical management of regional odontodysplasia. Pediatr Dent. 2005; 27:34-39
Crawford PJM, Aldred MJ. Regional odontodysplasia: a bibliography. J Oral Pathol Med. 1989; 18:251-263
Tervonen SA, Stratmann U, Mokrys K, Reichart PA. Regional odontodysplasia: a review of the literature and report of four cases. Clin Oral Invest. 2004; 8:45-51
Packota GV, Pharoah MJ, Petrikowski CG. Radiographic features of segmental odontomaxillary dysplasia: a study of 12 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1996; 82:577-584
Armstrong C, Napier SS, Boyd RC, Gregg TA. Histopathology of the teeth in segmental odontomaxillary dysplasia, new findings. J Oral Pathol Med. 2004; 33:246-248
Sadeghi EM, Ashrafi MH. Regional odontodysplasia: clinical, pathologic and therapeutic considerations. J Am Dent Assoc. 1981; 102:336-340
Jones CJ, Ford JF. Simultaneous occurrence of segmental odontomaxillary dysplasia and Becker's nevus. J Oral Maxiollfac Surg. 1999; 57:1251-1252
Paticoff K, Marion RW, Shprintzen RJ, Shanske AL, Eisig BS. Hemimaxillofacial dyplasia. A report of 2 cases and a further delineation of the disorder. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 83:484-488
Bhatia SK, Drage N, Cronin AJ, Hunter ML. Case report: segmental odontomaxillary dysplasia – a rare disorder. Eur Arch Paediatr Dent. 2008; 9:(4)245-248
Comparative case report of segmental odontomaxillary dysplasia and regional odontodysplasia Stephanie L Clark Alison M Cairns Keith D Hunter Dental Update 2024 41:9, 707-709.
Authors
Stephanie LClark
BDS, MFDS RCPSG, MPaedDent
Specialist Paediatric Dentist, Glasgow Dental Hospital and School
The clinical and radiological features of segmental odontomaxillary dysplasia (SOD) are well described but the condition is probably under recognized owing to misdiagnosis as an atypical form of regional odontodysplasia (ROD). Two cases are compared to highlight the differences between SOD and ROD. The clinical, radiographic and histological findings are compared using case reports of a 6-year-old male with SOD and a 4-year-old girl with ROD. Treatment and follow-up for these patients is described, along with a comparative review of the major characteristics of these two rare conditions.
Clinical Relevance: To help the paediatric dentist distinguish between these two rare conditions.
Article
Developmental disorders involving segments of the developing dentition and their associated structures are rare and, consequently, there is potential for confusion to arise. Two such conditions are segmental odontomaxillary dysplasia (SOD) and regional odontodysplasia (ROD).
SOD is a rare unilateral developmental disorder of the maxilla, involving abnormal growth and maturation of the bone, the teeth and covering gingiva. There are specific clinical, radiographic and histological characteristics. The condition was initially reported as hemimaxillofacial dysplasia by Miles et al in 1987.1 This was revised by Danforth et al in 19902 to the current definition which takes better account of the dental findings.
A review of the literature by Prusack et al3 in 2000 reported 26 cases of SOD. They found SOD to be a non-progressive developmental disorder limited to a posterior segment of the maxilla, resulting in:
Mild fibrous and/or bony expansion of the maxilla;
Loss of one or more premolars;
Variable alteration of primary molars; and
Delayed eruption of permanent teeth.
The condition is probably under recognized as it may be misdiagnosed as hemimaxillofacial dysplasia (HMD), fibrous dysplasia (FD), hemifacial hyperplasia or regional odontodysplasia (ROD).4 These conditions are described more fully in the discussion.
ROD is a rare localized developmental anomaly of the dental tissues with specific clinical, radiographic and histological characteristics.5 The condition was first described in 1934. It was not until 1963 that Zagarelli et al coined the term ‘odontodysplasia’ and Pindorg later added the prefix ‘regional’ in 1970.6 ROD has been reported in association with a number of rare conditions and syndromes, eg vascular naevi, haemangioma, epidermal naevus syndrome, hypophosphatasia, ectodermal dysplasia and hydrocephalus.7
The characteristic clinical findings include failure or delay of dental eruption, discoloured and atypically shaped teeth with abscesses or fistulae in the absence of caries. Enamel and dentine are hypomineralized and hypoplastic, so that the ‘ghost teeth’ appear shadowy on radiographs with wide pulp chambers.8
The following cases have been collated in order to highlight the similarities and differences between these two rare conditions.
Case reports
Case 1: SOD
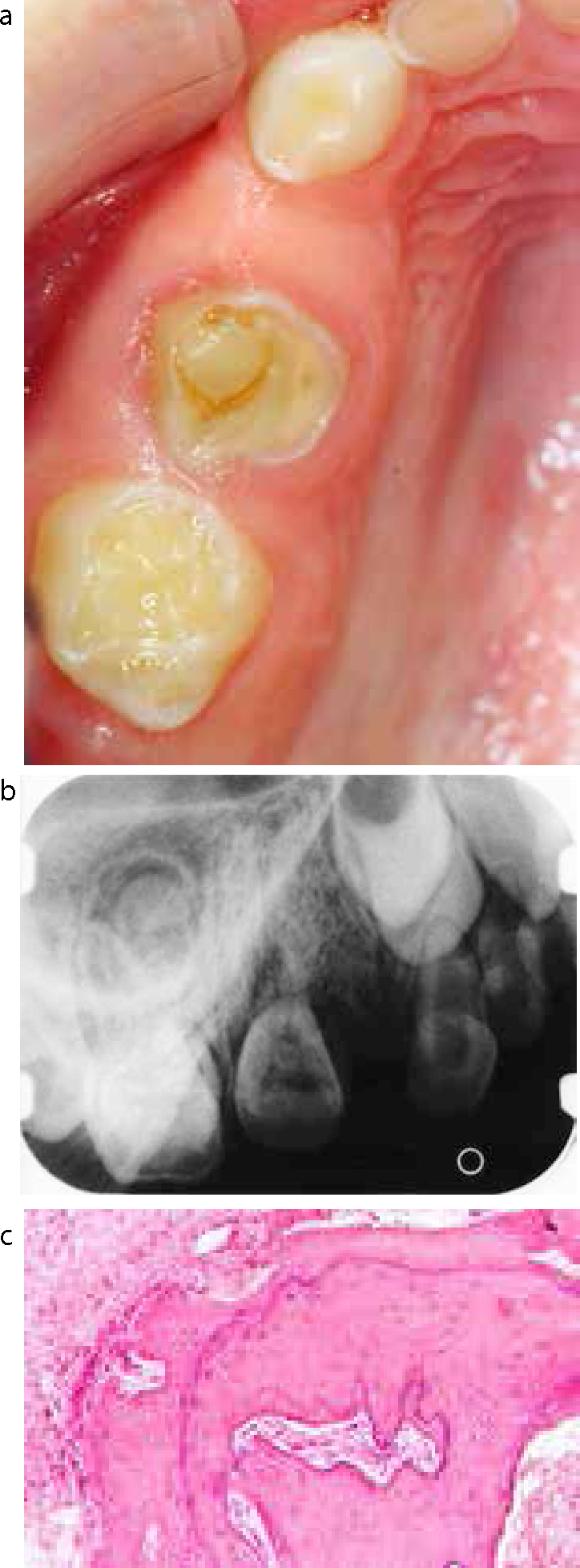
A 6-year-old healthy Caucasian male was referred to the paediatric dentistry department complaining of a bony swelling in the right maxilla (Figure 1a). On examination he had good oral hygiene, and had a full primary dentition along with both lower first permanent molars.
Figure 1.
(a) Intra-oral photograph of SOD showing bucco-palatal expansion of the right maxilla. (b) Periapical radiograph of SOD showing a segment of right maxilla which shows abnormal bone quality, missing UR4 and delayed eruption of UR6. (c) Photomicrograph of bone from patient with SOD, showing woven bone and prominent reversal lines. (Decalcified H&E x2).
He was caries free and had a restoration in the URD. There was generalized toothwear. The URD and URE were spaced and there was a hard bony expansion bucco-palatally in this region as well as gingival enlargement. Radiographic investigation revealed:
For a definitive diagnosis and to exclude FD, the patient was referred for surgical exploration of the bony expansion in the right maxilla under general anaesthetic (GA). The URD was extracted, along with attached soft tissue and separate bone fragments which were sent for histological examination (Figure 1c). The tooth fragments showed dentine with abnormally wide tubules in places and resorption of parts of the tooth with evidence of attempted repair by osteodentine. The bone was vital with a mixture of lamellar and woven bone with prominent reversal lines. There was no evidence to suggest a diagnosis of FD. These features are non-specific, but in combination with the clinical and radiographic features, a diagnosis of SOD was made.
Follow-up
The patient has been reviewed regularly for the last two years without complication. There has been no increase in the bucco-palatal width of the right maxillary alveolus, the UR6 has fully erupted and the alveolar bone around the URD has healed well.
Case 2: ROD
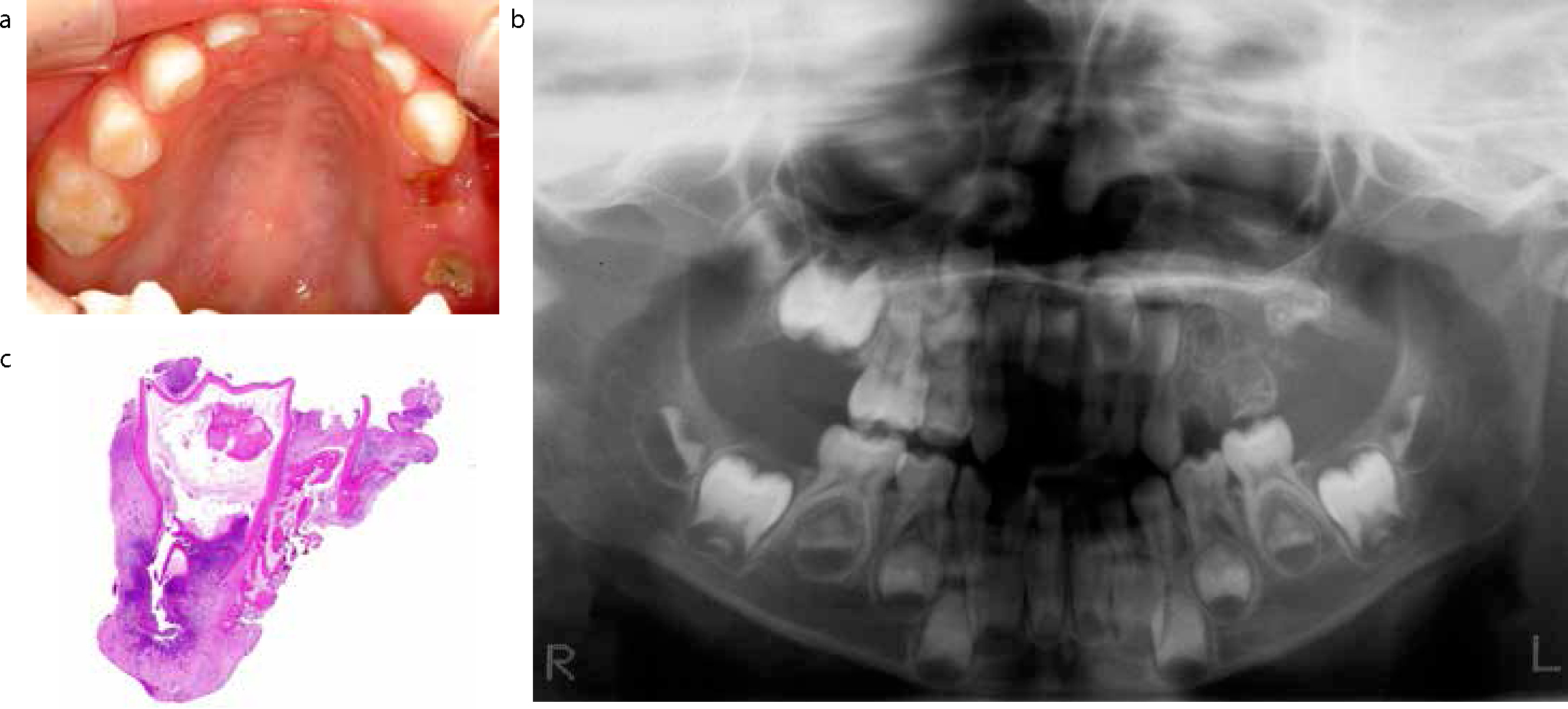
A 4-year-old healthy Caucasian girl was referred due to pain and swelling in the upper left quadrant and missing teeth (Figure 2a). On examination, she had a full primary dentition but the ULD and ULE were found to be badly broken down in a mouth which was otherwise caries-free. Radiographically, permanent successors in the upper left quadrant were not forming as expected at this stage, in comparison with other areas of the jaws. ‘Ghost-like’ outlines of the UL3, 4, 5, 6 and ULD, E were present, with all dental hard tissues affected (Figure 2b.)
Figure 2.
(a) Intra-oral photograph of ROD showing the upper arch and broken down ULD and ULE and associated abscess in an otherwise caries-free dentition. (b) OPG of RODshowing ‘ghost-like’ outlines of the UL3, 4, 5, 6. (c) Photomicrograph of a decalcified section of a tooth from patient with ROD. The image shows a ‘ghost tooth’ with associated periapical inflammation. (H&E x2).
Treatment
She was also referred for GA extraction of the ULD and ULE, along with bony curettage that were sent for histological examination. The submitted teeth had large pulp chambers with a thin abnormal dentine shell. The enamel was structurally very abnormal with small enameloid masses in the surrounding soft tissue (Figure 2c). The combination of clinical, radiographic and histological features led to a diagnosis of ROD.
Follow-up
The patient was reviewed after the extraction of these teeth with no further complications.
Discussion
SOD is probably under recognized as it may be misdiagnosed as hemimaxillofacial dysplasia (HMD), fibrous dysplasia (FD), hemifacial hyperplasia or regional odontodysplasia (ROD). In HMD, ipsilateral facial hypertrichosis (abnormal amount of hair growth) is present in addition to the SOD symptoms. FD causes enlargement of bone tissue, and affected bone growth is out of proportion with that of unaffected bones, and tooth malformations and missing premolars are not characteristic of the disease. Hemifacial hyperplasia results in unilateral facial enlargement and precocious eruption and enlarged teeth in the affected region.4
Table 1 compares and contrasts the main features of SOD and ROD.
SOD
ROD
Clinical
Affects bone, teeth and gingiva
Fibrous and/or bony expansion of the posterior segment of the maxilla
Always unilateral
Variable alteration of primary molars, eg spacing, hypoplasia
Delayed eruption of permanent teeth
Affects teeth only
No bony expansion
Can affect the maxilla and mandible
Unilateral (rarely crosses the midline)
Teeth present – small, brown, grooved and hypoplastic
Abscesses or fistula in the absence of caries
Eruption delay and failure
Radiographic
Sclerosis, increased density of bone with and thickened trabeculae
Missing permanent teeth
Reduced size of maxillary antrum
‘Ghost teeth’ – thinning of enamel dentine layers
Histological
Woven bone with reversal lines, lacking osteoblastic and osteoclastic rimming
Bone is normal. Dentine is dysplastic with irregular tubules, large areas of globular and interglobular dentine and a widened predentine layer. Enamel is variably present and is abnormal.
Most cases of SOD are diagnosed in childhood or adolescence,2 and there is no predilection for gender. It has been described as non-progressive and the long-term outcome remains largely unknown.3 SOD is characterized by abnormal growth and maturation of the bone, teeth and the covering gingiva. It mainly affects the posterior segment of the maxilla, causing bucco-palatal expansion of the alveolus and gingival fibrous hyperplasia, which can result in facial asymmetry.3 Other features include delayed eruption, most commonly of the first permanent molars,3,9 hypoplasia of primary teeth and absence of one or more premolars in the affected segment.3 The primary molars often have abnormal morphology and are spaced due to segmental expansion.1,2 The most useful radiographic findings for diagnosing SOD are the following:
Sclerosis or increased density of bone with thickened trabeculae;
Vertical orientation of bony trabeculae;
Absent premolars;
Delayed eruption or displacement of other permanent teeth;
Histological findings for SOD show that the bone is immature, woven bone with reversal lines, lacking osteoblastic and osteoclastic rimming.6 The primary teeth show enlargement of pulps and an irregular pulp/dentine interface. Tubular defects in the coronal dentine are present and widespread external resorption is also observed.10
ROD affects both the primary and permanent dentitions.5 The age at time of diagnosis varies between 4 and 23 years, and females are more often affected than males at a ratio of 1.7:1.8 The maxilla is typically affected twice as often as the mandible and is usually unilateral and rarely crosses the midline. The teeth are likely to be small, brown, grooved and hypoplastic. Eruption failure or delay is frequently seen, as well as abscesses or fistulae in the absence of caries.5 Radiographically, the teeth are hypoplastic with thin layers of enamel and dentine around a large pulp chamber, giving them a ‘ghostly’ appearance. Pulp calcifications may be identified in the coronal pulp, and periapical lesions can develop in association with the anomalous teeth.5,11 Histologically, the dentine is dysplastic with irregular tubules and there are large areas of globular and interglobular dentine and a widened predentine layer. Enamel is variably present and is abnormal with enameloid masses in the associated soft tissue.5
For both conditions, the aetiology and pathogenesis is largely unknown, although several factors have been suggested. In both cases, developmental problems during pregnancy have been suggested,6,9 along with cell mutations affecting ectodermal and mesodermal tissues.6,12 SOD has been associated with unilateral defects of the branchial arches.13
Treatment of SOD and ROD varies and requires to be tailored to the individual case. There have been no publications regarding the best treatment for patients with SOD as so few have been reported with long-term follow-up. The majority of reported cases had undergone bone biopsy to aid diagnosis, however, due to the benign nature of this developmental disorder and classical radiographic features, it may not be necessary. Long-term treatment will require a multidisciplinary approach. An osteoplasty may be required if the swelling is large and this should be done after growth has stopped. If there are missing teeth with spacing, the space can be managed by orthodontic or prosthetic treatment.
In a child with ROD, conservative treatment should be applied to keep the teeth for as long as possible to allow normal jaw development. However, if teeth have to be extracted, it is recommended that edentulous areas be restored with an acrylic removable appliance to maintain aesthetics and masticatory function. As the bone itself is not affected, autotransplantation is an effective treatment option and has been used successfully in some patients with ROD.5 Osseo-integrated implants would be a viable option after pubertal growth.
No treatment protocol has been established for either diagnosis since treatment has to be based on the degree of SOD or ROD, characteristics of the affected areas and the aesthetic and functional needs of each case.5,14
Conclusion
SOD and ROD may appear clinically similar but further knowledge of these two rare diseases should allow the dentist to distinguish between them and refer or manage appropriately.
Tracking and long-term management of patients with SOD and ROD is vital to understand more fully the progression of the two diseases. Regular monitoring of the patient with clinical and radiographic examinations is essential. Future management will require a multidisciplinary approach, depending on the patient's needs.14
Long-term follow-up of each documented case is encouraged to provide guidance in the management of these rare disorders.