Ross RB, Johnston MC.Baltimore: Williams and Wilkins; 1978
Piggot RW. Organization of cleft lip and palate services – results of a questionnaire. Br J Plast Surg. 1992; 45:385-387
Williams AC, Shaw WC, Devlin HB. Provision of services for cleft lip and palate in England and Wales. Br Med J. 1994; 309
Fitzpatrick DR, Raine PA, Boorman JG. Facial clefts in the West of Scotland 1980–84: epidemiology and genetic diagnoses. J Med Genet. 1994; 31:126-129
Gregg T, Boyd D, Richardson A. The birth prevalence of cleft lip and palate in Northern Ireland from 1980–1990. Br J Orthod. 1994; 21:387-392
Bellis TH, Wohlgemuth B. The incidence of cleft lip and palate deformities in the South-East of Scotland (1971–1990). Br J Orthod. 1999; 26:121-125
London: HMSO; 1998
Waitzman N, Scheffler RM, Romano PS.Lanham (MD): University Press of America; 1996
Sell D, John A, Harding-Bell A, Sweeney T, Hegarty F, Freeman J. Cleft audit protocol for speech (CAPS-A): a comprehensive training package for speech analysis. Int J Lang Commun Disord. 2009; 44:529-548
Atack NE, Hathorn IS, Semb G, Dowell T, Sandy JR. A new index for assessing surgical outcome in unilateral cleft lip and palate subjects aged five: reproducibility and validity. Cleft Palate Craniofac J. 1997; 34:242-246
Kindelan JD, Nashed RR, Bromige MR. Radiographic assessment of secondary autogenous alveolar bone grafting in cleft lip and palate patients. Cleft Palate Craniofac J. 1997; 34:195-198
Mars M, Plint DA, Houston WJ, Bergland O, Semb G. The Goslon Yardstick: a new system of assessing dental arch relationships in children with unilateral clefts of the lip and palate. Cleft Palate J. 1987; 24:314-322
Bergland O, Semb G, Abyholm FE. Elimination of the residual alveolar cleft by secondary bone grafting and subsequent orthodontic treatment. Cleft Palate J. 1986; 23:175-205
Mossey PA, Clark JD, Gray D. Preliminary investigation of a modified Huddart/Bodenham scoring system for assessment of maxillary arch constriction in unilateral cleft lip and palate subjects. Eur J Orthod. 2003; 25:251-257
Tonni G, Centini G, Rosignoli L. Prenatal screening for fetal face and clefting in a prospective study on low-risk population: can 3-and 4-dimensional ultrasound enhance visualization and detection rate?. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2005; 100:420-426
Beaumont D. The role of the clinical nurse specialist within the cleft lip and palate team: CLP series part 2. Ortho Update. 2012; 5:48-51
Konst EM, Prahl C, Weersink-Braks H, De Boo T, Prahl-Andersen B, Kuijpers-Jagtman AM, Severens JL. Cost-effectiveness of infant orthopedic treatment regarding speech in patients with complete unilateral cleft lip and palate: a randomized three-center trial in the Netherlands (Dutchcleft). Cleft Palate Craniofac J. 2004; 41:71-77
Pfeifer TM, Grayson BH, Cutting CB. Nasoalveolar molding and gingivoperiosteoplasty versus alveolar bone graft: an outcome analysis of costs in the treatment of unilateral cleft alveolus. Cleft Palate Craniofac J. 2002; 39:26-29
Clark SL, Teichgraeber JF, Fleshman RG, Shaw JD, Chavarria C, Kau CH, Gateno J, Xia JJ. Long-term treatment outcome of presurgical nasoalveolar molding in patients with unilateral cleft lip and palate. J Craniofac Surg. 2011; 22:333-336
McComb H. Primary correction of unilateral cleft lip nasal deformity: a 10-year review. Plast Reconstr Surg. 1985; 75:791-799
Management of patients with non-syndromic clefts of the lip and/or palate part 1: from antenatal diagnosis to primary surgery Grant T McIntyre Dental Update 2024 41:8, 707-709.
Patients with clefts of the lip and/or palate require input from a diverse group of medical, surgical, dental and parasurgical specialties working as part of a multidisciplinary team in the UK. Co-ordinated care ensures that the patient receives optimal treatment whilst minimizing the burden of care for the NHS and family. The primary care dentist has an important role in the overall management of patients with clefts. Because the dentist-patient/parent relationship is of a long-term nature, the primary care dentist can also provide useful support and advice for families as they progress through the care pathway. This three-part article will illustrate the integration of dentistry with the other aspects of care.
Clinical Relevance: Dentists should be aware of the different types of cleft lip and/or palate that occur and the role of the dentist in the overall management of patients who have clefts.
Article
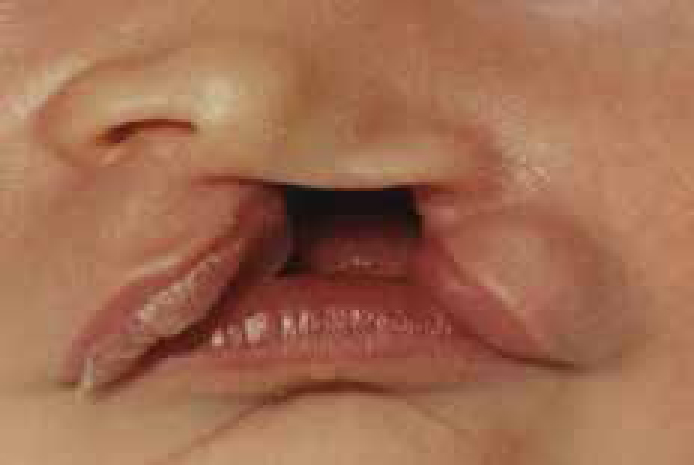
Non-syndromic clefts of the lip and palate include cleft lip with or without cleft palate [CL(P)] and isolated cleft palate (CP). The variety of CL(P) phenotypes includes:
Unilateral cleft lip (UCL) with or without alveolar notching;
Bilateral cleft lip (BCL) with or without alveolar notching;
Unilateral cleft lip and palate (UCLP);
Bilateral cleft lip and palate (BCLP).
The lip cleft can be further described as complete or incomplete depending on whether the cleft extends into the base of the nose or not.
Figures 1–4 show the main non-syndromic types of cleft that dentists are likely to encounter: a unilateral cleft lip (incomplete), a unilateral cleft lip and palate (complete), a bilateral cleft lip and palate (complete) and an isolated cleft palate.
Globally, the incidence of cleft lip and palate is approximately 1.35 in every 1000 live births,1,2 meaning that a baby with a cleft is born somewhere in the world every 3.6 minutes. There is, however, considerable geographical and ethnic variation in the epidemiology and, in the UK, the birth prevalence rate is approximately 650 cases per year, accounting for 65% of all congenital craniofacial abnormalities.3 Interestingly, the ratio of CL(P) to CP is approximately 2:1 in England and Wales (Table 1), however, there is an increased prevalence of CP in Scotland and N Ireland and, as a result,4,5,6 the ratio approximates 1:1. In general, boys have an increased prevalence of CL(P) when compared to girls (2:1), whilst girls are more likely to be affected by CP (1:2).
Cleft type
%
UCLP
40
CP
30
BCLP
10
CL
10
Other eg submucous cleft
10
Of unilateral clefts, almost two-thirds are left-sided. Although this article will mainly focus on non-syndromic clefting, there are over 300 syndromes where a cleft is part of the phenotype, accounting for 25% of patients with CP and 12% of those with CL(P). Around 50% of the remaining patients have less well defined anomalies.
Prevention
The aetiology of cleft lip and/or palate includes genetic factors, environmental factors and gene-environment interactions (GEIs). Specific genetic factors have been identified (eg MSX1, IRF-6, SATB2, TGFβ3, TBX22), but a consistently identifiable causative gene has not been detected across populations. Whilst it is known that certain medicines, such as the anticonvulsant drug phenytoin, drinking excessive amounts of alcohol, smoking and being exposed to high levels of ionizing radiation during pregnancy have been implicated in the aetiology of clefting, folic acid deficiency has somewhat surprisingly not been linked to an increased prevalence of cleft lip and palate. Nevertheless, a multivitamin tablet containing 400 μg folic acid (vitamin B9) is recommended for women in the peri-conceptual period.
As the aetiology is regarded as being polygenic and multifactorial, primary prevention of clefting is not possible, yet risk reduction through the minimization of environmental influences is advisable. Clearly, for families where there is more than one affected member, the likelihood of a genetic contribution is increased and these ‘at risk’ families should be offered the opportunity of referral for genetic counselling in relation to the specific risk of their children having a cleft. Primary care dentists may be asked at any stage by patients and potential parents about the recurrence risk, which for a couple with one affected child is 50 times higher than the risk in the general population.
Management
Children and adults with CL(P) are managed in the UK by a multidisciplinary team comprising various health professionals from different specialist backgrounds who work closely together. The team generally includes:
Cleft Nurse Specialist;
Cleft Surgeon;
Speech and Language Therapist;
Orthodontist;
Paediatric Dentist;
Audiologist and/or Ear, Nose and Throat (ENT) Specialist;
Paediatrician; with input from Clinical Psychology, Genetics and Sonography.
The 11 current multidisciplinary teams in the UK and Ireland (Table 2) were re-organized into ‘hub and spoke’ services following the CSAG report7 with the ‘hubs’ based in the main geographic population centres for multidisciplinary clinics and surgery. Many operate ‘outreach’ multidisciplinary clinics in other areas of their regions to avoid patients having to travel large distances for clinic appointments with Speech and Language Therapy, Paediatric Dentistry, Orthodontic treatment and other aspects of care being provided by the ‘spokes’ as close to patients' homes as possible. Whilst it has been estimated that the cost of treating a craniofacial birth defect such as cleft lip and/or palate is $101,000 in California,8 most healthcare professionals involved in cleft care would argue that this represents excellent value for money in relation to the number of episodes of care per patient.
Name of Multidisciplinary Cleft Team
Location
Cleft Net East
Addenbrookes Hospital, Cambridge
North Thames Cleft Service
Great Ormond Street Hospital for ChildrenSt Andrew's Centre, Broomfield Hospital, Chelmsford
Northern and Yorkshire Cleft Service
Leeds General InfirmaryRoyal Victoria InfirmaryNewcastle-upon-Tyne
Northern Ireland Cleft Service
Royal Victoria Hospital, Belfast
Northwest England, Isle of Man, North Wales Cleft Service
Alder Hey Hospital, Liverpool Royal Manchester Children's Hospital
Republic of Ireland
Children's University Hospital, DublinLady's Children's Hospital Crumlin, Dublin
Cleft Service in Scotland (CLEFTSiS)
Royal Hospital for Sick Children, EdinburghRoyal Hospital for Sick Children, Glasgow
Salisbury District HospitalThe John Radcliffe, Oxford
Trent Cleft Service
Nottingham City Hospital
West Midlands Cleft Service
Birmingham Children's Hospital
Wider role of the multidisciplinary team
In addition to treatment, the multidisciplinary team has an important role in monitoring growth and development of the individual patient, audit data collection and analysis of outcomes and service development. The audit records that are collected and the subsequent assessments are detailed in Table 3. Some cleft teams run specific audit clinics in order to capture these audit data, whilst others integrate audit data collection with routine progress assessment clinics. Most members of the multidisciplinary teams belong to the Craniofacial Society of Great Britain and Ireland, which provides an annual forum for audit and service improvement on a UK basis, whilst most centres benchmark their results with those neighbouring regions through tri-centre or quad-centre audit programmes.
Alveolar bone graft score using Kindelan index11 at 3–6 months post-operatively using occlusal radiograph;
GOSLON = Great Ormond Street, London and Oslo index scored on dental study models;12
Bergland score for alveolar bone grafting once cleft canine has erupted using occlusal radiograph;13
MHB score = modified Huddart-Bodenham index scored on dental study models;14
PAR score reduction calculated from study models recorded at start and completion of orthodontic treatment;
Lateral cephalometric radiograph – assessment of dentoskeletal relationships and orthognathic surgery if necessary.
Antenatal
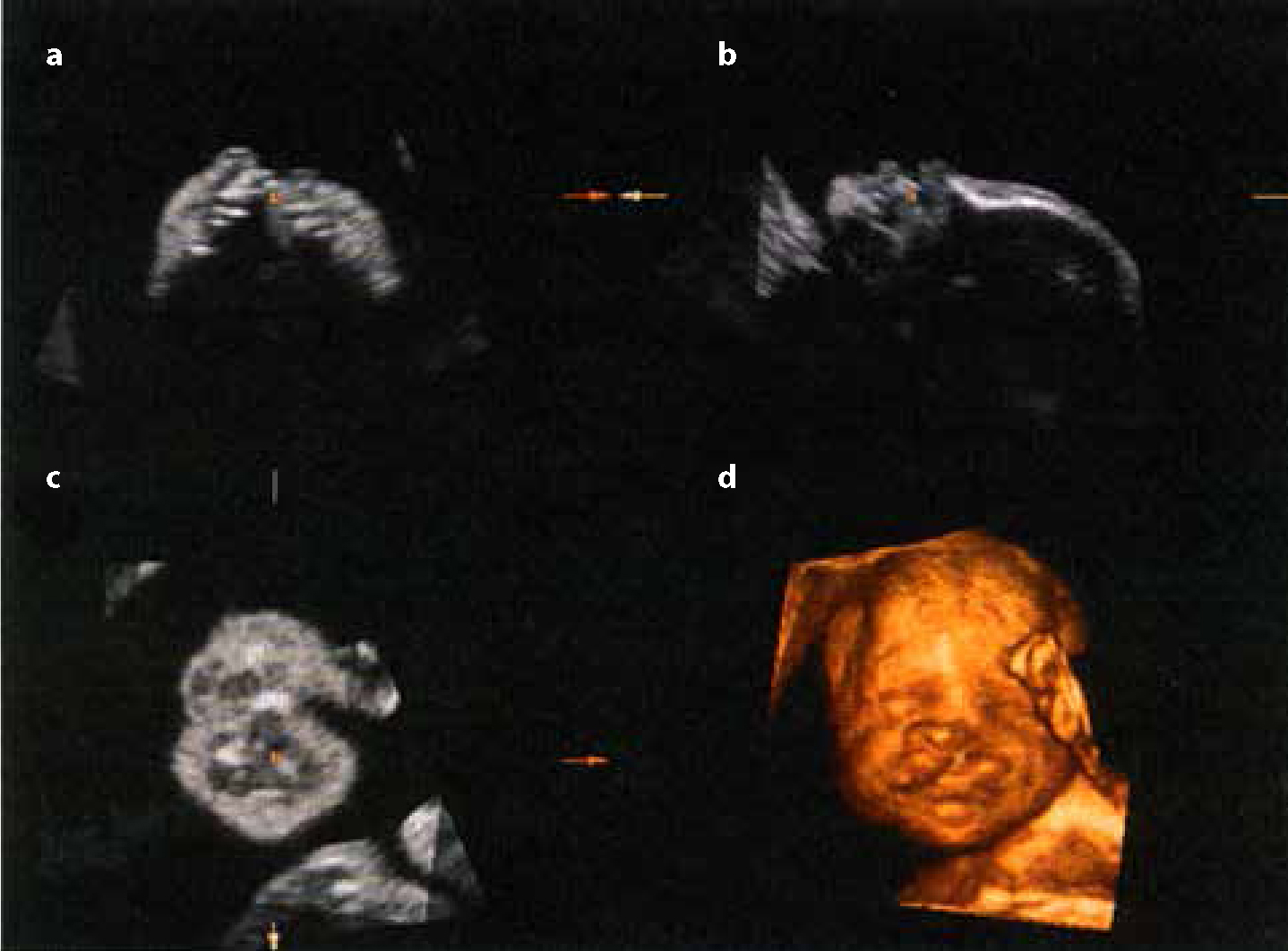
For most families, the first indication that their child has a congenital defect such as a cleft is antenatally at the 20-week ultrasonography (anomaly) scan. Clefts of the alveolus and palate are much less easily detected than clefts of the lip and depend on the extent of the defect, the position of the baby, maternal obesity and the sonographic equipment that is used. In many centres, 3D (Figure 5) and 4D (real-time) ultrasonography has superseded traditional 2D technology, although the sensitivity and specificity of newer technologies for cleft lip and palate diagnosis are broadly similar.15 A positive antenatal diagnosis can be a difficult time for many parents, with the joy and excitement of parenthood being tinged by feelings of shock, stress, anxiety and guilt that the cleft has somehow been their fault. The first questions parents ask at this stage are:
What caused the cleft?
Why will our baby have a cleft?
Will our child be OK?
Figure 5. 3D ultrasonography views. Reproduced with permission from the American Institute of Ultrasound in Medicine: (a) axial; (b) parasagittal; (c) coronal and (d) 3D rendered views.
It is therefore important that the parental concerns are managed appropriately at the antenatal diagnosis stage. Parents are provided with the excellent range of information produced by the Cleft Lip and Palate Association (CLAPA) before leaving the scanning department. A referral is also made to a member of the cleft team within 48 hours of a positive antenatal diagnosis for counselling and a general discussion on the future care of their child in relation to the potential phenotype. In many areas of the UK, the Cleft Nurse Specialist (CNS) will make telephone contact and may undertake a domiciliary visit to discuss the diagnosis with the prospective parents.16 In other areas, this service is provided by other members of the multidisciplinary team. Follow-up contact later in the pregnancy provides reassurance for potential parents. Whilst many prospective parents find the psychological ability to prepare themselves, their family and friends for the birth of their baby useful, a positive antenatal diagnosis can lead some parents of an otherwise healthy foetus to contemplate termination.
Newborn
On the birth of the baby, the Cleft Nurse Specialist will be contacted for advice on feeding, oral care and sleeping position; all important to ensure general and oral health.16 In some teams, the Specialist Speech and Language Therapist undertakes this role. The designated contact will normally aim to meet the family within 24 hours of birth, although feeding advice can be provided by telephone or telemedicine in remote/rural areas. Breast feeding or feeding with expressed breast milk is encouraged in line with UNICEF guidelines. For parents who choose to bottle feed their infant, a range of bottles and teats are available (Figure 6). These can be sourced through the Cleft Lip and Palate Association (CLAPA) website (www.clapa.com). Both the bottles shown in Figure 6 are useful where there are problems with the baby's suck to ensure that babies feed well. By reducing the amount of energy the baby has to use for feeding, growth is optimized. The general advice of ‘back to sleep’ is discouraged for babies with a cleft palate and ‘side sleeping’ is encouraged. In some cases of Pierre Robin sequence (characterized by a micrognathic mandible, a cleft palate and glossoptosis) due to the significant possibility of apnoeic episodes as a result of airway obstruction, a nasopharyngeal airway may also be required as a precautionary measure. Any concerns about sleep apnoea will trigger a referral for a sleep study and further management by a respiratory physician. Pacifiers are discouraged and new parents are advised to keep the baby's mouth and cleft area clean and to keep a watchful eye for intra-oral candidosis. Any neonatal teeth in the region of the cleft may need to be removed, particularly if the baby is breast fed! Input from the local Health Visitor in relation to other aspects of child development and family support at this stage can be invaluable. Within four weeks of birth, a routine newborn hearing screening test will be undertaken using either an automated otoacoustic emission (AOAE) test or an auditory brainstem response (ABR) evaluation.
Figure 6. Feeding bottles – (a) Nurture 250 ml ‘squeezy’ bottle (www.vitalbaby.co.uk) which can help deliver the correct amount of milk into the baby's mouth; (b) Haberman Feeder (www.athrodax.co.uk) which incorporates a soft variable-flow teat with a pump action valve.
A formal diagnosis is made when the baby is assessed by the multidisciplinary team and the child is then registered on the CRANE database for England, Wales and N Ireland or CLEFTSiS database in Scotland. A comprehensive oral examination will be undertaken to determine the nature and extent of the cleft and any associated features/dysmorphisms. Where these are thought to be linked to the cleft, a referral to the Geneticist on the multidisciplinary team will be made as identifying a syndrome is of value to ensure that children receive appropriate care for all aspects of their condition as they grow and develop.
Primary surgery
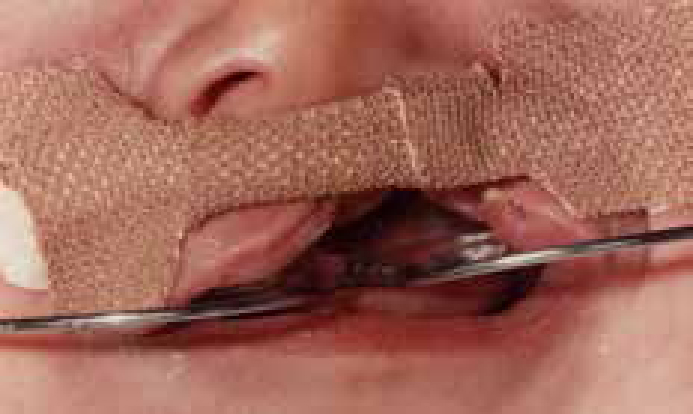
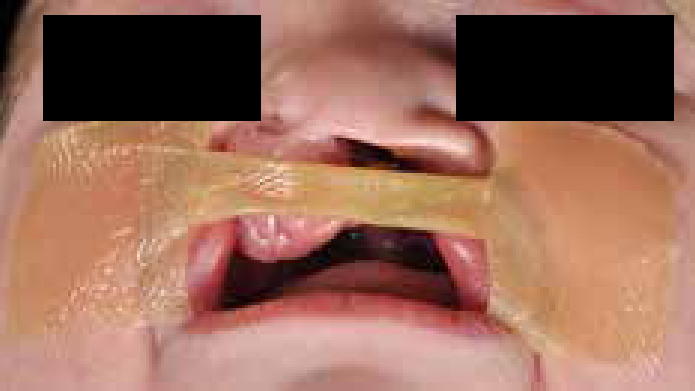
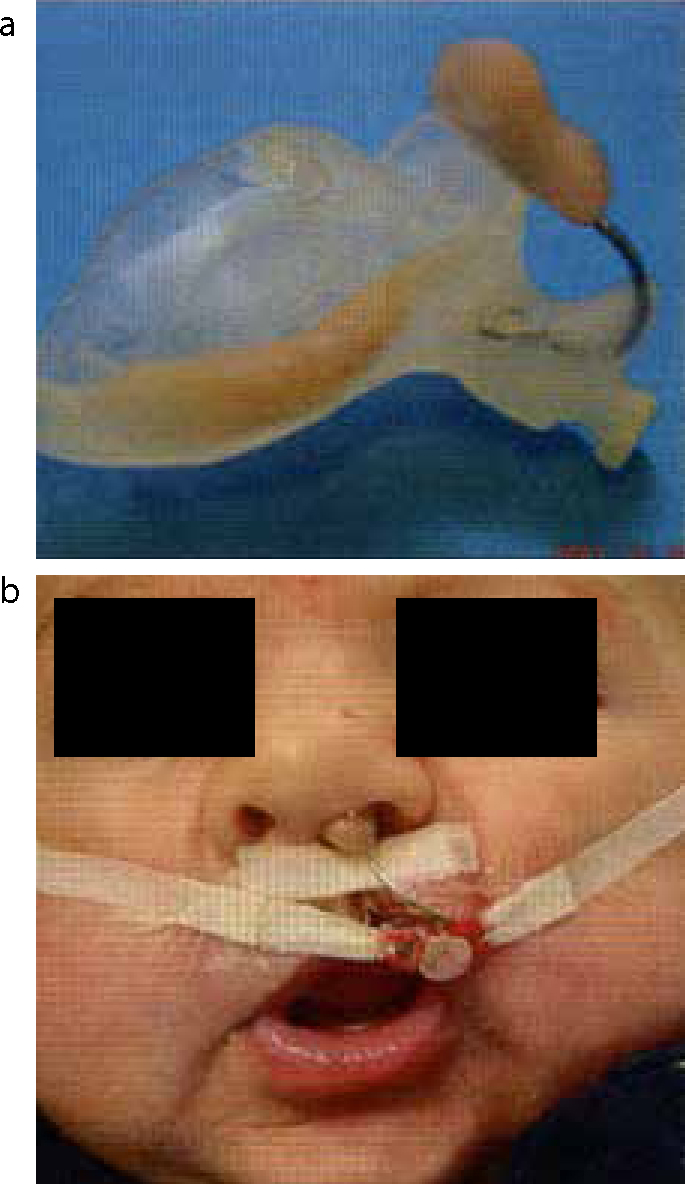
Children with a cleft lip normally undergo a lip repair procedure at around 3–5 months of age. Wide unilateral clefts and some bilateral clefts can initially be managed with presurgical orthopaedics or a lip adhesion surgical procedure to narrow the cleft and reduce the amount of tension that would otherwise adversely influence the outcome of the lip surgery. Whilst, historically, presurgical orthopaedics involved an intra-oral plate in conjunction with lip-strapping for most babies (Figure 7), the benefits have been shown to be disappointing when evaluated in a long-term randomized controlled trial17 and other studies. However, lip-strapping is effective in wide clefts and, as such, Orthodontists provide this service using either Dynacleft tape (http://www.canica.com/dynacleft.asp) or a generic skin tape/adhesive surgical dressing material (Figure 8). In the USA, naso-alveolar moulding (NAM) is a relatively recent development (Figure 9). This technique involves correction of the nasal cartilage deformity, stretching of nasal mucosal lining, non-surgical columella lengthening and moulding of alveolar process. It remains controversial, with proponents18 and opponents19 claiming either success or otherwise.
Figure 7. Presurgical orthopaedic treatment with plate and strapping.Figure 8. Presurgical orthopaedic treatment with lip-strapping (same patient as Figure 3).Figure 9.
(a) Naso-alveolar moulding (NAM) appliance and (b) appliance in place with elastics and tapes. (Reprinted from Seminars in Orthodontics Vol 15. Santiago PE, Grayson BH. Role of the craniofacial orthodontist on the crani-ofacial and cleft lip and palate team, pp225–243. Copyright 2009, with permission from Elsevier).
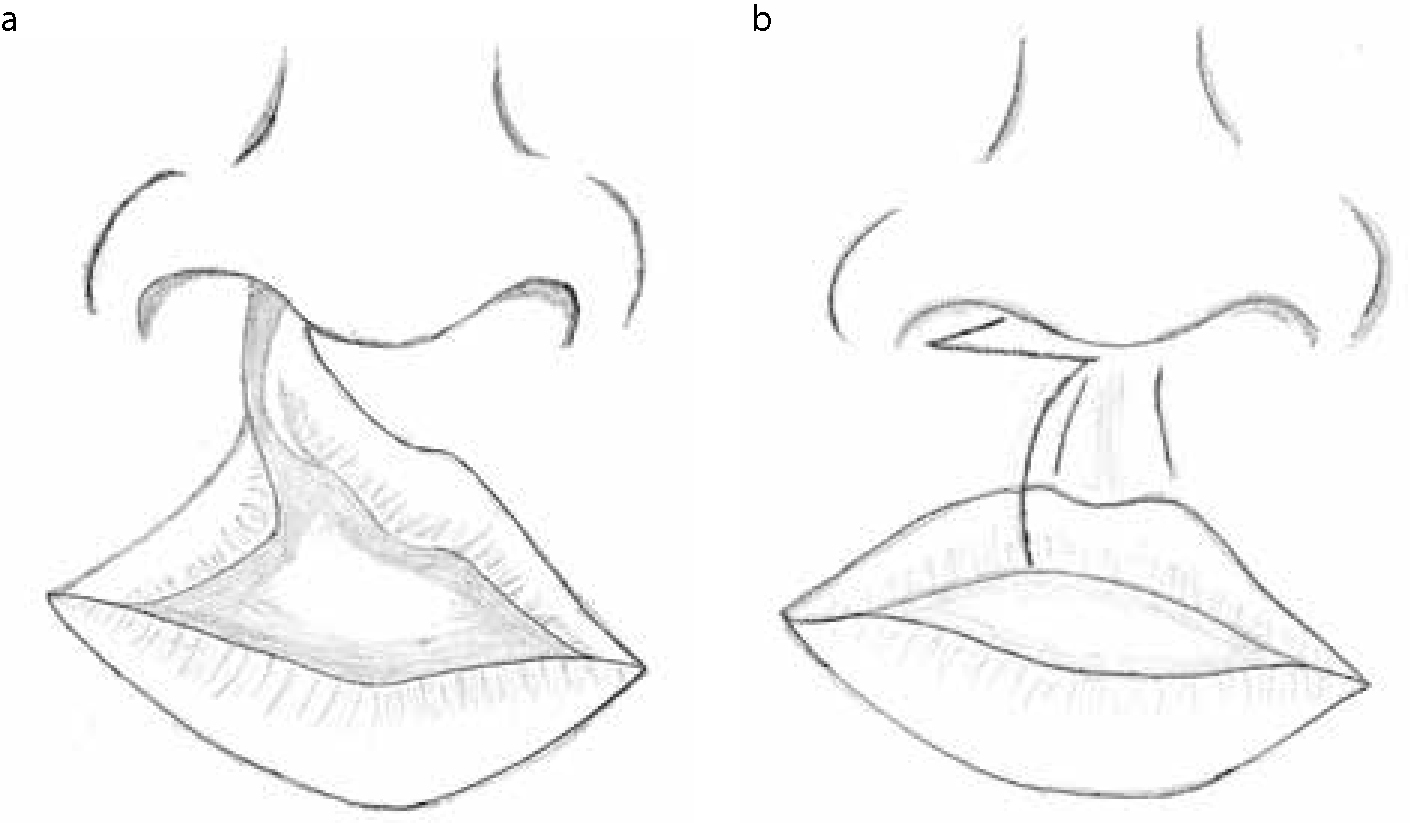
The lip surgery is undertaken by a rotation-advancement procedure originally described by Millard with a limited lateral (alar sill/crease) incision (Figure 10 a, b) and produces excellent results (Figure 11 a, b). A McComb nasal correction procedure to improve nasal aesthetics20 and a vomerine flap to repair the hard palate are carried out simultaneously in some centres. Feeding resumes as soon as possible post-operatively, and most babies are hungry, having been starved pre-operatively! Where non-resorbable sutures are used, a short general anaesthetic is required around five days later for suture removal.
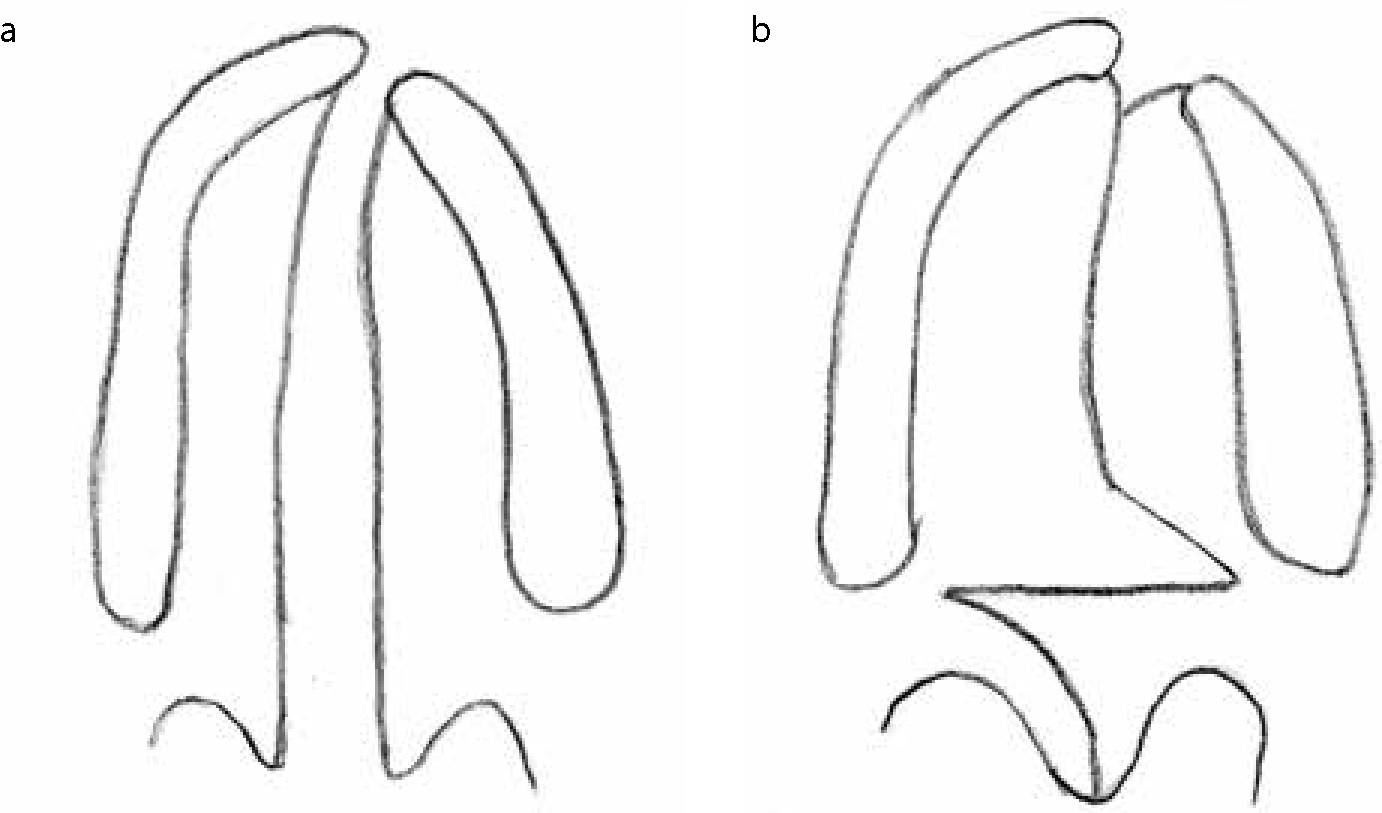
The palate is repaired normally in the UK by 9 months of age, although this is deferred in babies with Pierre Robin sequence until around 12 months, to allow further mandibular growth to take place and improve the patency of the airway post-operatively. Where a vomerine flap has not been undertaken along with the lip repair, both the hard and soft palate are repaired at the same time. The historical Von Langenbeck method of repairing the hard palate using lateral releasing incisions has been superseded by midline closure, where possible; the V-Y closure technique (which may involve two stages) or a Furlow double opposing Z-plasty (Figure 12). These techniques are thought to have less adverse impact on midfacial growth. The soft palate may also require an intravelar veloplasty (with radical dissection and re-orientation of the muscle fibres). It has been known for some time that early palate repair promotes good speech development, whilst later surgery leads to better facial growth outcomes. Research is continuing to investigate optimal timing through the Timing of Primary Surgery for Cleft Palate (TOPS) randomized controlled trial. Children with bilateral clefts may require staged surgery.
Figure 12.
(a, b) Palate repair (Furlow Z-plasty).
The second part of this article will provide details of the care of patients with clefts from primary surgery through to alveolar bone grafting.