Maintaining Standards. Guidance to Dentists on Professional and Personal Conduct. amended 2001: Section 4.8. 1997;
Standards for Conscious Sedation in Dentistry: Alternative Techniques. A Report from the Standing Committee on Sedation for Dentistry. 2007;
Woolf CJ, Salter MW. Neuronal plasticity: increasing the gain in pain. Science. 2000; 288:(5472)1765-1769
Woolf CJ. Pain: moving from symptom control toward mechanism-specific pharmacologic management. Ann Intern Med. 2004; 140:441-451
Marbach JJ. Is phantom tooth pain a deafferentation (neuropathic) syndrome? Part I: Evidence derived from pathophysiology and treatment. Oral Surg Oral Med Oral Pathol. 1993; 75:(1)95-105
Loggia ML, Schweinhardt P, Villemure C Effects of psychological state on pain perception in the dental environment. J Can Dent Assoc. 2008; 74:(7)651-656
Heap M, Alden P, Walker LG. The Nature of Hypnosis.Leicester: British Psychological Society; 2001
Mackey EF. Effects of hypnosis as an adjunct to intravenous sedation for third molar extraction: a randomized, blind, controlled study. Int J Clin Exp Hypn. 2010; 58:(1)21-38
Faymonville ME, Mambourg PH, Joris J Psychological approaches during conscious sedation. Hypnosis versus stress reducing strategies: a prospective randomized study. Pain. 1997; 73:361-367
Piccionne C, Hilgard ER, Zimbardo PG. On the degree of stability of measured hypnotizability over a 25 year period. J Personality Social Psychol. 1989; 56:289-295
NIH Consensus Development Panel on Acupuncture. J Am Med Assoc. 1998; 280:1518-1524
Tavares MG, Machado AP, Motta BG Electro-acupuncture efficacy on pain control after mandibular third molar surgery. Braz Dent J. 2007; 18:(2)158-162
Kitade T, Ohyabu H. Analgesic effects of acupuncture on pain after mandibular wisdom tooth extraction. Acupunct Electrother Res. 2000; 25:(2)109-115
Lao L, Bergman S, Hamilton GR Evaluation of acupuncture for pain control after oral surgery: a placebo-controlled trial. Arch Otolaryngol Head Neck Surg. 1999; 125:(5)567-572
Ekblom A, Hansson P, Thomsson M Increased postoperative pain and consumption of analgesics following acupuncture. Pain. 1991; 44:(3)241-247
Dickenson AH. Mechanisms of the analgesic actions of opiates and opioids. Br Med Bull. 1991; 47:(3)690-702
British National Formulary (No. 62). 2011;
Hargreaves KM, Keiser K. Development of new pain management strategies. J Dent Educ. 2002; 66:(1)113-121
Hargreaves KM, Abbott PV. Drugs for pain management in dentistry. Aust Dent J. 2005; 50:S14-S22
, 2nd edn. Geneva: WHO; 1996
Urquhart E. Analgesic agents and strategies in the dental pain model. J Dent. 1994; 22:336-341
Weil K, Hooper L, Afzal Z Paracetamol for pain relief after surgical removal of lower wisdom teeth. Cochrane Database Syst Rev. 2007; (3) https://doi.org/10.1002/14651858.CD004487.pub2
Toms L, Derry S, Moore RA Single dose oral paracetamol (acetaminophen) with codeine for postoperative pain in adults. Cochrane Database Syst Rev. 2009; (1) https://doi.org/10.1002/14651858.CD001547.pub2
Ahmad N, Grad HA, Haas DA The efficacy of non-opioid analgesics for postoperative dental pain: a meta-analysis. Anesth Prog. 1997; 44:(4)119-126
Moore RA, Edwards J, Derry S Single dose oral dihydrocodeine for acute postoperative pain. Cochrane Database Syst Rev. 2000; (2) https://doi.org/10.1002/14651858.CD002760
Mehlisch DR, Aspley S, Daniels SE Comparison of the analgesic efficacy of concurrent ibuprofen and paracetamol with ibuprofen or paracetamol alone in the management of moderate to severe acute postoperative dental pain in adolescents and adults: a randomized, double-blind, placebo-controlled, parallel-group, single-dose, two-center, modified factorial study. Clin Ther. 2010; 32:(5)882-895
Daniels SE, Goulder MA, Aspley S A randomised, five-parallel-group, placebo-controlled trial comparing the efficacy and tolerability of analgesic combinations including a novel single-tablet combination of ibuprofen/paracetamol for postoperative dental pain. Pain. 2011; 152:(3)632-642
Mehrvarzfar P, Abbott PV, Saghiri MA Effects of three oral analgesics on postoperative pain following root canal preparation: a controlled clinical trial. Int Endod J. 2012; 45:(1)76-82
Moore PA, Nahouraii HS, Zovko JG Dental therapeutic practice patterns in the US. II. Analgesics, corticosteroids, and antibiotics. Gen Dent. 2006; 54:(3)201-207
Mickel AK, Wright AP, Chogle S An analysis of current analgesic preferences for endodontic pain management. J Endodont. 2006; 32:(12)1146-1154
Marek MA, Lindsell CJ, Jauch EC Effect of education and guidelines for treatment of uncomplicated dental pain on patient and provider behavior. Ann Emerg Med. 2004; 44:323-329
Rothwell PS. Self-medication for dental pain. J Dent. 1970; 20
Preshaw PM, Meechan JG, Dodd MD. Self-medication for the control of dental pain: what are our patients taking?. Dent Update. 1994; 21:(7)299-304
Dodd MD, Graham CA. Unintentional overdose of analgesia secondary to acute dental pain. Br Dent J. 2002; 193:(4)211-212
Thomas MB, Moran N, Smart K Paracetamol overdose as a result of dental pain requiring medical treatment: two case reports. Br Dent J. 2007; 203:(1)25-28
Sivaloganathan K, Johnson PA, Bray GP Pericoronitis and accidental paracetamol overdose: a cautionary tale. Br Dent J. 1993; 174:(2)69-71
Mason C, Porter SR, Madland G Early management of dental pain in children and adolescents. J Dent. 1997; 25:(1)31-34
Manchikanti L. National drug control policy and prescription drug abuse: facts and fallacies. Pain Phys. 2007; 10:(3)399-424
Oakley M, O'Donnell J, Moore PA The rise in prescription drug abuse: raising awareness in the dental community. Compend Cont Educ Dent. 2011; 32:(6)14-16
Zechnich AD, Hedges JR. Community-wide emergency department visits by patients suspected of drug-seeking behavior. Acad Emerg Med. 1996; 3:312-317
Townsend JA, Ganzberg S, Thikkurissy S. The effect of local anesthetic on quality of recovery characteristics following dental rehabilitation under general anesthesia in children. Anesth Prog. 2009; 56:(4)115-122
Kaufman E, Epstein JB, Gorsky M Preemptive analgesia and local anesthesia as a supplement to general anesthesia: a review. Anesth Prog. 2005; 52:(1)29-38
Baygin O, Tuzuner T, Isik B Comparison of pre-emptive ibuprofen, paracetamol, and placebo administration in reducing post-operative pain in primary tooth extraction. Int J Paediatr Dent. 2011; 21:(4)306-313
O'Donnell A, Henderson M, Fearne J Management of post operative pain in children following extractions of primary teeth under general anaesthesia: a comparison of paracetamol, voltarol, and no analgesia. Int J Paediatr Dent. 2007; 17:(2)110-115
Bridgman JB, Gillgrass TG, Zacharis M. The absence of any pre-emptive analgesic effect for non-steroidal anti-inflammatory drugs. Br J Oral Maxillofac Surg. 1996; 34:(5)428-431
Chapman CR, Gehrig JD, Wilson ME. Acupuncture compared with 33 per cent nitrous oxide for dental analgesia: a sensory decision theory evaluation. Anesthesiology. 1975; 42:(5)532-537
Babl FE, Oakley E, Puspitadewi A Limited analgesic efficacy of nitrous oxide for painful procedures in children. Emerg Med J. 2008; 25:717-721
Ong CK, Seymour RA, Tan JM. Sedation with midazolam leads to reduced pain after dental surgery. Anesth Analg. 2004; 98:(5)1289-1293
Panzer O, Moitra V, Sladen RN. Pharmacology of sedative-analgesic agents: dexmedetomidine, remifentanil, ketamine, volatile anesthetics, and the role of peripheral Mu antagonists. Anesthesiol Clin. 2011; 29:(4)587-605
Nayyar MS, Yates C. Bupivocaine as pre-emptive analgesia in third molar surgery: randomised controlled trial. Br J Oral Maxillofac Surg. 2006; 44:(6)501-503
Cambell WI, Kendrick RW. Pre-emptive analgesia using local anaesthesia: a study in bilateral symmetrical surgery. Br J Anaesth. 1997; 79:(5)657-659
Sultan J, Curran AJ. Effect of warming local anaesthetics on pain of infiltration. Emerg Med J. 2007; 24:723-725
Quaba O, Huntley JS, Bahia H A users guide for reducing the pain of local anaesthetic administration. Emerg Med J. 2005; 22:188-189
Diplomate of the National Dental Board of Anaesthesiologists (USA), Professor of Anaesthesiology and Sedation at University of the Western Cape, and Programme Director of Postgraduate Certificate in Dental Sedation and Pain Management at University College London
Effective pain control is a basic requirement for patients undergoing dental treatment, particularly under conscious sedation as patients are usually nervous. In order to achieve adequate pain management, clinicians must have an understanding of the physiology of pain, the various pain control modalities and be aware of the evidence base relating to analgesia in dentistry. This article focuses on how to provide effective pain control using analgesic drugs for patients undergoing dental conscious sedation, whilst also considering other available pain control modalities.
Clinical Relevance: Dentists have a duty to provide, and patients have a right to expect, adequate and appropriate pain and anxiety control.
Article
The General Dental Council document Maintaining Standards. Guidance to Dentists on Professional and Personal Conduct1 emphasizes the importance of adequate pain and anxiety control by stating that dentists ‘have a duty to provide and patients have a right to expect adequate and appropriate pain and anxiety control’. This statement is fundamental to the provision of successful conscious sedation.
Conscious sedation has been defined as:
‘A technique in which the use of a drug or drugs produces a state of depression of the central nervous system enabling treatment to be carried out, but during which verbal contact with the patient is maintained throughout the period of sedation.’1
The drugs and techniques used should carry a margin of safety wide enough to render loss of consciousness unlikely, with protective reflexes maintained.
Two categories of sedation techniques exist; basic and advanced techniques.
Basic techniques involve the use of a single agent drug at a time, administered via a single route. This includes inhalational sedation using nitrous oxide with oxygen, intravenous sedation using titrated midazolam alone, or a benzodiazepine administered orally or transmucosally.
Basic techniques exclude sedation in children under 12 years, with the exception of nitrous oxide/oxygen inhalation sedation. Advanced techniques may involve the use of combinations of drugs, multiple drugs, infusion techniques or combined different routes of administration of the drugs used.2
The importance of pain control during sedation
There are significant advantages in achieving optimal pain control for patients undergoing conscious sedation for dentistry. These include:
Patient comfort;
Operator and patient safety;
Operator ease;
Avoidance of potential negative psychological impacts from pain;
Avoiding the potentiation of pain post-operatively.
As there are numerous important clinical requirements and documentation issues relating to conscious sedation, which may pre-occupy the dental sedationist, it is important that the fundamental obligation of providing appropriate pain control is not overlooked. In addition, patients who undergo sedation are usually anxious, their responses during sedation are depressed, and these are both possible hindrances to communicating any pain they experience effectively. Therefore, an active effort must be made to assess and appropriately manage pre-, intra-, and post-operative pain.
This article focuses on how to provide effective pain control using analgesic drugs for patients undergoing dental conscious sedation, whilst also considering other available pain control modalities.
The physiology of pain
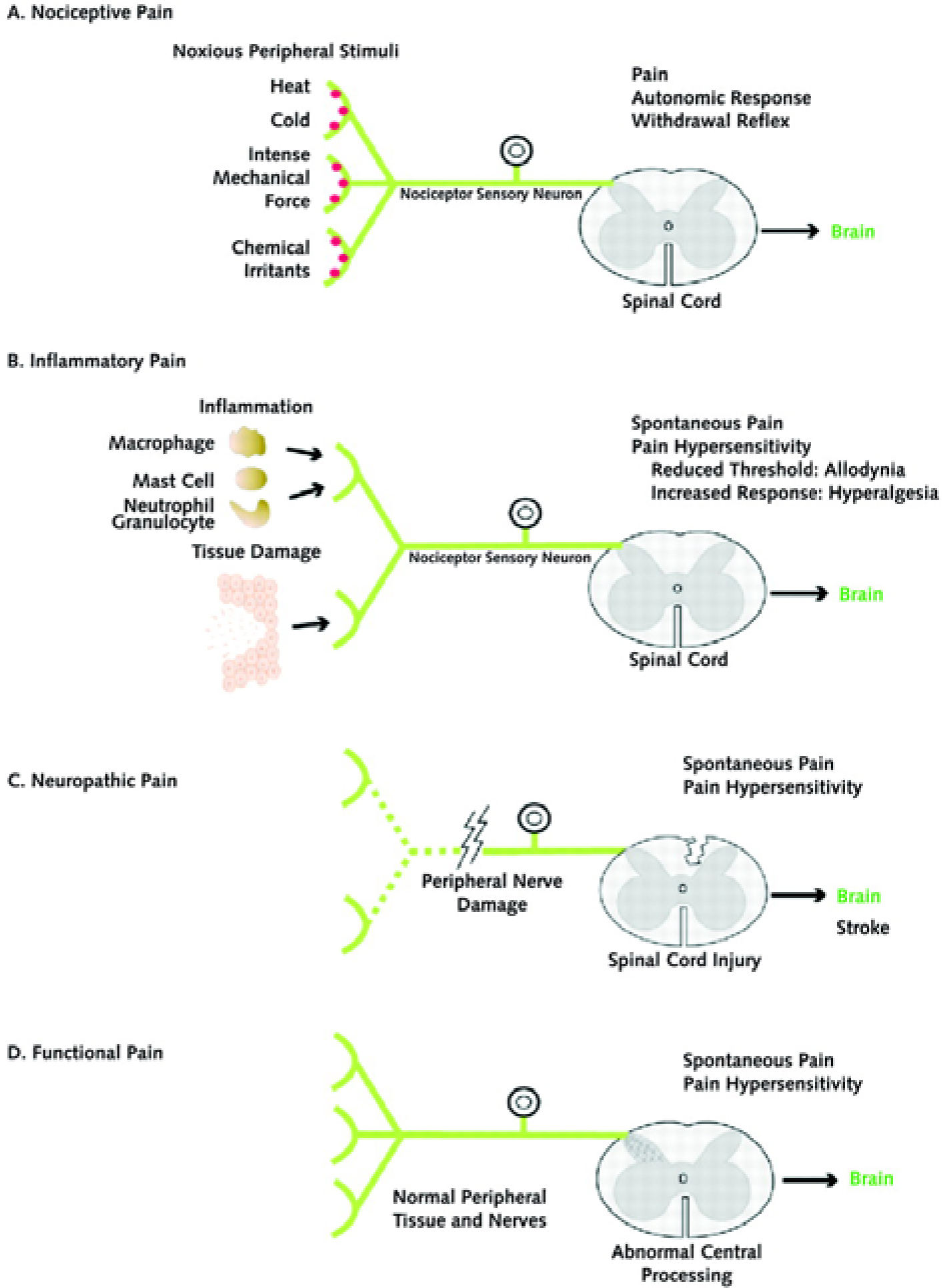
In order to understand various pain control modalities, a basic understanding of the physiology of pain is necessary. Pain is an unpleasant response to noxious stimuli; it serves an important protective purpose in identifying potentially harmful agents and discouraging exposure to them.3 Woolf describes four basic types of pain4 (Figure 1):
Nociceptive pain – transient pain in response to a noxious stimulus.
Inflammatory pain – spontaneous pain, with hypersensitivity to pain in response to tissue damage and inflammation.
Neuropathic pain – spontaneous pain, with hypersensitivity to pain in association with damage to, or a lesion of, the nervous system.
Functional pain – hypersensitivity to pain resulting from the abnormal central processing of a normal input.
Figure 1. Diagram demonstrating the mechanisms of pain. (With kind permission of Annals of Internal Medicine, Woolf.4
Nociceptive pain is the type of pain experienced during dental procedures, with inflammatory pain having a predominant role after the procedure is carried out. However, neuropathic pain may also result following neural trauma, such as in the case of inferior alveolar nerve damage, or in the case of ‘phantom tooth pain’ following pulp extirpation or extraction.5
Pain is a complex physiological process, with input from the higher centres of the brain, and comprises both sophisticated positive and negative feedback mechanisms.3 These numerous natural mechanisms that modulate pain present various opportunities to manipulate pain whilst undergoing dentistry.
Pain control techniques
The available methods of pain control include:
Psychological techniques;
Alternative techniques, such as hypnosis and acupuncture;
Analgesics;
Local anaesthetic agents;
The use of sedatives with analgesic properties.
This section focuses on the use of analgesics and briefly outlines the other pain control modalities.
Psychological techniques
Various psychological factors influence the perception of pain, including attentiveness, emotions, stress, empathy and the administration of a placebo. Thereby, it is possible to use techniques such as distraction and relaxation to improve mood and focus the patient's attention away from pain.6
Alternate methods
Hypnosis
Hypnosis is the interaction between one person and another, in an attempt to influence the subject's perceptions, feeling or thinking.7 Studies have reported that the use of hypnosis can reduce post-operative pain and analgesic consumption, as well as the amount of sedative required.8,8,9 It is recognized that individuals have a variable susceptibility to hypnotization10 and further studies are required to substantiate the wider application of hypnosis for dental pain control.
Acupuncture
Acupuncture involves the stimulation of anatomical locations on the skin by a variety of techniques. The most studied mechanism is by penetration of the skin by thin, solid, metallic needles, which are manipulated manually or by electrical stimulation.11
The National Institutes of Health (NIH), a part of the US Department of Health and Human Services, evaluated the literature on the use of acupuncture for a variety of conditions and promising results were reported in the case of post-operative dental pain.11 Some studies have shown acupuncture improves post-operative pain relief,12,13,14 however, there have been conflicting findings.15 The limited numbers of studies have included small sample sizes and well designed studies of sufficient power are required to derive meaningful conclusions.
Analgesics
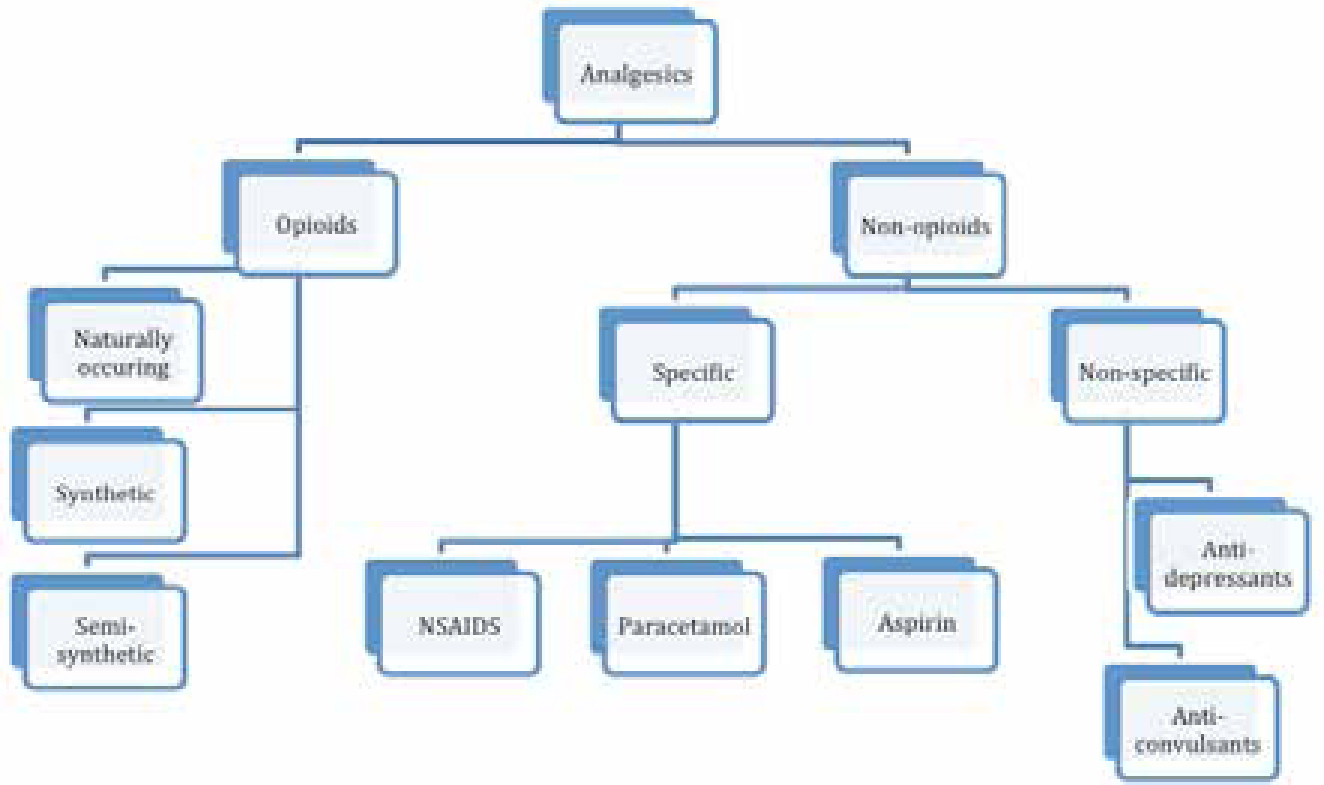
Various types of analgesics exist (Figure 2), which fall into two broad groups:
Opioids; and
Non-opioids.
Figure 2. A broad classification of analgesic types.
Opioids
Opioid analgesics act on centrally located opiate receptors resulting in an inhibition of pain.16 They do, however, have a number of untoward effects when used systemically, including nausea, vomiting, constipation, dry mouth, hypotension, respiratory depression, mood change and dependence.17 Opioids also potentiate the effect of sedatives and increase the likelihood of respiratory depression, so should be used cautiously in patients undergoing conscious sedation. Their application as locally acting agents for dental pain has also been investigated, which may have an increasing role in the future.18
Non-opioids
There are two main types of non-opioid analgesic:
Specific; and
Non-specific.
Specific analgesics include non-steriodal anti-inflammatory drugs (NSAIDs), paracetamol and aspirin; these are the most commonly used analgesics in acute dental pain and will be discussed further.
The non-specific analgesic drugs have other primary indications but also have analgesic properties, such as the anti-convulsants and anti-depressants; their use in dentistry is largely in the case of chronic pain conditions.
There may be a number of mechanisms by which NSAIDs work. A major hypothesis is that they produce analgesic and anti-inflammatory actions by the inhibition of cyclo-oxygenase, reducing the synthesis of arachidonic acid metabolites, such as prostaglandins and thromboxanes, which are pain mediators. However, other actions affecting signalling pathways that mediate inflammatory responses have also been suggested.19
The exact mode of action of paracetamol is unclear, but it is known to have analgesic and anti-pyretic effects. It is also a weak inhibitor of cyclo-oxygenase and inhibits prostaglandin synthesis in the CNS but not in the peripheral tissues, so there is very little, if any, anti-inflammatory action.19
Choice of analgesic for dental pain
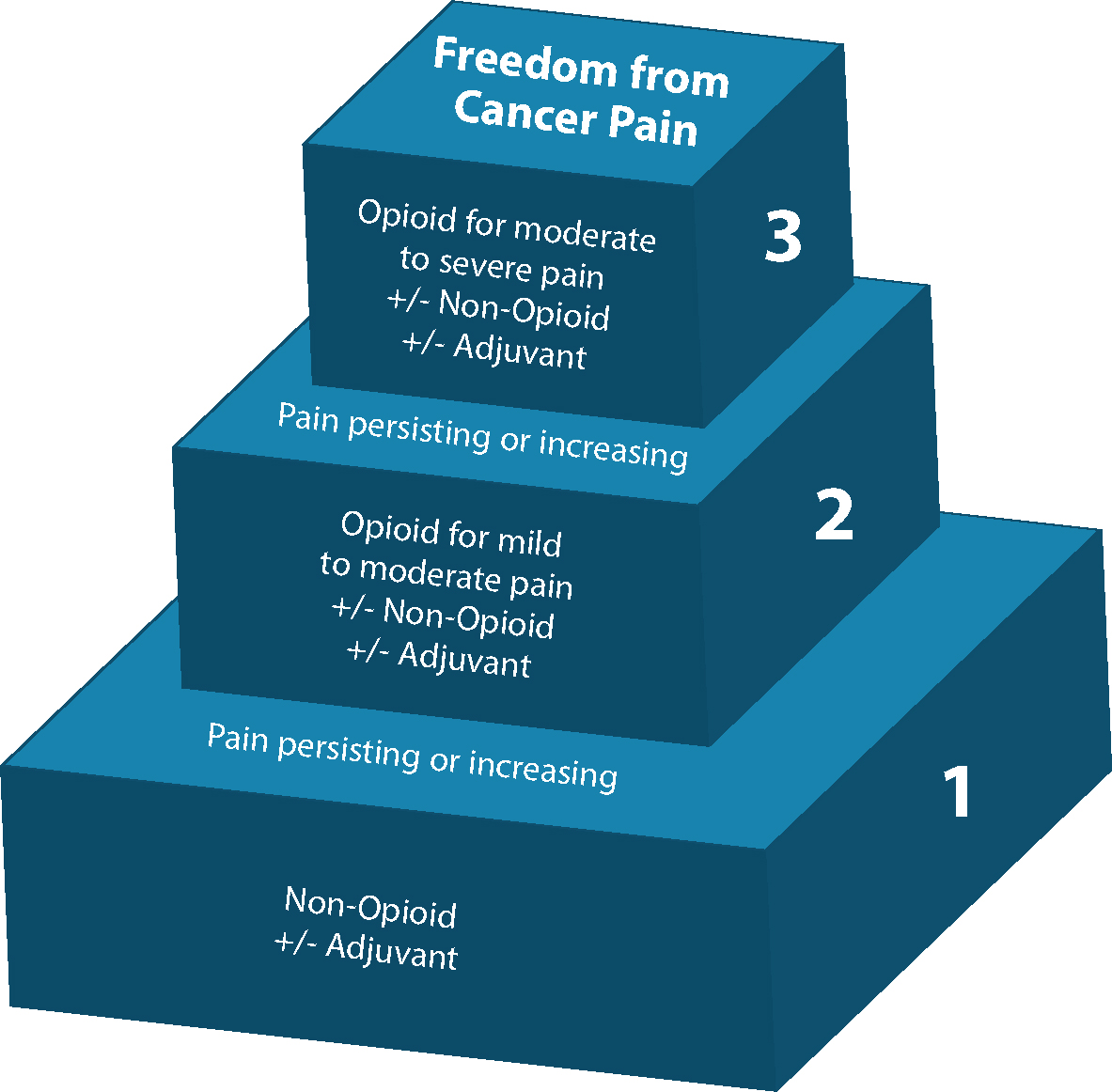
The World Health Organization developed a ‘three step’ plan for pain management,20 based on cancer pain, which can serve as a useful model for the selection of appropriate analgesics. To summarize:
Step 1: mild pain is managed by simple non-opioid analgesics such as paracetamol and NSAIDs;
Step 2: moderate pain is managed by weak opioids such as tramadol or codeine phosphate;
Step 3: severe pain is managed by strong opioids such as morphine (Figure 3). Although this may be extrapolated to other forms of non-cancer pain, it is not strictly applicable to dental pain given the relevant evidence base.19, 21
Figure 3. The WHO pain relief ladder.20
In the case of dental pain that cannot be controlled by over-the-counter medication, the prescribing of analgesics can be challenging. Various studies have explored analgesic potency in dental pain, predominantly following the extraction of bilateral lower third molars, which allows individuals to serve as their own controls.
Systematic reviews have examined the use of single drugs, combination analgesics, and have also compared the effectiveness of different analgesic drugs. It has been shown that paracetamol is a safe and effective drug to use following third molar extractions,22 and combining paracetamol with codeine increases the duration of analgesia.23 A review and meta-analysis on the efficacy of non-opioid analgesics for dental pain revealed that therapeutic doses of NSAIDs were significantly more efficacious than the combination of paracetamol and codeine.24
An overview of 35 Cochrane reviews examining analgesic efficacy in acute post-operative pain revealed that, in dental pain, 400 mg ibuprofen was better than 1000 mg paracetamol and 1000 mg aspirin.25 This review highlighted the fact that the use of analgesics in dental pain had been widely investigated, as such studies formed the majority of those included. It had also been found that dihydrocodeine is significantly inferior to ibuprofen for moderate to severe post-operative pain.26
The combined use of ibuprofen and paracetamol is often advocated, but there have been few studies assessing their combined use until recently. A recent trial has found concurrent ibuprofen and paracetamol provides significantly better analgesic efficacy compared with ibuprofen or paracetamol alone, for acute post-operative dental pain.27 Daniels and co-workers28 conducted a double-blind randomized placebo-controlled study comparing the efficacy and tolerability of the following drug combinations: ibuprofen and paracetamol, ibuprofen and codeine, and paracetamol and codeine. Results demonstrated that the ibuprofen and paracetamol combination was significantly more efficacious than the paracetamol and codeine combination, and was comparable to the ibuprofen and codeine combination. Adverse events were uncommon and were significantly less frequent in the groups taking the ibuprofen and paracetamol combination compared to the codeine combinations.
In an alternative dental pain model, a study compared a combination of paracetamol and ibuprofen to tramadol or naproxen, for post-operative pain following the instrumentation of root canals. Tramadol was found to be significantly less effective than naproxen and the paracetamol-ibuprofen combination, the latter two being similar.29
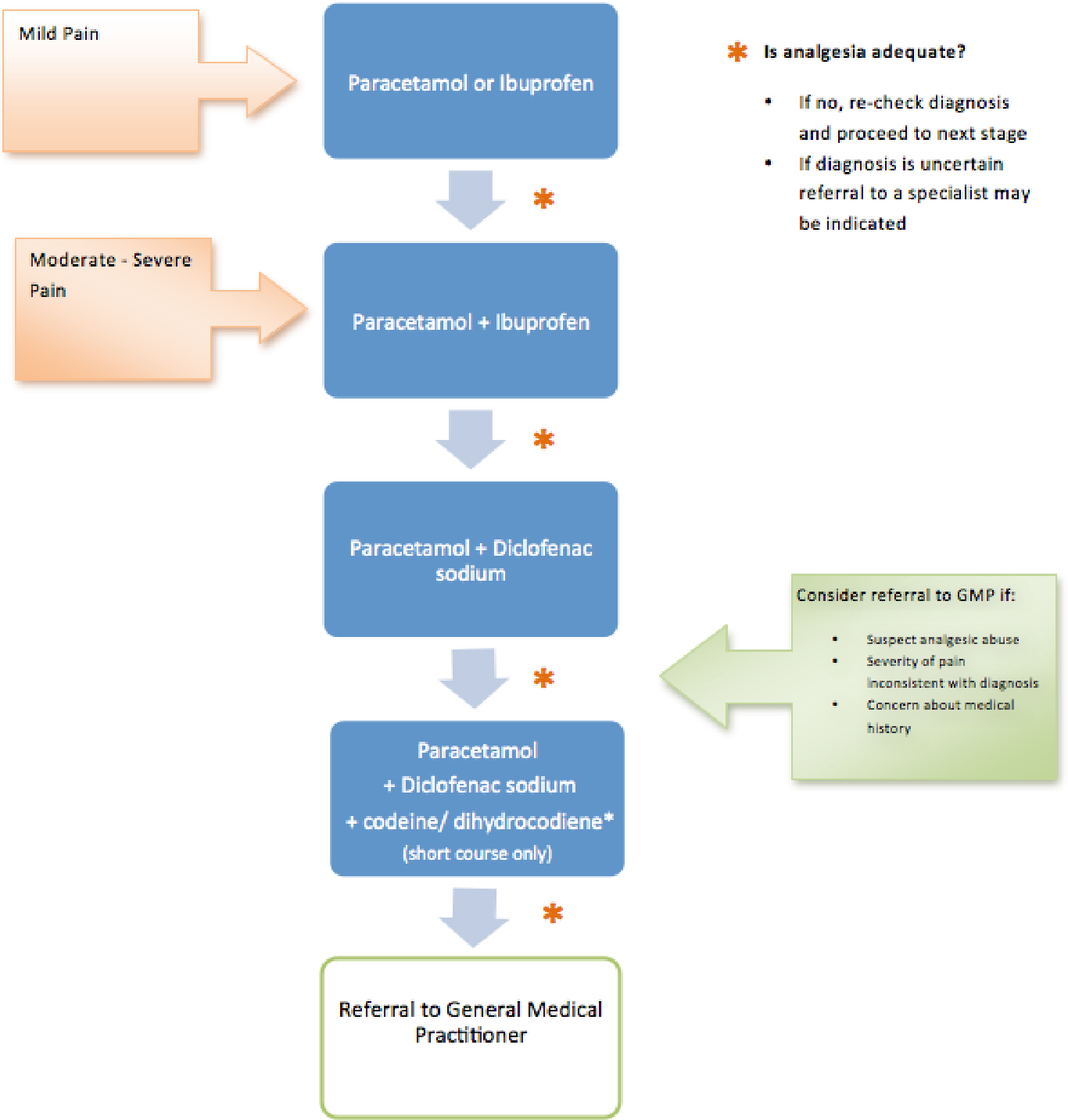
From the available evidence base, it appears that, in the case of acute dental pain, NSAIDs such as ibuprofen offer superior pain relief compared to other analgesics and should be the first choice, unless there are specific contra-indications, in which case paracetamol should be advised. When pain relief with a single agent is insufficient, or in the case of moderate-severe pain, a combination of a NSAID, such as ibuprofen, and paracetamol should be used (Figure 4). Paracetamol is also available as an intravenous formulation for patients undergoing sedation. If pain relief is still not optimal, an alternative NSAID could be considered. Only in the case of severe pain, not amenable to control with these agents alone, may weak opioids, such as tramadol, codeine or dihydrocodeine, supplement analgesia. As these opioids have been shown to be less effective than paracetamol and ibuprofen, in the case of dental pain, there seems little point in their use as single agents. They may, however, be useful in combination therapy. It is likely that this pathway would control most dental pain, but if there is persistent pain, despite these measures, high priority should be given to re-assessing the cause of pain and managing it appropriately, for example pulp extirpation or extraction if irreversible pulpitis is present. In any case, prompt treatment of the cause of pain is preferable to prolonged symptomatic control. In cases of uncontrollable dental pain, the use of a long-acting local anaesthetic may occasionally be necessary.
Figure 4. A suggested model of analgesia for dental pain.
The Dental Practitioners Formulary (DPF), as part of the British National Formulary (BNF),17 contains aspirin, diclofenac sodium, dihydrocodeine, ibuprofen and paracetamol, which should be adequate to control most dental pain. In the UK, these drugs are also readily available over the counter, with the exception of dihydrocodeine. Whilst dentists may prescribe other analgesic drugs not listed in the DPF using a private prescription, they should be aware of the limitations of these drugs in relation to their personal training and experience.
Studies on analgesic prescriptions from dentists reveal a similar pattern to that recommended above, with ibuprofen being most frequently prescribed and non-narcotics being preferred.30,31 In the emergency department hospital setting, putting into effect guidance has been shown to reduce the inappropriate prescribing of opiates,32 and having clear national guidance for the prescribing of analgesics in the dental setting has the potential to improve prescribing practices.
Patients' choices of analgesics for dental pain seem to have changed over the years, with paracetamol replacing aspirin as being the most commonly used agent.33,34 The importance of appropriate advice regarding analgesia cannot be under-estimated, as some patients self medicate inappropriately or overdose following dental pain.35,36,37,38 The possibility of prescription drug abuse is a further reason to discourage inappropriate prescribing, which is becoming an increasing problem. With regard to analgesics, the most commonly abused drugs are opiates and opioids, with a significant proportion being obtained through prescriptions.39 At risk groups include adolescents, young adults and seniors over 65 years of age.40 Dentists should be aware of drug-seeking behaviours, such as reporting pain that is inconsistent with clinical findings, shopping around for prescriptions from different practitioners, or reporting an allergy to all other commonly used analgesics.39,41
Pre-emptive analgesia
Studies have suggested that the pre-operative peripheral blocking of painful stimuli, by analgesics or local anaesthetics, can reduce the severity of post-operative pain.42,43
Different pre-operative analgesic agents have been compared to a placebo in order to assess effects on post-operative pain in children who were having primary molars extracted. Both paracetamol, and more so ibuprofen, reduced post-operative pain at 15 minutes and 4 hours.44 An earlier study on children undergoing extractions compared the pre-operative use of paracetamol, voltarol and no analgesia; they found children experienced less pain when rectal voltarol was provided compared to paracetamol or no analgesia, and patients that received no analgesics experienced the most pain.45
Conversely, a double-blind, randomized, cross-over trial on a small sample of 21 patients failed to show any difference in post-operative pain when they compared patients receiving a pre-operative or post-operative 100 mg dose of diclofenac sodium.46 Further well designed studies of sufficient power are required to assess the benefits of pre-emptive analgesia in dental pain models.
Analgesic properties of various sedatives
There is a variation in the analgesic properties of the different sedative drugs used, and the benefits of sedative drugs with analgesic properties can be conferred to patients as part of the provision of effective pain relief.
Nitrous oxide sedation has been shown to reduce tooth pulp responsiveness,47 however, its efficacy as an analgesic used alone in very painful procedures is limited.48
Intra-venous sedation with midazolam itself has been shown to result in lowered post-operative pain intensity scores, and reduced analgesic consumption.49
Other agents used as sedatives have strong analgesic properties, these include opioids, such as fentanyl and remifentanil, and the dissociative drug ketamine.50 However, these drugs are advanced techniques and should only be used by appropriately trained sedationists.
Local anaesthesia
Achieving adequate pain control during dental conscious sedation relies upon effective local anaesthesia. Although the use of local anaesthesia during conscious sedation for potentially painful dental procedures is standard practice, there is little in the literature exploring its importance. Local anaesthesia has been shown to provide pre-emptive analgesia and significantly reduce post-operative pain following the extraction of third molars,51 however, there have been conflicting findings.52
Care should be taken to limit pain on injection as part of the overall pain control plan. This can be achieved by reassurance and distraction, warming local anaesthetics, using a buffered anaesthetic solution, prior to application of topical anaesthetic, use of a fine gauge needle, injecting slowly, using small amounts of anaesthetic, and using blocks where necessary.53,54
Summary
The prevention of pain, and effective pain control, are fundamental components of a dentist's duty of care to a patient. This is particularly important for patients undergoing conscious sedation who are likely to be anxious from the outset. Conscious sedation should not be considered as an alternative to providing effective pain control during dentistry, but part of the total package of effective pain and anxiety management. In order to achieve effective pain control for patients undergoing dental conscious sedation, an understanding of the basic physiology of pain and different pain control modalities is essential. Patients should be prescribed, or given, appropriate advice on suitable analgesics for dental pain control, including pre-emptive analgesia, when indicated. This necessitates an awareness of the evidence base pertaining to the use of analgesics in dentistry, which shows that NSAIDs, such as ibuprofen, are the analgesics of choice for dental pain. They can be substituted or supplemented with paracetamol when there are contra-indications to NSAIDs, or when their use in isolation is insufficient. Weak opioids may be considered in combination with these drugs if complete pain control is not achieved, and stronger opioids may be considered, if necessary, but should be prescribed by an appropriately trained practitioner. The use of various other methods to control pain should be employed, where appropriate, to include psychological methods, effective local anaesthesia for painful dental procedures and, when suitable, the use of sedative drugs with analgesic properties. Hypnosis and acupuncture have been reported to reduce dental pain, however, the evidence is limited and high quality randomized controlled trials on their effectiveness are required.