
Article
With an increasing elderly population there is an increased prevalence of edentulism and a need for complete dentures.1,2 Traditionally, complete loss of teeth is restored with a conventional complete denture. Several problems are reported to be associated with the use of complete dentures.3,4,5 These problems include discomfort, looseness of dentures, adaptation difficulty and phonetics. These complications are not uncommon and dental practitioners need to be able to diagnose and manage such complications. In this clinical tip, a 62-year-old male patient presented to the Dublin Dental University Hospital (DDUH) complaining of a loose upper complete denture and requesting a new one to be made. Clinical examination revealed a completely edentulous upper jaw and Kennedy Class I lower arch. The upper edentulous jaw was restored with a conventional complete denture while the lower jaw was not restored. Both arches had good alveolar ridges with a Class II skeletal relationship. The patient's denture stability and retention were poor and it was approximately 10 years old. After discussing treatment options with patient, the following treatment was carried out: upper complete denture and lower chrome cobalt removable partial denture using the RPI system. A new upper complete denture was made along with a lower chrome cobalt removable partial denture. On review, the patient reported difficulties in speech and making a whistle sound when pronouncing words with sibilants; in particular when he pronounced ‘flowers’, which was heard as ‘flowersh’.
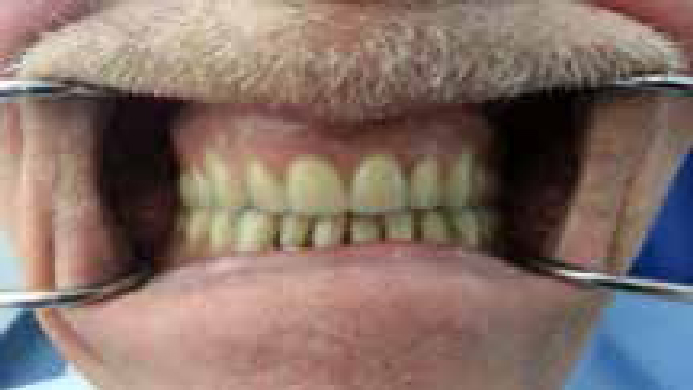
A subsequent examination revealed an increase in the closest speaking space. Further clinical examination was carried out to study the cause of the existing speech problem. The clinical examination revealed that the incisor relationship between the upper artificial and lower natural teeth, in the normal occlusal vertical dimension (OVD), was about 5 mm and a large space between the incisal edges of the lower anterior teeth and the palatal surface of the denture could be seen. This relationship was dictated by the skeletal relationship as the patient had a Class II skeletal relationship. Furthermore, the incisal edge of the upper two central incisors was placed almost at an equal level incisally with those of the lateral incisors (Figure 1). Any of these findings may have caused the speech problem. Therefore, Red beading wax® (Associated Dental Products Ltd, Kemdent Works, Swindon, UK) was added to the palatal surface of the upper anterior teeth in order to reduce the horizontal overlap. A little improvement was observed but the patient still had speech difficulties. The length of the four incisors was then increased by about 2 mm. Speech returned to normal and the patient was able to create intelligible speech. The patient was involved in a conversation and different sibilant sounds were pronounced. Accordingly, the options were to reset the upper four incisors in the laboratory and to retry the denture in wax again. This is a lengthy clinical and laboratory procedure which leaves the patient without his denture for some time. The second option was to replace the beading wax with an acrylic resin which has the same shade as the teeth. However, the acrylic is liable to discoloration and needs to be frequently changed. As the patient declined to leave the clinic without the denture, the second option was carried out. Therefore, the wax was replaced by auto-polymerizing acrylic (Snap® Parkell, Inc, NY, USA) (Figure 2). An acrylic resin of the same shade as the teeth was added to the teeth and the palatal surface of the denture in order to regain the normal phonetics. The acrylic was adjusted until the patient was able to create intelligible speech.

One week later, the patient was satisfied with the result. This method is fast and can be carried out in clinic, but should be considered as a provisional measure only.