Garavello W, Bertuccio P, Levi F, Lucchini F, Bosetti C, Malvezzi M The oral cancer epidemic in central and eastern Europe. J Int du Cancer. 2010; 127:(1)160-71
Montoro JR, Tavares MG, Melo DH, Franco Rde L, Mello-Filho FV, Xavier SP Mandibular ameloblastoma treated by bone resection and immediate reconstruction. Braz J Otorhinolaryngol. 2008; 74:(1)155-157
Dunn JL, Olan WJ, Bank WO, Narang AK, Schwartz AM. Giant ameloblastoma: radiologic diagnosis and treatment. Radiographics: a review publication of the Radiological Society of North America Inc. 1997; 17:(2)531-536
Erdmann D, Follmar KE, Debruijn M, Bruno AD, Jung SH, Edelman D A retrospective analysis of facial fracture etiologies. Ann Plast Surg. 2008; 60:(4)398-403
Carek PJ, Dickerson LM, Sack JL. Diagnosis and management of osteomyelitis. Am Fam Phys. 2001; 63:(12)2413-2420
Drozdzowska B. [Osteonecrosis of the jaw].: Martwica zuchwy; 2011
Martin LP, Gallo LJ, Pons MC, Soto MJ, Carretero JL, Garcia MB. Mandibular osteoradionecrosis: use of sequential fibula free flaps for a remote sequence of complications. Craniomaxill Trauma Reconstr. 2010; 3:(2)91-95
Choumerianou DM, Dimitriou H, Kalmanti M. Stem cells: promises versus limitations. Tissue engineering Part Bd, Reviews. 2008; 14:(1)53-60
Jimi E, Hirata S, Osawa K, Terashita M, Kitamura C, Fukushima H. The current and future therapies of bone regeneration to repair bone defects. Int J Dent. 2012; 2012
Saxena AK, Singh D, Gupta J. Role of stem cell research in therapeutic purpose – a hope for new horizon in medical biotechnology. J Exp Ther Oncol. 2010; 8:(3)223-233
Rana M, Warraich R, Kokemuller H, Lemound J, Essig H, Tavassol F Reconstruction of mandibular defects – clinical retrospective research over a 10-year period. Head Neck Oncol. 2011; 3:23-29
Buchbinder D, Urken M. Chapter 82: Mandibular Reconstruction.Philadelphia: Lippincott; 1993
Sandor GKB, Lindholm TC, Clokie CML. Bone regeneration of the cranio-maxillofacial and dento-alveolar skeletons in the framework of tissue engineering. In: Ashammakhi A, Ferretti P (eds). Tampere2003
Oppenheimer AJ, Tong L, Buchman SR. Craniofacial bone grafting: Wolff's Law revisited. Craniomaxill Trauma Reconstr. 2008; 1:(1)49-61
Richardson CR, Mellonig JT, Brunsvold MA, McDonnell HT, Cochran DL. Clinical evaluation of Bio-Oss: a bovine-derived xenograft for the treatment of periodontal osseous defects in humans. J Clin Periodontol. 1999; 26:(7)421-428
Pryor LS, Gage E, Langevin CJ, Herrera F, Breithaupt AD, Gordon CR Review of bone substitutes. Craniomaxill Trauma Reconstr. 2009; 2:(3)151-160
O'Fearraigh P. Review of methods used in the reconstruction and rehabilitation of the maxillofacial region. J Ir Dent Assoc. 2010; 56:(1)32-37
Glenn MG. Scapular osteocutaneous free flap for mandibular reconstruction. West J Med. 1989; 150:(4)450-451
National Institute for Health and Care Excellence. Total prosthetic replacement of the temporomandibular joint (IPG329). http://guidance.nice.org.uk/IPG329 (cited 6/07/2013)
Speculand B. Current status of replacement of the temporomandibular joint in the United Kingdom. Br J Oral Maxillofac Surg. 2009; 47:(1)37-41
Sinno H, Tahiri Y, Gilardino M, Bobyn D. Engineering alloplastic temporomandibular joint replacements. Mcgill J Med. 2011; 13:(1)63-72
van Steenberghe D, Callens A, Geers L, Jacobs R. The clinical use of deproteinized bovine bone mineral on bone regeneration in conjunction with immediate implant installation. Clin Oral Implants Res. 2000; 11:(3)210-216
Schlegel AK, Mohler H, Busch F, Mehl A. Preclinical and clinical studies of a collagen membrane (Bio-Gide). Biomaterials. 1997; 18:(7)535-538
Spiegelberg B, Parratt T, Dheerendra SK, Khan WS, Jennings R, Marsh DR. Ilizarov principles of deformity correction. Ann R Coll Surg Engl. 2010; 92:(2)101-105
Nanjappa M, Natashekara M, Sendil Kumar C, Kumaraswamy SV, Keerthi R, Ashwin DP ‘Transport distraction osteogenesis for reconstruction of mandibular defects': our experience. J Maxillofac Oral Surg. 2011; 10:(2)93-100
Kao RT, Murakami S, Beirne OR. The use of biologic mediators and tissue engineering in dentistry. Periodontology 2000. 2009; 50:127-153
Kuriakose MA, Sharma M, Iyer S. Recent advances and controversies in head and neck reconstructive surgery. Indian J Plast Surg. 2007; 40:3-12
Arora V, Arora P, Munshi AK. Banking stem cells from human exfoliated deciduous teeth (SHED): saving for the future. J Clin Pediatr Dent. 2009; 33:(4)289-294
Zheng Y, Liu Y, Zhang CM, Zhang HY, Li WH, Shi S Stem cells from deciduous tooth repair mandibular defect in swine. J Dent Res. 2009; 88:(3)249-254
d'Aquino R, De Rosa A, Lanza V, Tirino V, Laino L, Graziano A Human mandible bone defect repair by the grafting of dental pulp stem/progenitor cells and collagen sponge biocomplexes. Eur Cell Mater. 2009; 18:75-83
Alhadlaq A, Mao JJ. Tissue-engineered neogenesis of human-shaped mandibular condyle from rat mesenchymal stem cells. J Dent Res. 2003; 82:(12)951-956
Watt FM, Driskell RR. The therapeutic potential of stem cells. Philos Trans R Soc Lond B Biol Sci. 2010; 365:(1537)155-163
Bone defects of the jaws: moving from reconstruction to regeneration Elena Kyriakidou Norma O'Connor Nicholas J Malden Victor R Lopes Dental Update 2024 41:7, 707-709.
Authors
ElenaKyriakidou
BDS, MFDS, MClinDent, MOralSurg
Academic Clinical Fellow/Specialty Trainee in Oral Surgery, School of Clinical Dentistry, University of Sheffield
Professor of the Combined Department of Oral and Maxillofacial Surgery and Oral Medicine, Edinburgh Dental Institute and St John's Hospital, Livingston, UK
Jaw reconstruction is necessary for a variety of reasons including neoplastic disease, traumatic injuries, infective/inflammatory lesions, and congenital defects. Such defects can be a significant handicap for patients leading to physiological and psychological morbidity. Maxillofacial bone reconstruction remains challenging for the reconstructive surgeon; yet it has evolved significantly over recent years. The current state of the art reconstruction is via the use of vascularized osseous flaps. Modern developments in regenerative medicine propose a future for stem cells in the regeneration of bone for jaw defects.
Clinical Relevance: Knowledge of the current methods of reconstruction and advances in the field of tissue engineering is of interest to dental clinicians.
Article
The mandible is the strongest and largest bone in the face and plays a central role in function and aesthetics in the oral and maxillofacial region.1 It is the only unpaired and movable facial bone and it outlines the profile and appearance of the lower face.2 The muscles of mastication attach to the mandible aiding mandibular movements and functions such as speech, airway support, swallowing and mastication.3
Maxillofacial bone defects may be due to:
Neoplastic disease;
Trauma;
Infective/Inflammatory disease;
Congenital deformity.
Neoplastic disease
The most common indication for maxillofacial bone reconstruction is following ablation of neoplastic disease. Oral squamous cell carcinoma represents 3–4% of total body cancer in the UK with incidence rate of 2.8/100000.4,5
Ameloblastoma (Figure 1) is the commonest benign neoplasm of the jaws and typically affects the posterior mandible. It is an odontogenic tumour which exhibits a locally aggressive behaviour and, despite its slow growth, is extremely invasive and rarely metastases. Its treatment comprises a wide surgical excision with 2 cm margin frequently leaving a considerable mandibular defect.6,7 Malignant variants of ameloblastoma are seen in two forms:
Malignant ameloblastoma; and
Ameloblastic carcinoma.
Figure 1. Ameloblastoma of the left body of the mandible with classical multilocular cystic ‘soap bubble’ or ‘honeycomb’ appearance.
Trauma
Trauma to the head and neck region frequently results in facial bone fractures with studies showing mandibular fractures to be most prevalent.8 Major traumatic injuries to the face, eg gunshot injuries/road traffic accidents, can lead to extensive maxillofacial bone defects where restoration of function and aesthetics can only be achieved through reconstruction.
Infective/inflammatory process
‘Osteomyelitis’ (Figure 2) is defined as infection of the medullary portion of bone.9 Infection becomes established in the calcified portion of bone, compromising or obstructing blood supply to the region and leading to ischaemia. Following ischaemia, the infected bone becomes necrotic and leads to sequestrum formation. The pathogenesis of osteomyelitis is multifactorial and some important factors include: virulence of the infecting organisms, underlying immune status of the host, and type, location, and vascularity of bone.10 In the oromaxillofacial region this is usually due to odontogenic infection, post-extraction complication or trauma and, most recently, bisphosphonate therapy.9 Treatment generally involves evaluation, staging, determination of microbial aetiology and antimicrobial therapy. Where extensive necrotic bone is present, debridement of bony sequestrae is necessary along with resection and dead-space management, usually with reconstruction.10
Figure 2. Moth-eaten appearance of bone. Areas of osteosclerosis and osteolysis with loss of definition of inferior dental canal in the LL5 and LL6 region indicative of osteomyelitis.
Osteoradionecrosis (ORN) is described as a disease process where devitalization and devascularization of bone occurs as a result of irradiation. It is a complex metabolic and tissue homeostatic deficiency which can be spontaneous, but most commonly results from tissue injury.11,12 Prophylaxis of ORN is the major goal in modern combined tumour therapy. Once ORN is established, conservative treatment modalities are used initially in an attempt to control disease progression involving curettage of necrotic bone and hyperbaric oxygen therapy. Unfortunately, radical resection of the affected bone is the only curative treatment, leading to a significant defect.
Congenital deformities
The majority of congenital deformities affecting the mandible are associated with syndromes such as Pierre-Robin syndrome and Treacher Collins syndrome. These syndromes are commonly associated with hypoplasia of the mandible and reconstructive surgery is indicated to improve aesthetics. Other features of these syndromes include cleft palate with hypoplastic air sinuses and malars. Deformed ears are characteristic features of Treacher Collins. In Pierre-Robin syndrome glossoptosis, downward displacement of the tongue, together with mandibular retrognathia, can cause airway problems.
Hemifacial microsomia is a congenital craniofacial deformity in which one side of the lower face fails to develop properly. It is characterized by malformation of the ear on the affected side and defects in the size and structure of the mandible requiring reconstruction.
Reconstruction and regeneration techniques
Any maxillofacial bone defect can have both a physiological and psychological impact on patients, affecting function and aesthetics. However, recent advances in the management of these deformities have led to a significant improvement in patients' life quality. Optimum reconstruction requires advanced techniques and the challenge is to achieve good functional and cosmetic outcomes.2
Developments in the field of regenerative medicine are relentless at present with particular focus on stem cell therapy. Stem cell research has grown exponentially and it is well recognized that cell-based therapies have the potential to improve the quality of life for patients with various diseases.13,14,15
Reconstruction
Reconstruction attempts to restore the bony contour of the maxillofacial skeleton while minimizing the aesthetic deformity. The aim is to restore mastication, swallowing and articulation ability whilst maintaining an adequate airway.16 Aesthetic deformity and functional losses depend on size and location of the segmental defect. In general, defects in the posterior body of the mandible or ramus are better tolerated. As the defect extends to involve the symphysis or anterior body of the mandible, significant deformity and loss of function occurs. Mastication and swallowing may be compromised as the structural support for the tongue and larynx is lost, whereas airway compromise due to tongue prolapse can occur and necessitate tracheostomy.17 If possible, mandibular reconstruction should not be delayed as this will lead to scarring and fibrosis of the remaining bone and soft tissue, making the reconstruction more challenging.2 The decision in relation to the best approach mainly depends on the disease process, location and anatomy of the defect.3
Reconstruction of the maxillofacial bone defects
Maxillofacial bone defects may be reconstructed using:
Bone grafts;
Alloplastic material; or
Free flaps.
Bone grafting
Embryologically, bone may be classified as intramembranous or endochondral. Intramembranous ossification occurs in the so-called membrane bones of the skull, eg frontal, parietal, temporal, occipital, maxilla, mandible and flat bones, whereas endochondral ossification is characteristic of the bones of the trunk and extremities.18 The principle of replacing like with like should generally be adhered to and therefore bone of intramembranous origin should be used to reconstruct mandibular defects. It has been reported that membranous bone grafts maintain better volume because of their larger cortical and smaller cancellous components, along with a faster revascularization process.19 Bone grafts can be of three different types:
Autogenous bone graft;
Allogenic bone graft; or
Xenograft.
Autogenous bone grafts refer to bone harvested within the same individual. This is the gold standard for reconstruction as it contains viable and immunocompatible osteoblastic cells that are needed to regenerate bone.2,17Figure 3 illustrates an autogenous ramus graft augmenting a bony defect in the maxilla.
Three types of autogenous bone graft can be harvested:
Cancellous;
Cortical; and
Corticocancellous.
Figure 3.
(a) Autogenous bone harvested from mandibular ramus. (b) Bone transferred and secured in recipient site. (c) Xenograft material placed to cover autogenous bone graft (d) Resorbable membrane overlaying surgical site. (e) Implant placed in the augmented area. (f) Healed intra-oral view.
Cancellous bone grafts contain higher quantities of viable osteoblasts than either cortical or corticocancellous grafts and therefore a higher percentage of viable cells survive during the transplantation procedure.2,17
One of the difficulties associated with autogenous bone grafts is obtaining sufficient quantities of bone for grafting, while minimizing risks during harvesting, such as donor site morbidity, inflammation and resorption of the implanted bone.2,17 Therefore, autogenous grafting is only indicated when restoring small mandibular defects.
Allografts refer to grafts harvested from another individual of the same species. The most commonly used allograft for mandible reconstruction is freeze-dried bone. In 1965, Marshall reported on the benefits of using allogenic bone grafts for osseous repairs.18 Such bone grafts are suitable for small defects where the continuity of the mandible is intact. The main drawbacks with allografts are vulnerability to infection, antigenicity and concerns with regards to potential disease transmission.17
Xenografts refer to material harvested from a different species17 and they can be used to restore small bony defects. They show a high degree of osseoconductivity and have a slow resorption profile which contributes to the stability of newly generated bone. Bio-Oss®, a bovine-derived deproteinized bone, is one such material. It has been utilized successfully for over 20 years with clinical uses in bone augmentation, sinus elevation, repair of furcation lesions and intrabony defects.20
Alloplastic materials
Several alloplastic materials are available to restore osseous defects (Table 1) with variable success rates. Such biomaterials can be broadly categorized into calcium phosphate-based ceramics and cements, synthetic polymers and, most recently, tissue-engineered bone substitutes. Hydroxyapatite (HA) is a calcium phosphate material; a major component in bone and teeth. It is available in naturally-occurring or synthetic forms. Synthetic calcium phosphate (CaP) ceramics, such as beta-tricalcium phosphate (β-TCP), are engineered to resemble that of cancellous bone and therefore used to restore cancellous defects. HA cements have been used since the early 1990s as multipurpose bone substitutes for filling calvarial defects and contouring facial skeleton abnormalities. However, they lack sufficient tensile and compressive strength and therefore cannot be used in load-bearing applications.21
Compound
Commercial Products
Hydroxyapatite
Pro-Osteon, Calcitite and coral-based products
Tricalcium phosphate
Vitoss
Hydroxyapatite cements
Norian CRS, Bone Source, Mimix Bone Void Filler
Bioactive glass
NovaBone
Porous polyethylene polymer
Medpor
Methylmethacrylate polymer
Hard tissue replacement
Bioactive glass is a synthetic, osteoconductive, silica-containing particulate bone filler that is used for restoring surgical or traumatic bone defects. It can be used in combination with autogenous bone particles and demineralized bone matrix, leading to accelerated bone healing compared with bone grafting alone.21
Medpor is a biocompatible, porous, high-density polyethylene implant material, which has been used successfully for aesthetic contour enhancement and reconstruction of the facial skeleton. It is long-lasting, with a low frequency of complications. Associated morbidity is similar to procedures involving autologous grafts, and overall patient satisfaction is high.21
Organic calcium salts and synthetic materials such as methylmethacrylate, proplast and teflon have been used with limited success. In general, alloplastic materials' lack of osteo-inductive properties and absence of vascularity and cellular components contra-indicates their use in radiated or poorly vascularized tissue.17
Vascularized free flaps
Over the past 20 years the use of vascularized bone grafts has become common practice for mandibular reconstruction, with success rates of over 90% reported. The most usual donor sites for osseous tissue transfer include the fibula, scapula, iliac crest and radius.16
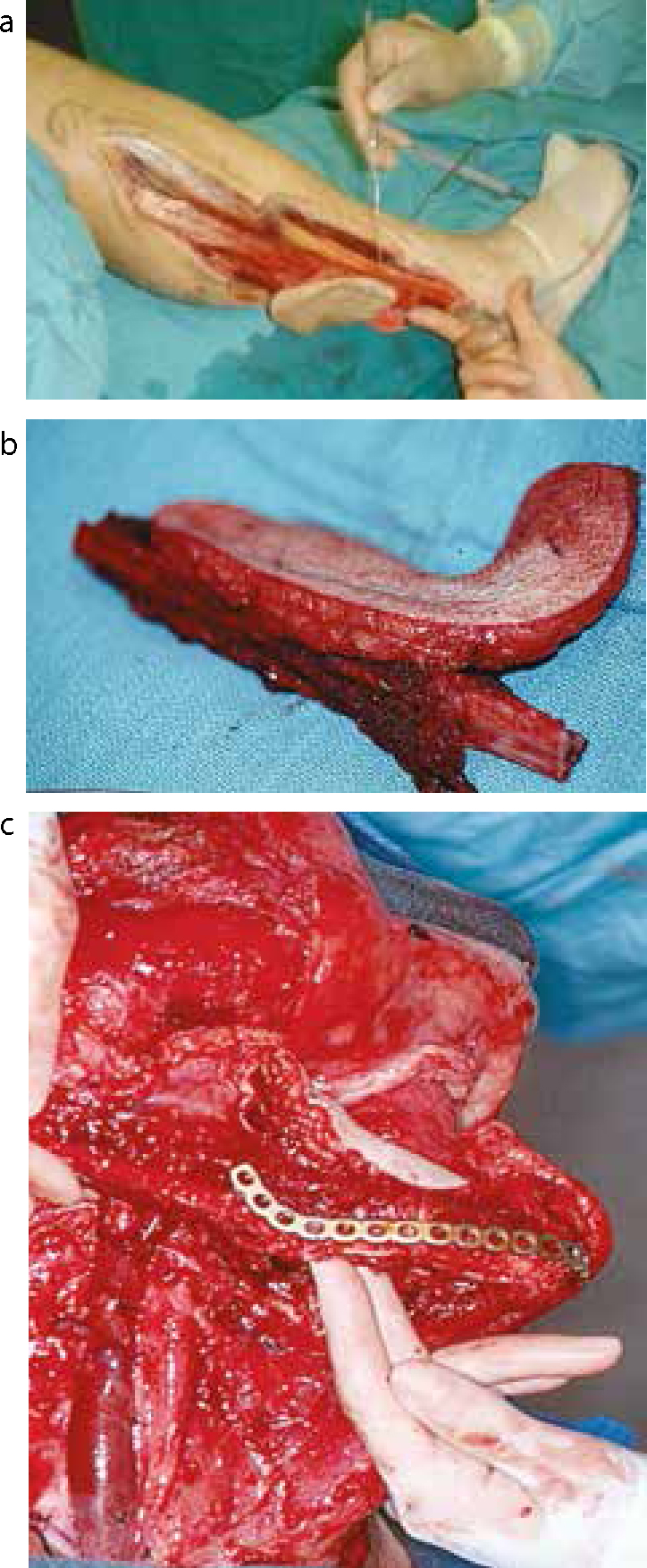
Fibula free flaps (FFF) (Figure 4) are most commonly used for mandibular reconstruction. This is an excellent choice for reconstructions that require primarily bone and in cases where the native mandible is atrophic.3 It allows for significant bone transfer (max 25 cm in length) and is thus ideal for reconstruction of large defects.2,3,17 The FFF is based on the peroneal artery and its accompanying veins. The fibula graft allows placement of osseointegrated implants to support dental prostheses and can be contoured, thereby improving aesthetics and function.22
Figure 4.
(a) Harvesting of osteocutaneous flap from right fibula. (b) Fibula osteocutaneous flap. (c) Fibula flap in situ with osteotomies and titanium reconstruction plate.
Scapular osteocutaneous free flaps are indicated where there is a full thickness defect, such as those involving facial skin, bone and mucosa.22 It is based on the circumflex scapular artery and its accompanying veins. The vascular pedicle, which is 6–9 cm, is of sufficient length to reach recipient vessels in the neck.3,17,23 Osseointegrated implants can be placed in most cases to aid with dental prostheses.22
Development of the iliac crest free flap has significantly improved the surgical restoration of the mandible. This donor site provides a long vascular pedicle, appropriately shaped bone, and is advantageous for lateral and hemimandibulectomy defects.17
Radial forearm free flaps can be successfully used to restore small mandibular defects but are not ideal for reconstruction of large defects. This is due to unacceptable donor site morbidity when harvesting a large amount of bone, including a limited range of motion, grip strength and supination.22 The length of the radius bone that can be harvested safely without unacceptable forearm dysfunction is limited to 10–12 cm with recommendations to harvest only up to 40% thickness of the circumference of the radius, to minimize the risk of subsequent pathological fractures.17 It can easily bear tissue-borne prosthesis and, in fact, provides a better contour for support of tissue-borne prosthesis than either the fibula or scapular composite free flaps.22
Total replacement of the TMJ has been performed in the UK since 1987 and approximately 60–65 are performed annually. Indications for TMJ replacement include relief of severe arthritis pain, ankylosis, avascular necrosis, benign or malignant neoplasms and degenerative joints with severe anatomical discrepancies. The key efficacy outcomes of TMJ surgery are pain relief, correction in bite, improved mouth opening and ability to eat a more normal diet.24 Three prosthetic systems currently exist which differ in their component material and are illustrated in Table 2.25,26
Regenerative medicine involves the creation of functional tissues to replace damaged or malfunctioning tissues and organs. Tissues and cells may be generated from a patient's own cells, thus minimizing or eliminating the risk of rejection. Furthermore, it has the potential to obviate organ transplant.14
Currently, the following bone regenerative techniques are employed:
Guided bone regeneration;
Distraction osteogenesis;
Bone morphogenetic proteins.
Guided bone regeneration (GBR)
Guided bone regeneration encourages bone growth in the site of a defect. GBR protects the defect against population by epithelial and connective tissue to allow the space to be inhabited by bone cells that grow into the area of the defect. The available preclinical and clinical evidence suggests that GBR continues to be a successful adjunct in peri-implant bone defects and preservation of alveolar bone following extraction of teeth.14
Over the past number of years, non-immunogenic and resorbable biomaterials are becoming the basis for complete and predictable guided bone regeneration in many cases. GBR, using expanded polytetrafluoroethylene (e-PTFE) membranes has become an accepted method for promoting bone growth adjacent to oral implants.27Bio-Gide®, a porcine resorbable bilayer collagen membrane is currently used in periodontal, peri-implant applications or to improve the ossification of bone defects of any origin. It consists of a smooth and a rough surface. The smooth surface is covered by a particularly dense film, designed to prevent the invasion of soft tissue in a membrane-protected bone defect and the rough side is designed to promote bone ingrowth.28
Distraction osteogenesis (DO)
The discovery of DO was made by a Russian orthopaedic surgeon, Professor Gavriil Ilizarov in 1954 when, by chance, he observed callus formation in a patient who mistakenly distracted his frame instead of compressing it.29
Distraction osteogenesis is a technique to lengthen bones without the use of grafting material (Figure 5). This technique can be particularly useful for congenital deformities of the mandible.30 It is the process of new bone generation through the gradual separation of segments of existing bone.2 An average growth of 10 mm in bone height is reported with DO when used to reconstruct the mandible.22 The advantages and disadvantages of DO are outlined in Table 3.
Figure 5. Distraction osteogenesis device: (a) lateral cephalometric radiograph at pre-activation stage; (b) orthopantomogram near end of treatment and (c) posterior-anterior view showing final position of the mandible. Radiographs are courtesy of Mr Duncan Campbell, Consultant in Oral and Maxillofacial surgery.
Advantages
Disadvantages
Less extensive than conventional surgery
Greater probability of bone stability post-surgery
Need for bone graft or internal fixation is obviated
Maximum distraction 40 mm
Decreased bone density in the area
Risk of TMJ ankylosis
Technique-sensitive and equipment-sensitive surgery
Need for second surgery to remove distraction device
Patient compliance
Bone morphogenetic proteins (BMPs)
BMPs are multi-functional growth factors belonging to the transforming growth factor beta (TGFβ) superfamily.31 Extraction, purification and cloning of the protein morphogens has led to therapeutic strategies for regeneration of human bone.2,22 Recombinant human bone morphogenic protein-2 (rhBMP-2) and -7 (rhBMP-7) are used for spine and long bone non-union, as an alternative to autologous bone grafts. In the head and neck region, this concept is applied in alveolar regeneration and in sinus floor procedures. Regeneration of 6 cm segmental bony defects in the mandible have recently been reported.32
Cell based therapy for bone regeneration
Stem cells
Stem cells are unique cells found in multi-cellular organisms and they have the following specific features:
Ability to differentiate into one or more specialized cell types (multi-lineage differentiation).13
There are two different types of stem cell:
Embryonic; and
Adult-derived.
Embryonic stem cells (ESCs) are derived from embryos. They can differentiate into over 200 different cell types found in the body and renew almost any tissue and are therefore classified as pluripotent stem cells. Adult stem cells (ASCs), also known as somatic stem cells, are usually found in a specific tissue or organ in the body and they have limited differentiation capacity. Their main function is to maintain and repair tissue in which they are found and therefore are regarded as multipotent cells.13 ASCs can be harvested from many organs and tissues as demonstrated in Table 4.
Bone Marrow
Skin
Lung
Skeletal Muscle
Retinal Tissue
Dentinal Epithelium
Adipose Tissue
Neural Tissue
Blood Vessels
Heart
Gut
Brain
Liver
Ovarian Epithelium
Testes
Dental Tissues
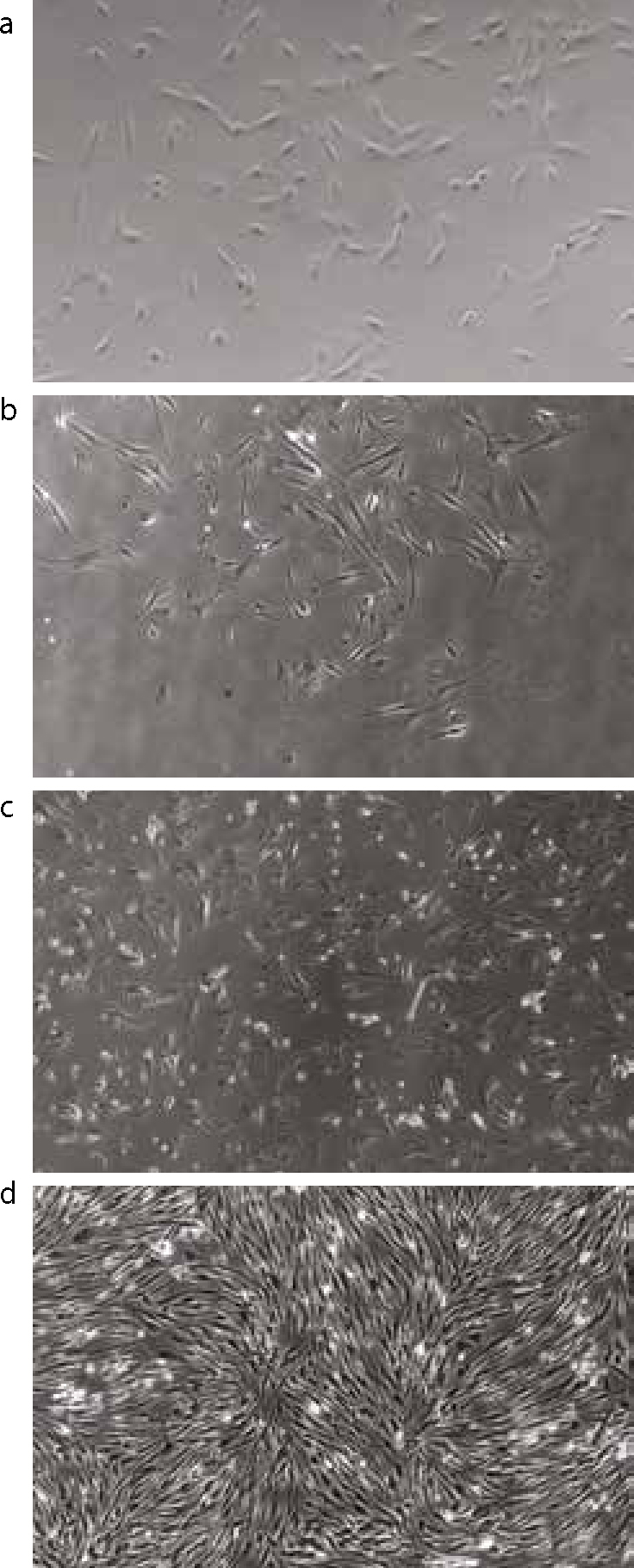
Contentious issues surrounding the use of ESCs, including development and subsequent destruction of embryos, forced scientists to seek other methods of culturing stem cells. This led to the innovation of induced pluripotent stem cells, whereby ASCs are reprogrammed to behave like ESCs and have the potential to develop into any cell type. This new technique could exclude the possible problems associated with immune rejection, ethical obstacles and issues with tumorigenicity.13 Dental pulp stem cells (Figure 6) represent an adult stem cell population that is readily accessible from extracted teeth.33 There are recent reports on the successful induction of pluripotency in cells of dental pulp origin.
Figure 6. Microscopic 4x view of undifferentiated mesenchymal stem cells harvested from the pulp of adult caries-free wisdom teeth. (a–d) The progressive growth in dental pulp stem cells population with 6D showing confluence of the cells. The photographs were taken at the Scottish Centre for Regenerative Medicine.
Current clinical uses of stem cells
Stem cells have been used for decades in transplantation therapy and it is now a common practice for the treatment of bone marrow failure and haematological malignancies. Their uses may be considered in categories as shown in Table 5.
Non-malignant Disorders: bone marrow failure, haemoglobinopathies, immune deficiencies, inherited diseases of metabolism, autoimmune disorders
Currently, experimental animal studies have shown that stem cells harvested from pig's deciduous teeth can regenerate bone in critical size mandibular defects.34 Researchers in Italy demonstrated the use of dental pulp stem/progenitor cells and scaffolds in repairing maxillofacial bony defects.35 Furthermore, animal studies demonstrated that rat mesenchymal stem cells encapsulated in a biocompatible polymer were able to form a human-shaped mandibular condyle.36 This approach, once refined, could be used as the ultimate therapeutic application in patients requiring temporomandibular joint replacement.
Future uses of stem cells
Work is ongoing in tissue engineering in an attempt to devise solutions to the highly personal needs of specific patients in keeping with the long tradition of surgical innovation. In the future, medical researchers anticipate being able to use technologies derived from stem cell research to treat a wider variety of diseases including cancer, Parkinson's disease, ischaemic heart disease, liver disease, diabetes mellitus and connective tissue disorders.13 Progressive research involving stem cell and tissue engineering may lead to the development of new less invasive techniques to repair maxillofacial bony defects.
Conclusion
The field of maxillofacial bone reconstruction has witnessed tremendous advances in recent years. This has led to current state of the art reconstructive techniques, with vascularized osseous free tissue transfer being the preferred reconstructive modality for larger defects. Surgeons need to be familiar with numerous alternatives to choose the most appropriate procedure on an individual basis. The future seems to lie in the field of regenerative medicine and with the further refinement of techniques in stem cell research and tissue engineering; bone regeneration may be the next step in management of maxillofacial bone defects.