Anneroth G, Sigurdson A. Hyperplastic lesions of the gingiva and alveolar mucosa. A study of 175 cases. Acta Odontol Scand. 1983; 41:75-86
Hirshberg A, Shnaiderman-Shapiro A, Kaplan I, Berger R. Metastatic tumours to the oral cavity – pathogenesis and analysis of 673 cases. Oral Oncol. 2008; 44:743-752
Daley TD, Wysocki GP, Wysocki PD, Wysocki DM. The major epulides: clinicopathological correlations. J Can Dent Assoc. 1990; 56:627-630
Cawson RA, Odell EW. Cawson's Essentials of Oral Pathology and Oral Medicine, 8th edn. Edinburgh: Churchill Livingstone; 2008
Soames JV, Southam JC., 4th edn. New York: Oxford University Press; 2006
Meleti M, Corcione L, Sesenna E, Vescovi P. Unusual presentation of primary squamous cell carcinoma involving the interdental papilla in a young woman. Br J Oral Maxillofac Surg. 2007; 45:420-422
Scipio JE, Murti PR, Al-Bayaty HF, Matthews R, Scully C. Metastasis of breast carcinoma to mandibular gingiva. Oral Oncol. 2001; 37:393-396
Jaguar GC, Prado JD, Soares F, Alves FA, Osório CAT. Gingival metastasis from non-small cell undifferentiated carcinoma of the lung mimicking a pyogenic granuloma. Oral Oncol Extra. 2006; 42:36-39
Suzuki T, Kumamoto H, Nagasaka H, Kawamura H, Ooya K. Intramucosal naevus with pseudoepitheliomatous hyperplasia in the gingiva: a case report. Int J Oral Maxillofac Surg. 2002; 31:331-334
De Vicente JC, Martín M, López-Arranz JS. Asymptomatic epulis of the maxilla. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 91:135-138
Zhang W, Chen Y, An Z, Geng N, Bao D. Reactive gingival lesions: a retrospective study of 2,439 cases. Quintessence Int. 2007; 38:(2)103-110
Lawoyin JO, Arotiba JT, Dosumu OO. Oral pyogenic granuloma: a review of 38 cases from Ibadan, Nigeria. Br J Oral Maxillofac Surg. 1997; 35:185-189
Al-Khateeb T, Ababneb K. Oral pyogenic granuloma in Jordanians: a retrospective analysis of 108 cases. J Oral Maxillofac Surg. 2003; 61:1285-1288
Katsikeris N, Kakarantza-Angelopoulou E, Angelopoulos AP. Peripheral giant cell granuloma. Clinicopathologic study of 224 new cases and review of 956 reported cases. Int J Oral Maxillofac Surg. 1988; 17:94-99
Burkes EJ, White RP. A peripheral giant-cell granuloma manifestation of primary hyperparathyroidism: report of a case. J Am Dent Assoc. 1989; 118:62-64
Papageorge MB, Doku HC. An exaggerated response of intra-oral pyogenic granuloma during puberty. J Clin Pediatr Dent. 1992; 16:213-216
Daley TD, Nartey NO, Wisocki GP. Pregnancy tumour: an analysis. Oral Surg Oral Med Oral Pathol. 1991; 72:196-199
Cloutier M, Charles M, Carmichael RP, Sándor GKB. An analysis of peripheral giant cell granuloma associated with dental implants. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2007; 103:(5)618-622
Yadav R, Gulati A. Peripheral ossifying fibroma: a case report. J Oral Sci. 2009; 51:(1)151-154
Coelho CM, Zucoloto S, Lopes RA. Denture induced fibrous inflammatory hyperplasia: a retrospective study in a school of dentistry. Int J Prosthodont. 2000; 13:148-151
Wood NK, Goaz PW., 5th edn. New Delhi: Elsevier; 2007
Meng HK. Periodontal abscess. Annals Periodontol. 1999; 4:79-82
Yamalik K, Bozkaya S. The predictivity of mandibular third molar position as a risk indicator for pericoronitis. Clin Oral Invest. 2008; 12:9-14
Manor Y, Mardinger O, Katz J, Taicher S, Hirshberg A. Peripheral odontogenic tumours – differential diagnosis in gingival lesions. Int J Oral Maxillofac Surg. 2004; 33:268-273
Buchner A, Merrell PW, Carpenter WM. Relative frequency of peripheral odontogenic tumors: a study of 45 cases and comparison with studies from the literature. J Oral Pathol Med. 2006; 35:385-391
Ide F, Mishima K, Satio I, Kusama K. Rare peripheral odontogenic tumours: report of 5 cases and comprehensive review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2008; 106:e22-e28
Aldred MJ, Talacko AA, Ruljancich K Oral focal mucinosis: report of 15 cases and review of the literature. Pathology. 2003; 35:(5)393-396
Gabay E, Akrish S, Machtei EE. Oral focal mucinosis associated with cervical external root resorption: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2010; 110:e75-e78
Polonowita AD, Firth NA, Rich AM. Verruciform xanthoma and concomitant lichen planus of the oral mucosa. A report of three cases. Int J Oral Maxillofac Surg. 1999; 28:62-66
Philipsen HP, Reichart PA, Takata T, Ogawa I. Verruciform xanthoma-biological profile of 282 oral lesions based on a literature survey with nine new cases from Japan. Oral Oncol. 2003; 39:325-336
Sist TC, Greene GW. Traumatic neuroma of the oral cavity. Report of thirty-one new cases and review of the literature. Oral Surg Oral Med Oral Pathol. 1981; 51:394-402
Barasch A, Gofa A, Krutchkoff DJ, Eisenberg E. Squamous cell carcinoma of the gingiva. A case series analysis. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1995; 80:183-187
Alsharif MJ, Jiang WA, He S, Zhao Y, Shan Z, Chen X. Gingival squamous cell carcinoma in young patients: report of a case and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107:696-700
Gomez D, Faucher A, Picot V Outcome of squamous cell carcinoma of the gingiva: a follow-up study of 83 cases. J Craniomaxillofac Surg. 2000; 28:331-335
Walvekar RR, Chaukar DC, Deshpande MS Verrucous carcinoma of the oral cavity: a clinical and pathological study of 101 cases. Oral Oncol. 2009; 45:47-51
Tanaka N, Mimura M, Ogi K, Amagasa T. Primary malignant melanoma of the oral cavity: assessment of outcome from the clinical records of 35 patients. Int J Oral Maxillofac Surg. 2004; 33:761-765
Meleti M, Leemans CR, Mooi WJ, Vescovi P, van der Waal I. Oral malignant melanoma: a review of the literature. Oral Oncol. 2007; 43:116-121
Barker BF, Carpenter WM, Daniels TE Oral mucosal melanomas: The WESTOP Banff Workshop Proceedings. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 1997; 83:672-679
Laskaris G. Oral manifestations of HIV disease. Clin Dermatol. 2000; 18:447-455
Epstein JB, Epstein JD, Le ND, Gorsky M. Characteristics of oral and paraoral malignant lymphoma: a population based review of 361 cases. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2001; 92:519-525
Angiero F, Stefani M, Crippa R. Primary non-Hodgkin's lymphoma of the mandibular gingiva with maxillary gingival recurrence. Oral Oncol Extra. 2006; 42:123-128
Ramirez JR, Seoane J, Montero J, Cerero R. Isolated gingival metastasis from hepatocellular carcinoma mimicking a pyogenic granuloma. J Clin Periodontol. 2003; 30:926-929
Nxumalo TN, Shear M. Gingival cyst in adults. J Oral Pathol Med. 1992; 21:(7)309-313
Shear M, Speight PM., 4th edn. Oxford: Blackwell Mungskaard; 2007
Dayan D, Buchner A, Gorsky M, Harel-Raviv M. The peripheral odontogenic keratocyst. Int J Oral Maxillofac Surg. 1988; 17:81-83
Koudstaal MJ, van der Wal KGH, Lam KH, Meeuwis CA, Speleman L, Levin MD. Granulocytic sarcoma (chloroma) of the oral cavity: report of a case and literature review. Oral Oncol Extra. 2006; 42:70-77
Lynch DP, Conlon TO, Maxwell GR, Martinez F. Exophytic gingival mass in a geriatric patient. Oral Surg Oral Med Oral Pathol. 1998; 85:5-7
Ponniah I, Shaheen A, Shankar KA, Kumaran MG. Wegener's granulomatosis: the current understanding. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:265-270
Stewart C, Cohen D, Bhattacharyya I Oral manifestations of Wegener's granulomatosis: a report of three cases and a literature review. J Am Dent Assoc. 2007; 138:338-348
Fatahzadeh M. Inflammatory bowel disease. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 108:e1-e10
Buchner A, Merrel PW, Carpenter WM. Relative frequency of solitary melanocytic lesions of the oral mucosa. J Oral Pathol Med. 2004; 33:(4)550-557
Jainkittivong A, Langlais RP. Buccal and palatal exostoses: prevalence and concurrence with tori. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90:48-53
Localized gingival overgrowths (LGOs) encompass a category of oral lesions that are commonly encountered in dental practice. The authors report three cases of gingival epulides and also review the various conditions (both local and systemic) in which LGOs have been reported to occur. A flowchart is also proposed for a systematic approach to aid diagnosis. Although most epulides are hyperplastic lesions, rare conditions clinically identical to inflammatory or reactive LGOs do occur. Their innocuous appearance may frequently deceive the dental practitioner.
Clinical Relevance: Knowledge of various lesions that could present as an LGO is necessary and significant, as prompt diagnosis and specialist referral influences the treatment plan.
Article
Localized gingival overgrowth (LGO)
Occurrence of a LGO can indicate many conditions, both local and systemic, ranging from regular hyperplastic reactive lesions1 to atypical metastatic neoplasms.2 A non-specific term ‘epulis’ (literally, ‘on the gingiva’) is commonly used to describe any such circumscribed overgrowths on the gingiva. However, as this description refers only to the site and does not provide any indication about the nature of the lesion, a clinical diagnosis of ‘epulis’ must be replaced with a more definitive diagnosis after biopsy and histopathologic evaluation.3,4,5,6
A review of the literature shows that many rare lesions have manifested as asymptomatic epulides. Meleti et al6 reported a case of primary squamous cell carcinoma on the gingiva that clinically mimicked a fibrous epulis. Cases of metastases from breast7 and lung carcinoma,8 bearing clinical resemblance to a gingival pyogenic granuloma, have also been published. Intramucosal nevi and oral melanoma presenting as circumscribed soft tissue masses on the gingiva were reported by Suzuki et al9 and De Vicente et al,10 respectively. Thus, in practice, the final diagnosis of an epulis may range from benign to potentially lethal lesions, although most epulides are fibrous reactive lesions.4
Case reports
Case 1
A 23-year-old female presented to the AIMST Dental Institute with an asymptomatic, pale-pink, firm, sessile mass arising from the maxillary labial gingiva of tooth UL2 (Figure 1). Clinically, the lesion measured 1 x 0.6 x 0.4 cm approximately, with no surface ulceration or signs of inflammation. The mass had been present for two years, with the patient's only complaint being its unaesthetic appearance. Her medical history was non-contributory. The patient could not relate any traumatic event to the area and, except for plaque accumulation on the surface of teeth, there was no evidence of other local irritating factors. A periapical radiograph revealed no obvious pathology, ruling out a central lesion. Based on the clinical findings, a provisional diagnosis of fibrous epulis was made. However, other benign neoplasms were also considered in the differential diagnosis. The lesion was excised from the underlying mucosa, preserving the gingival architecture and contour (Figure 2). The final diagnosis after histopathological evaluation was irritational fibroma. Hence, a wider excision of the area was not indicated and the patient remained free of recurrence during a follow-up period of more than 6 months (Figure 3).
Figure 1. Asymptomatic, non-ulcerated exophytic growth.Figure 2. Gingival form and architecture preserved after excision.Figure 3. Six months following surgical removal.
Case 2
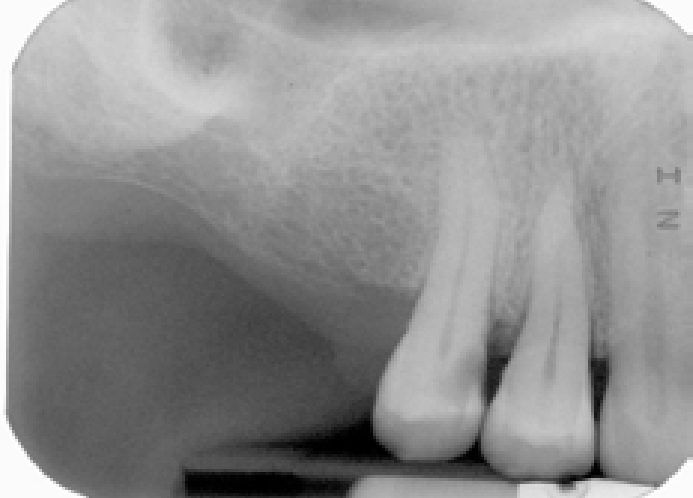
A 53-year-old female was referred for evaluation of a reddish pink growth on the maxillary right posterior buccal gingiva. The mass measured about 0.7 x 0.5 x 0.5 cm, was soft in consistency and showed no evidence of surface ulceration (Figure 4). Her medical and family histories were non-contributory. A periapical radiograph of the region revealed superficial erosion of the alveolar crest and loss of cortication on the distal aspect of tooth UR5 (Figure 5). The differential diagnosis included pyogenic granuloma and peripheral giant cell granuloma. A final pathologic diagnosis after excisional biopsy was peripheral giant cell granuloma.
Figure 4. Reddish pink growth on the distobuccal aspect of UR5.Figure 5. Periapical radiograph showing superficial erosion.
Case 3
A 49-year-old male was referred for evaluation of a pale pink mass on the mandibular right posterior buccal gingiva. The lesion measured approximately 1.5 x 1 x 0.6 cm, and was bony-hard in consistency (Figure 6). The clinical impression from the referring clinician was a bony overgrowth. The mass was excised as a requisite for pre-prosthetic preparation and submitted for histopathologic evaluation. The lesion was diagnosed as a fibro-epithelial polyp with dystrophic calcification.
Figure 6. Pink bony hard growth on the buccal aspect of LR6.
Differential diagnosis
Our literature survey showed that a variety of lesions (Table 1) caused focal masses on the gingiva. As seen from this table, a wide range of origin may be expected for LGOs, which may necessitate the inclusion of several lesions in the differential diagnosis.
All hyperplastic lesions are reactive or inflammatory in nature and represent an exuberant tissue response to persistent irritation or trauma.5 They are the most common oral exophytic lesions, described with distinct clinical terms based on the anatomical site of involvement, clinical features, or microscopic picture.11 Different entities of reactive hyperplasias arise from the gingival connective tissue response to varied intensities or sources of irritation. Hence, such a cause should be investigated by the practitioner during routine clinical examination.
Fibrous epulis is by far the most frequently reported reactive lesion on the gingiva, which usually presents with features as described in Case 1. These lesions represent a reactive fibrous hyperplasia (irritational/traumatic fibroma) or a fibro-epithelial hyperplasia (fibro-epithelial polyp) of the gingiva.12,13,14,15
Certain studies have reported pyogenic granuloma as the most common reactive lesion on the gingiva. This vascular lesion is usually painless and appears as a small, red, exophytic mass with a tendency to bleed easily.16,17 Some cases may show surface ulceration and can exhibit rapid growth that simulates malignancy, while long-standing lesions appear pink due to secondary fibrosis.13
A peripheral giant cell epulis clinically resembles the gingival pyogenic granuloma,11,13 as reported in Case 2. They are unique to the gingival mucosa with a tendency to resorb the underlying alveolar bone.18
Concentrations of circulating hormones also have an important role in the development of some of these lesions. Cases of peripheral giant cell epulides associated with hyperparathyroidism and reactive lesions occurring during puberty have been reported in the past. Frequently, pyogenic granulomas can develop in the second or third trimesters of pregnancy and ‘pregnancy tumour’ is a term often used to describe this lesion. Elevated female sex hormones during pregnancy cause the gingival tissues to respond in an exaggerated manner to local factors, resulting in this lesion, which often regresses after parturition.14,19,20,21
Recently, the occurrence of pyogenic granuloma and giant cell epulis have been related to dental implants.22
This category of reactive lesions also includes the peripheral ossifying fibroma, which occurs more often in the maxillary anterior gingivae. Clinically, it appears as a pink or red, exophytic lesion, usually less than 2 cm in diameter. Further, most studies have reported female predilection and peak incidences in the first and second decades of life.12,13,23
Epulis fissuratum or denture-induced hyperplasia is a reactive lesion associated with ill-fitting dentures. Arising usually in the vestibule, or sometimes beneath the denture base, they are asymptomatic overgrowths, varying from pink and firm to erythematous and oedematous with occasional ulceration.24
Inflammatory lesions
Abscesses related to teeth (both periodontal and periapical) can appear as ovoid elevations on the gingiva, along the lateral aspect of tooth roots. Pain, sensitivity to percussion, tooth elevation in the socket, increased mobility and suppuration are common findings in such cases. On occasions, in periapical abscesses, pus may accumulate beneath the mucosa where a ‘gum boil’ forms before a sinus develops. Further, a nodule of granulation tissue (parulis) often arises at the sinus opening in response to mucosal irritation by pus.25
In a previously healthy site, a gingival abscess can manifest as an acute suppurative swelling following impaction of a foreign body (food substance, toothbrush, toothpick, etc) into the gingiva.26 Inflammatory, oedematous focal gingival enlargement may occur as a result of localized gingivitis and pericoronitis.27,28
Peripheral odontogenic tumours
Peripheral odontogenic tumours are uncommon benign focal overgrowths of the oral soft tissue, occurring in the gingiva and overlying jaw mucosa. These peripheral tumours demonstrate histologic characteristics of their intra-osseous counterpart and many times are initially diagnosed clinically as reactive or inflammatory lesions. In a review of publications in English from 1987 to 1999, Manor et al29 found 129 reported cases of peripheral odontogenic tumours, with peripheral odontogenic fibroma as the most frequently described entity, followed by the other odontogenic tumours listed in Table 1. Further evidence from recent studies also demonstrated similar frequencies in the occurrence of these tumours.30,31
Benign tumours
The majority of the soft tissue tumours occurring in other sites of the body can present in the oral mucosa as well. Tumours on the gingiva can be clinically indistinguishable from focal fibrous hyperplasias.14 Common connective tissue tumours, like true fibromas, cannot reliably be distinguished from reactive lesions.5
An uncommon tumour, oral focal mucinosis, has been reviewed by Aldred et al.32 Their study showed that this tumour occurred most commonly on the gingiva, and often presented clinically as an innocuous soft tissue swelling. Gabay et al33 reported one case on the gingiva causing adjacent cervical root resorption.
Another rare tumour causing a verrucous or papillary excrescence predominantly on the gingiva and alveolar ridge is verruciform xanthoma. This lesion represents an unusual reaction to localized epithelial trauma or degeneration. Cases of verruciform xanthoma have been associated with lichen planus, lupus erythematosus, pemphigus vulgaris, leukoplakia and carcinoma in situ.34,35
Sometimes, traumatic neuromas can occur in the oral cavity following nerve injury, more often in the region of the metal nerve. A small nodule near the mental foramen, which causes considerable pain on pressure, is typical of a traumatic neuroma arising from a severed mental nerve. They arise as a disorganized mass, from proliferation of the proximal end of a severed nerve in an attempt to re-establish innervation with the distal segment.13,36,37
Malignant tumours
As a group, primary gingival malignancies are rare; the overall incidence of gingival carcinoma is less than 10% of all carcinomas arising on the oral mucosa, although it has been increasingly reported at this site in the past few years.38 The most frequently reported neoplasm on the gingiva is squamous cell carcinoma; however, cases of primary gingival verrucous carcinomas and rare malignant mesenchymal lesions on gingiva have also been published. The aetiology for malignancies in general is considered to be multifactorial, however, it has been estimated that smoking and alcohol consumption account for 75% of all cases of oral cancer. Carcinomas on the gingiva in particular may present with benign features and sometimes similarity to reactive lesions or periodontal disease may lead to delays in diagnosis or even to misdiagnosis, thereby posing problems in management.39,40 The proximity of underlying periosteum and alveolar bone usually invites early invasion, thereby resulting in radiographic evidence of bone involvement. Superficial erosion may arise apparently as a pressure phenomenon.40,41
Verrucous carcinomas, with a characteristic white warty appearance, may involve the gingiva and alveolar ridge. Seen commonly in elderly men, particularly associated with the habit of tobacco chewing, this tumour is described to be slow growing, locally aggressive with a low propensity for regional or distant metastasis.42
A potentially aggressive tumour of melanocytic origin is the malignant melanoma. Primary oral melanomas account for fewer than 1% of all melanomas. This neoplasm is more common in Japan and Africa than in Western countries; occurring more often in older adults with a predilection for the hard palate and maxillary alveolar gingiva. Most patients exhibit pre-existing oral pigmentation before the onset of this malignancy. Hence, a classic clinical presentation of an irregular, variegated, pigmented lesion on the oral mucosa necessitates suspicion of a melanoma. However, 4% to 15% of oral melanomas are non-pigmented, a feature that can delay early recognition and diagnosis.10,43,44,45
Critically, Kaposi's sarcoma is a malignancy commonly associated with HIV infection. Frequently arising on the palate and gingiva, this malignant connective tissue tumour usually presents as purplish nodules with a tendency to bleed.46
Malignant lymphoproliferative disorders, like non-Hodgkin's lymphoma, arise primarily within the lymph nodes, and involve the Waldeyer's ring, usually in the head and neck region. However, extranodal locations have been seen in the past and cases of gingival lymphomas have also been reported. Clinically, they appear as non-tender swellings, often mimicking an inflammatory process.47,48 Given an appropriate clinical setting, an extranodal lymphoma must be considered in the differential diagnosis.
Metastasis to the jawbones and oral soft tissues accounts only for about 1% of all oral malignancies. Nevertheless, when oral soft tissue metastases do occur, gingiva (54%) is the most commonly affected site. Suggested pathogenesis for the metastatic process, inflammation normally occurring in the gingiva, plays a role in the attraction of metastatic cells towards this site. Lung carcinoma is the most frequently reported malignancy that metastasizes to the gingiva, which occurs significantly in older males. Other tumours with oral metastasis include malignancies of the breast, kidney, bone and colon. Metastases to oral soft tissues develop as rapidly growing expansile masses which tend to ulcerate, bleed and cause pain. In addition, most lesions show associated bony changes on radiographs. However, early lesions of gingival metastasis may resemble hyperplastic or reactive lesions.2,7,8,49
Cysts
Occasionally, jaw cysts can produce circumscribed, fluctuant swellings on the gingiva. In adults, gingival cysts which arise from the proliferation of dental lamina rests, and sometimes lateral periodontal cysts, may produce conspicuous focal gingival swellings. Gingival cysts are frequently described as the extra-osseous counterparts of the intra-osseous lateral periodontal cysts. With a predilection for the mandibular canine-premolar region, these cysts may produce swellings usually less than 1 cm in diameter.50,51
Inflammatory cysts, such as the paradental cysts, mandibular infected buccal cysts and lateral radicular cysts may also produce swellings confined to the gingiva. Paradental cysts result from inflammation around the crowns of erupting teeth, particularly mandibular third molars. They usually present on the buccal or distobuccal aspects of teeth. A similar variety encountered in younger individuals is the mandibular infected buccal cyst which typically affects the mandibular first or second molar teeth. The associated teeth in the above types of cysts are usually vital, which allows differentiation from a radicular cyst on the lateral aspect of tooth roots.51
Dayan et al52 described a peripheral type of odontogenic keratocyst that occurred entirely within the gingiva and had clinical features similar to gingival cysts. Unlike the central variety, they are non-aggressive, usually without recurrence after complete surgical removal.
Systemic diseases
Many systemic disorders present with oral manifestations, of which some occur on the gingiva more frequently. Chloroma or granulocytic sarcoma is an extramedullary myeloid tumour, which is a solid collection of leukaemic cells occurring outside the bone marrow. They are mostly associated with acute myeloid leukaemia.53 Lynch et al54 described a case of granulocytic sarcoma on the gingiva which gave a clinical impression of a pyogenic granuloma.
Strawberry gingivitis, a red oedematous enlargement with petechiae, is a rare manifestation of Wegener's granulomatosis, but characteristic of this granulomatous disease. Initially, this condition may be localized and patches of affected gingiva may coalesce to produce a generalized pattern involving the attached gingiva, which may extend even beyond the mucogingival junction. However, oral lesions appear in only 5–10% of patients affected with this disorder.55,56
Erythematous hyperplastic gingiva may also be seen in cases of Crohn's disease.57
Benign epithelial lesions
Pigmented naevi, known as ‘common mole’ on the skin, are a rare finding in the oral mucosa. These brown or black pigmented lesions may be flat or slightly raised and are seen more often on the palate, but gingiva is not an uncommon location. The clinical appearance is not diagnostic, so a biopsy is usually required to exclude other pigmented lesions and, most importantly, an early malignant melanoma.58 Like naevi, verruca vulgaris, the ‘common wart’, is infrequent in the oral mucosa, but children are more often affected as a result of autoinoculation from warts on their fingers. Clinically, they are white, sessile and exophytic with finger-like projections. Though the majority of them are found on the lips and palate, 10–20% occur on the gingiva.14,59
Bony overgrowths
Localized overgrowths of bone are called exostoses. Most dentists are familiar with these bony protuberances arising from the alveolar bone, frequently distinct on the maxillary buccal and mandibular lingual aspects (torus mandibularis).25,60 However, on occasions, soft tissue hyperplasias and peripheral tumours with calcifications can mimic bony overgrowths, as in Case 3.
Proposal of a diagnostic flowchart
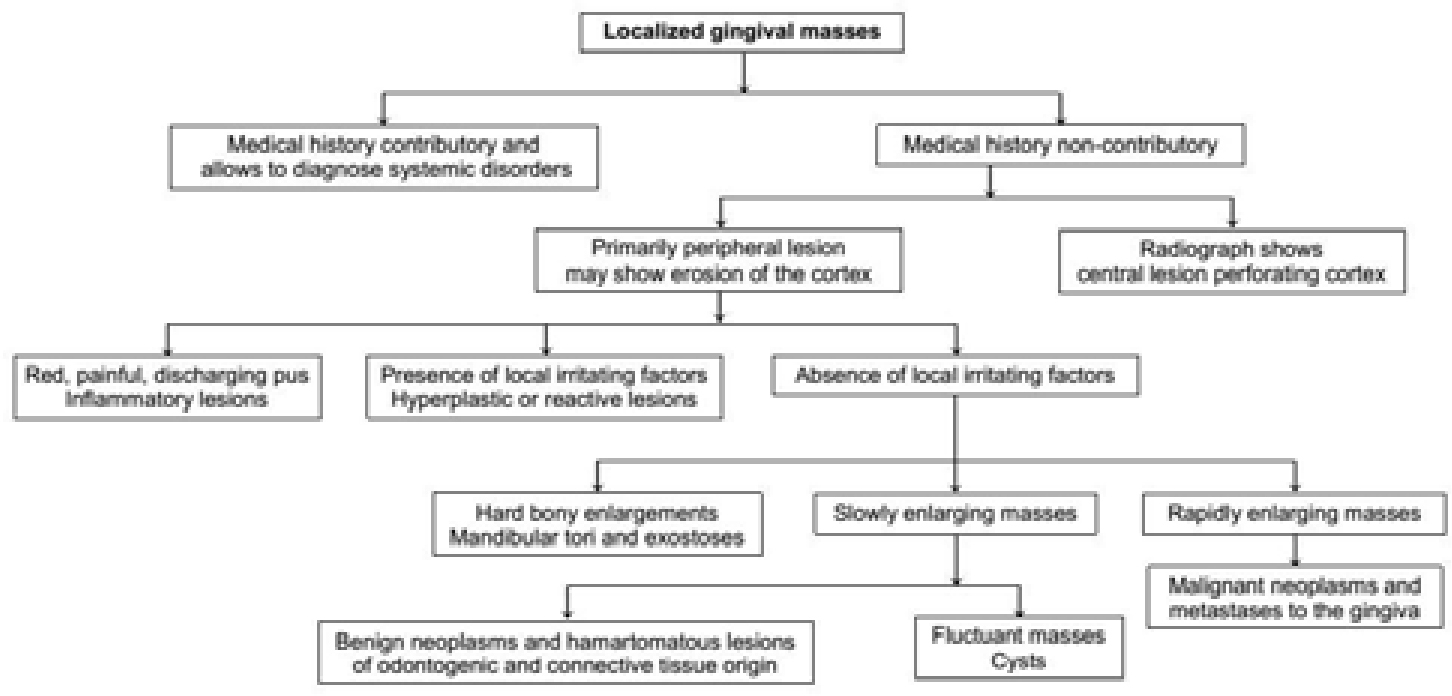
The flowchart (Figure 7) depicts a diagnostic path for LGOs and may aid a dental clinician when such lesions are confronted in daily practice. It methodically prompts the inclusion of a large number of lesions in the differential diagnosis, thereby helping to avoid overseeing any potentially lethal condition affecting the gingiva. Evaluation of a patient presenting with a LGO should include a detailed history followed by clinical and radiographic examinations. Primarily, the history may assist in classifying a lesion as a manifestation of a systemic disorder, although it should be kept in mind that the oral lesion may be the first manifestation of a systemic disease of which the patient may be unaware. Next a LGO should be identified as originating in the soft tissue or bone to help in developing the differential diagnosis. Careful visual, digital and radiographic examinations may indicate the origin. Radiographs help in identifying central lesions perforating the cortex, and peripheral lesions causing bony erosions, but sometimes, in advanced cases, the distinction may not be possible.25 Finally, the literature previously cited may also be of some help to the clinician and some lesions may confidently be diagnosed on clinical grounds alone. However, such a diagnosis remains ‘provisional’ and a definitive diagnosis usually requires confirmation histopathologically.
Figure 7. Diagnostic flowchart.
Treatment options
Precise diagnosis and treatment are essential for managing patients with LGOs. Every patient should receive a thorough oral examination followed by appropriate dental radiographs. The clinical and radiographic findings may provide sufficient information for diagnosis; however, a biopsy is often needed for diagnostic confirmation and for planning further treatment.
Although various techniques, such as scalpel biopsy, punch biopsy, electrocautery and lasers, are available for obtaining biopsy tissue samples, scalpel biopsy is probably the best preferred technique as others have their drawbacks. Heat from lasers and electrocautery distorts tissue producing cytological artefacts, while using the punch biopsy for gingival sites may not be feasible as access may be difficult, especially on lingual aspects.
A biopsy can be incisional or excisional. Incisional biopsy samples only a portion of the lesion, and is most appropriate for large lesions where complete surgical removal is impractical. Excisional biopsy involves complete removal of the lesional tissue. This is most appropriate for small lesions that are easily accessible to surgery. Following biopsy, the excised material needs to be fixed to stop autolysis, and the solution of choice is 10% neutral buffered formalin. This can be obtained from most pathology laboratories along with histopathology request forms and specimen jars.
The clinician has to analyse whether he/she can perform the biopsy: simple excisional biopsies of polyps and reactive lesions are suitable for general dental practice, and can be both diagnostic and curative at the same time. However, when a systemic disease or malignancy is suspected, the biopsy should be undertaken in a hospital setting following appropriate referral. Such biopsies should be performed by the surgeon who is going to initiate the treatment, and should not be attempted in general dental practice.
Conclusion
Although most of the LGOs are reactive lesions, the gingiva can also succumb to a variety of neoplasms. Hence, awareness of diverse conditions that manifest as a LGO may assist in diagnosis and treatment planning. Gingival overgrowths confined to the soft tissue may be managed by surgical excision, followed by histopathological evaluation. Whereas, lesions of central origin, or those associated with systemic disorders, may require immediate referral to a specialist for definitive management. A dental practitioner should promptly identify and refer suspicious lesions that require specialist evaluation.