Consultant Dermatological Surgeon, NHS Lothian and Hon Senior Lecturer, University of Edinburgh, Dermatology, Room 4.018, Lauriston Building, Lauriston Place, Edinburgh, EH3 9HA, UK
Skin cancer is the commonest malignancy in most European populations, and is highly treatable. The highest density of tumours is on the face, ears and – if the patient is bald – the scalp. There are two main varieties of skin cancer with very different consequences: melanoma is uncommon but has a significant case-fatality of ~20%, whereas keratinocyte tumours, such as basal cell carcinoma and squamous cell carcinoma, are more common, but have a much better prognosis than melanoma. Diagnosis of skin cancer relies on clinical suspicion and the ability to distinguish the morphologies typical of cancer from the far larger number of benign mimics of skin cancer. Clinical suspicion is paramount in achieving early diagnosis.
Clinical Relevance: Dentists, although their principal activities are confined to the mouth, should be in a position to recognize suspicious skin lesions on the face and other exposed surfaces.
Article
Jonathan L Rees Lisa Naysmith
When to make a diagnosis?
Most dermatological diagnoses, just like most dental ones, are not fatal and, in general, treatment for skin disease is symptomatic, and based on the ‘here and now’. Unlike much of the work of the modern general medical practitioner, dermatologists are usually concerned with resolving conditions that patients deem important, because they are symptomatic, rather than attempting to prevent some future serious event in a patient who is currently asymptomatic (such as a stroke in somebody who is hypertensive). It follows, that if you as a dentist notice that a patient has a skin disorder, say bad dandruff (essentially a variant of seborrhoeic dermatitis, an inflammatory response to a yeast infection), then the decision to point this out to the patient is perhaps best made on the basis of what you know about the patient already — do you really think they want this issue raising or not? You may reasonably choose to stay quiet.
There are, however, two major exceptions to the above course of action. The first, concerns rashes such as lupus erythematosus, or the bullous disorders that may also involve the oral mucosa (eg pemphigus or pemphigoid), where treatment is necessary, not just for symptomatic relief, but in order to prevent the development of scarring or other damaging sequelae. In these instances, the case for early diagnosis is compelling.
The second, and largest group, however, is that of skin cancer. In this latter scenario, early diagnosis is important because it is associated with a better prognosis and, in the case of a melanoma, early diagnosis may be life saving. This article focuses on this latter group. Dentists are frequently in a good position to diagnose common skin cancers, and to advise patients on the need to seek further care.
In what follows, we describe the main types of skin cancer, summarize what we know about their causes, and provide a (very) brief overview of treatment. We then go on to describe the clinical appearance of many of the most common cancers that may be seen on the head or neck, along with some of the main clinical mimics of the more common skin cancers. Finally, we provide pointers to openly available websites that provide more information if you remain curious to know more.
The classification of skin cancer
There are two main types of skin cancer:
Melanoma, a highly malignant tumour of melanocytes (Figure 1); and
Non-melanoma skin cancer (NMSC), a term which encompasses basal cell carcinomas (BCC) (Figure 2) and squamous cell carcinomas of the skin (SCC) (Figure 3), both of which are keratinocyte-derived malignant tumours.
Figure 1. A malignant melanoma arising on the cheek. Note the lighter brown area and the much darker black area that has probably arisen from it. The lesion is just palpable.Figure 2. A classic nodulocystic basal cell carcinoma on the middle third of the face. There is central ulceration, a pearly edge and telangiectasia.Figure 3. A squamous cell carcinoma on the face presenting as a nodule 2.0 cm across. Note the surrounding sun damage, and the keratotic centre.
This binary divide is useful. NMSC is much more common than melanoma, but the case-fatality is much lower. By contrast, melanoma is perhaps 10–20 times less common than NMSC but kills more people. As a rough guide, around 1% of the UK population will develop a melanoma sometime in their life, whilst around 20% will develop a NMSC. Of those who develop a melanoma, around 20% will die from it, whilst for NMSC fatalities are rare (<0.5% of cases). Many lay people do not appreciate the important differences in prognosis between NMSC and melanoma and, when obtaining a history, a family or personal history of NMSC is often incorrectly described as a history of melanoma. Similarly, because a harmless mole was removed, patients sometimes believe it meant they have had skin cancer.
Causes of skin cancer
The main risk factors for skin cancer are the level of skin pigmentation, exposure to ultraviolet radiation (UVR), and age. Melanin protects against the harmful mutagenic effects of UVR. In those with very dark skin, skin cancer is rare, and the degree of UVR exposure almost irrelevant. By contrast, those with pale skin are at greatly increased risk of skin cancer and, even within European populations, variation in skin colour is an important determinant of risk. Thus the individual with bright red hair who is unable to tan, and covered in freckles (a marker of both exposure and genetic risk) is more at risk of skin cancer by a factor of up to five than his/her darker haired, olive skinned counterpart (Figure 4).
Figure 4. Freckles are a marker of both sun exposure and genetic susceptibility to skin cancer. The darker central lesion is not a melanoma but a blue nevus (see text).
In those with pale skin, sun exposure is a major determinant of risk. So, skin cancer rates are highest in those living closer to the equator and in those who spend more time outdoors, whether occupationally or as part of leisure activities. An extreme example would be some Australian populations, where up to 1:30 of the adult population develops a new skin cancer each year. Rates in the UK are 20–50 times lower. As with most human malignancies, the rates of all types of skin cancer rise dramatically with age.
Numerically much less important, at least at the population level, but which confer very high risks at the individual level, are the dramatically increased rates of NMSC seen in patients receiving immunosuppressive therapies after organ transplant, and a rare autosomal dominant inherited disorder, Gorlin's syndrome, which is associated with multiple basal cell carcinomas and odontogenic keratocysts, as well as a range of other phenotypic abnormalities.
The two main types of NMSC
The two commonest types of NMSC are basal cell carcinomas (BCCs) (Figure 2) and squamous cell carcinomas (SCCs) (Figure 3). Both these tumour types are derived from keratinocytes and both are common on the face. They are both malignant – that is the cells invade deeper structures – but they differ dramatically in their ability to metastasize. Although rare instances (<1:4000) of metastasis from a BCC are recorded – usually in large lesions in people who have neglected them – in practice they are managed as though they do not metastasize. Note that this does not imply that they do not present a serious risk to the patient. BCCs are, by definition, a cancer and are capable of invasion of underlying structures, such as muscle and bone, and can track along nerves from the skin intracranially. Overall mortality from a BCC is incredibly low, however, and, in general, the main therapeutic challenge is how to remove or destroy the tumour in a way that, whilst effective, causes minimal functional and cosmetic impairment.
SCCs, by contrast, as well as being invasive, are capable of metastasis. In up to 5% of many case series, SCCs metastasize to regional lymph nodes or elsewhere, and fatalities occur in up to 3% of cases. (There are a number of prognostic factors that help predict high risk clinical behaviour.) One confusion relating to terminology relates to the phrase ‘head and neck SCC’. This term should exclude all primary skin SCCs and refer only to lesions that arise from the various mucosae: the mouth, pharynx, larynx, etc. All such tumours have a worse prognosis than cutaneous SCCs. Similarly, SCCs of the lip have a worse prognosis than those of the fully keratinized skin.
There are two precursor lesions of skin SCCs (BCCs have no known precursors), actinic keratoses (Figure 5), and Bowen's disease (BD) (intra-epidermal carcinoma) (Figure 6). Both of these are characterized by focal areas of dysplasia but where the basement membrane has not been breached by the clones of aberrant cells. Like NMSC in general they are markers of high sun exposure. Both actinic keratosis and Bowen's disease can progress to SCC, but the rate of progression is low: for actinic keratosis a rate of 1:1000 per lesion per year, and for BD up to 10% over a period of time have been quoted. The authors' view is that these figures should be treated with considerable scepticism because, not surprisingly, we simply do not have robust long-term observational studies of progression. In everyday clinical practice, once either of these lesions is diagnosed, they are usually treated.
Figure 5. A typical actinic keratosis on the tip of the nose. Actinic keratoses can vary in size from 1mm to up to 1cm or more. They feel rough, and small ones are sometimes better felt than seen.Figure 6. A small plaque of Bowen's disease. They sometimes resemble a plaque of psoriasis or eczema.
Melanoma
Melanomas are malignant tumours of melanocytes (Figure 1). Sometimes people use the term malignant melanoma instead of just melanoma, but there is no such entity as a benign melanoma, so the term melanoma, by definition, means a malignant melanoma. Like NMSC, melanomas are most common in those with pale skin and high sun exposure. A minority of melanomas appear to develop from benign nevi (‘moles’), themselves clusters of melanocytes in the epidermis or dermis. The clinical story is often of a longstanding stable mole that has undergone change by either growing in size or changing colour.
Treatment of primary skin cancer
The mainstay of treatment of all types of skin cancers, that is melanoma, SCC and BCC, is excision.1,2,3,4 This is usually performed in an outpatient setting under local anaesthetic with follow-up protocols dependent on tumour characteristics and patient preferences.
Suspected melanomas are initially excised with a 2 mm clinical margin and cuff of fat for histological confirmation of the diagnosis. The Breslow thickness, a powerful prognostic indicator, is measured histologically as the distance from the superficial epidermis to the bottom of the tumour lesion. If the Breslow thickness is <1 mm, 5-year survival rates are in excess of 90%; if the Breslow thickness is ≥4 mm, 5-year survival rates drop to around 50% or lower. The Breslow thickness is also used to guide further clinical wide local excision margins, which are performed to reduce the risk of local recurrence. If the Breslow thickess is <1 mm, then 1 cm wide local excision margins to fascia are carried out. If the Breslow thickness is ≥1 mm, then 2cm wide local excision margins to fascia are used, taking into account functional and aesthetic constraints.1 (Other considersations at this stage include whether to recommend sentinel lymph node biopsy for primary melanomas with a worse prognosis, a topic on which there is no consensus.)
Surgical excision is the treatment of choice for the majority of cutaneous SCC. This allows characterization of the tumour histologically and examination of tissue margins to ensure complete removal. The surgical excision margins range between 4 mm and 6 mm or greater. A 4 mm margin, used for small, well-defined tumours at low risk of metastasis, is expected to remove all the tumour completely in 95% of cases. Wider margins of 6 mm, or more, are used for high risk tumours. High risk factors include the following clinical features:
Immunosuppression, particularly organ transplant recipients;
Size greater than 2 cm;
Sites such as the ear or lip; and
Histopathological features including: thickness greater than 6 mm, perineural invasion and poor differentiation.2
In a minority of instances, some BCCs may be treated using cryotherapy, or surgical curettage and cautery, or even with topical agents such as five fluorouracil or imiquimod. In general, clinical opinion has increasingly moved towards excision as the preferred treatment for the majority of BCCs on the head, rather than curettage and cautery or cryotherapy.3 For the premalignant lesions, such as actinic keratoses or Bowen's disease, curettage and cautery, cryotherapy, or drug treatment with topical cytotoxics or immune response modifiers (imiquimod) are usually preferred over excision.5 More details about treatment can be found at www.skincancer909.com
The clinical approach
Knowledge of the biology and epidemiology of the various skin cancers is of limited use for diagnosis. Most dermatological diagnosis is non-analytical and often relies on tacit knowledge, rather than the application of explicit rules that can be applied by the novice. The expert clinician may arrive at the correct diagnosis in a flash, but explaining how he is able to make a particular diagnosis is often an exercise in wishful thinking (or self-delusion).
The difficulty for the novice is also that even a very simple classification of tumour types into, for example, melanoma and NMSC, as outlined above, is of limited use. Some NMSCs are heavily pigmented whereas some melanomas, tumours of pigment cells (melanocytes), may be lacking in melanin pigment. If this did not make the task difficult enough, malignant lesions of skin are greatly outnumbered by benign lesions, lesions that are almost ubiquitous, and most of which increase with age (as do skin cancers). This is a long way of saying that diagnostic algorithms have a very limited role, and the basis for most clinical diagnosis in this clinical area is the ability to classify lesions based on their resemblance to reference lesions in books or prior clinical experience. This is one branch of clinical practice that remains refreshingly dependent on clinical skills, and exposure to patients. In what follows we describe some of the main skin cancers and non-malignant lesions that may be confused with them. More details can be found at www.skincancer909.com
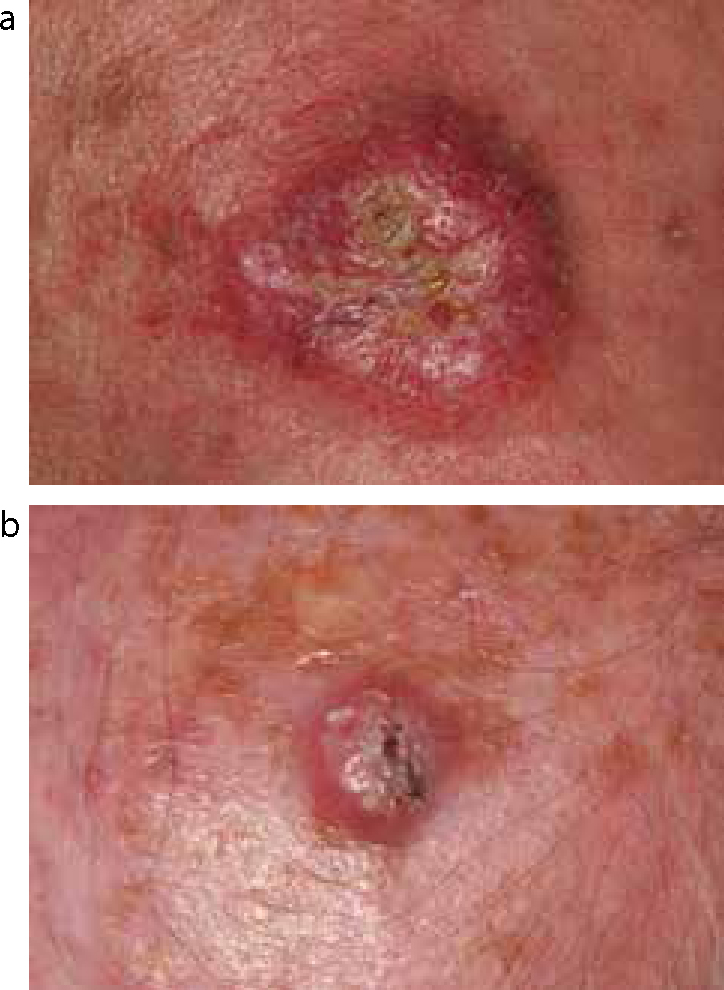
Basal cell carcinomas are the most common skin cancer. These are most common on the middle third of the face and often present as skin-coloured papules or nodules with a central area of ulceration, a pearly edge and telangiectasia. The appearance of some BCCs is much more subtle, and they extend several centimetres beyond what you first think is the margin of the lesion.
Figure 7.
(a, b) Two typical nodulocystic basal cell carcinomas on the head. Note the ulceration, the telangiectasia and the translucent colour.
Most common in those with a history of high cumulative sun exposure, these tumours are common on the pate of bald-headed men, the ears, the face and the backs of the hands. They often have a keratotic centre or even a volcano-like profile, and seem to have a reaction of repugnance amongst lay people. A keratoacanthoma (KA) is a fast growing lesion that clinically often resembles a true SCC but, by definition, involutes of its own accord leaving a scar. In practice, even when the lesion is suspected, the apparent KA is excised for fear of missing a fast-growing SCC.
Figure 8.
(a, b) Two squamous cell carcinomas. Note the surrounding sun damage with dyspigmentation (b), and the presence of keratin in the tumours.
Actinic keratoses and Bowen's disease (Figures 5, 6, 9, 10)
Like SCCs, these are related to cumulative sun exposure, and are most common at sites that have received the most sunshine. They can vary from lesions that are so small that they are often easier to feel than see, through to lesions 1 cm in diameter with a hard hyperkeratotic scale. The main differential is from seborrhoeic keratoses and small SCCs. They are frequently multiple and it is not unusual to be able to count at least 10 actinic keratoses in people with extensive sun exposure. Bowen's disease can be viewed as a lesion somewhere further on the line of tumour progression from actinic keratosis to SCC. The lesions show more dysplasia histologically, and are often larger plaques measuring up to several centres in diameter.
Figure 9. Multiple actinic keratoses on the scalp.Figure 10. A plaque of Bowen's disease behind the ear. Any induration or nodule (not present) would raise the possibility of progression to a SCC.
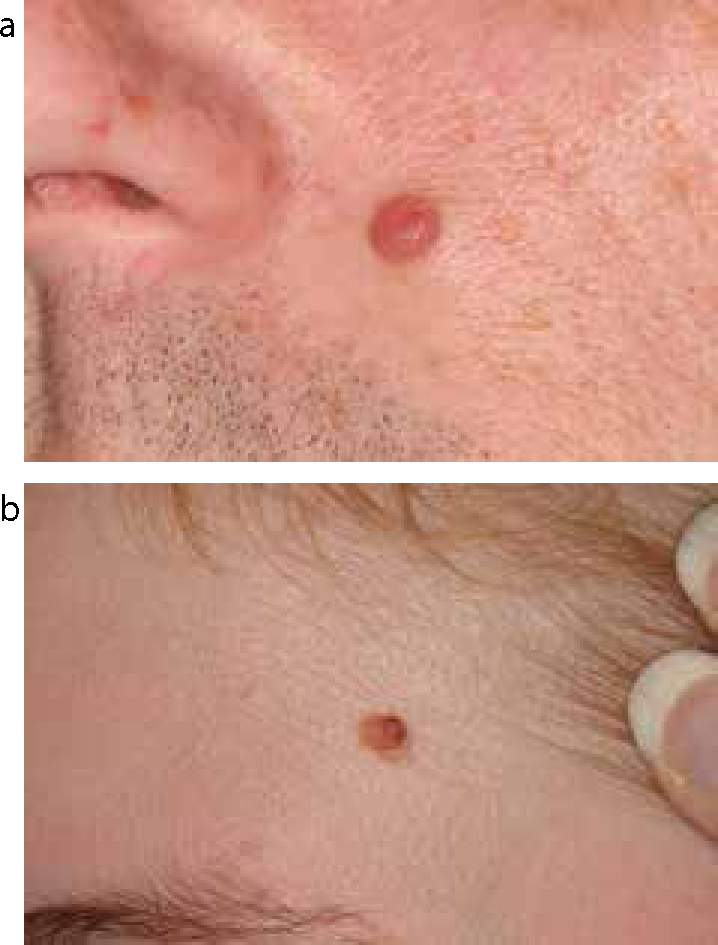
These are, of course, ubiquitous, and generally harmless. They represent clusters of melanocytes at the dermo-epidermal junction, or melanocytes that have migrated down into the dermis. Their clinical appearance varies from small, flat macules through to large, skin-coloured nodules. Melanocytic nevi change with age, appearing in childhood, and often growing in early adulthood before, on occasions, losing their pigment and ending up as skin-coloured nodules in later life. A significant proportion of melanomas arise in pre-existing melanocytic nevi.
Figure 11.
(a, b) Not all melanocytic nevi show excess melanin pigmentation. Whilst often flat and darker in earlier life, they may become more nodular and skin coloured in middle age.
Melanomas can present in a myriad of ways: dark, rapidly growing nodules (nodular melanomas) or slow-growing, pigmented macules (flat lesions) that gradually darken over years or even decades. Not all melanomas are dark; some melanomas lose most or occasionally all their pigment (‘amelanotic melanoma’). A variety of acronyms, such as ABCD, are often suggested as ways to improve diagnostic accuracy where A stands for asymmetry, B for border irregularity, C for colour variation, and D for a diameter greater than 6 mm. Despite the intuitive appeal of such mnemonics, there is little evidence to suggest that they improve diagnosis. It is probably more useful to compare what you see on a patient with a set of reference images. Beyond an individual lesion looking like a melanoma, the best predictors of a lesion being a melanoma is a history of change, and an appearance that is unlike the other melanocytic nevi on a patient (the so called ‘ugly duckling’ sign).
Figure 12. The upper and darker pigmented lesion is a melanoma. Note the variation in colour and the deep pigmentation. The other pigmented lesions are benign nevi.Figure 13. A tan area of pigmentation on the face, and a much darker area of nodular melanoma developing from the thinner lesion.
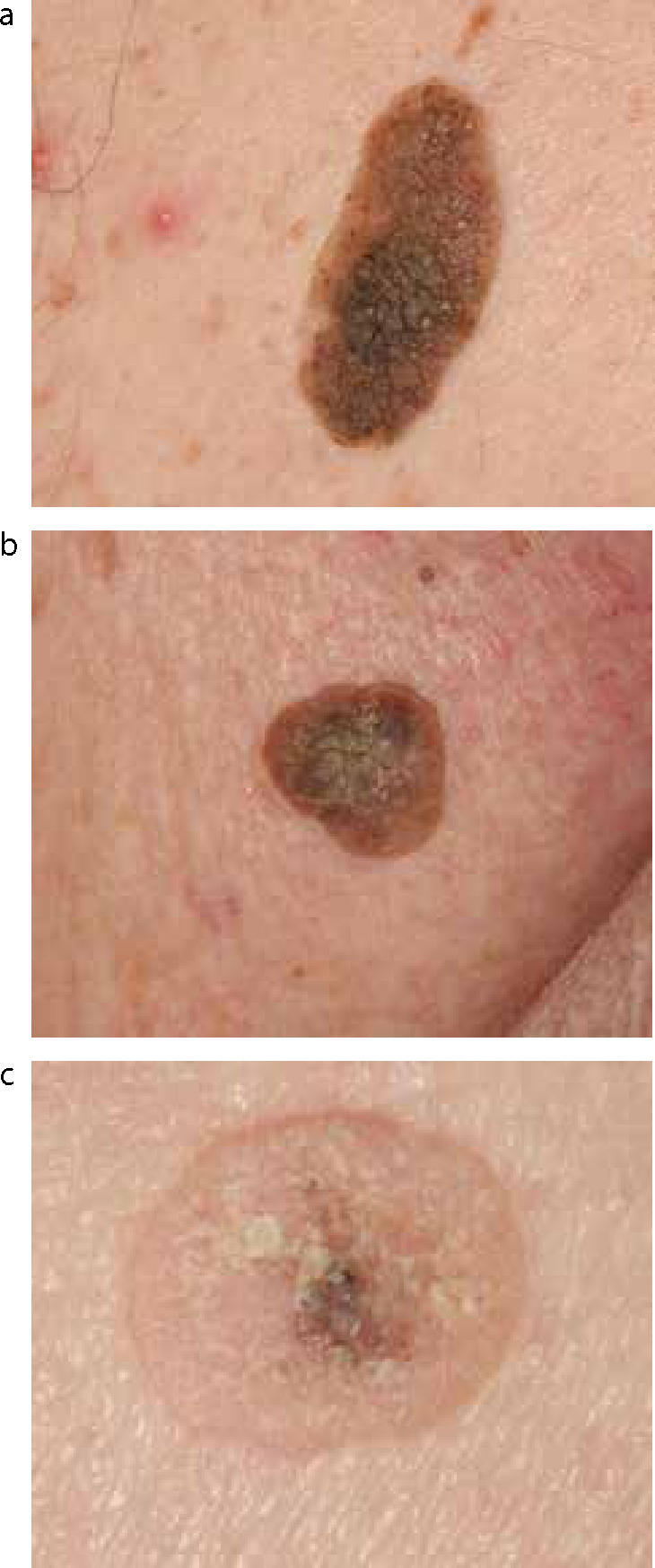
These are benign keratinocyte tumours that are the greatest mimic of melanomas (Figure 14). Most lesions referred to hospital by GPs as melanomas will turn out to be seborrhoeic keratoses. They present with a range of appearances from flat lentigo-like lesions, often referred to as solar lentigines (and by patients as liver spots) (Figure 15), through to pedunculated warty tumours measuring up to 8 cm or more. A minority resemble early melanomas, and even experts occasionally excise a seborrhoeic keratosis because of fear that they might be missing a melanoma. If you are confident of your diagnosis, most seborrhoeic keratoses can be treated with cryotherapy or curettage and cautery.
Figure 14.
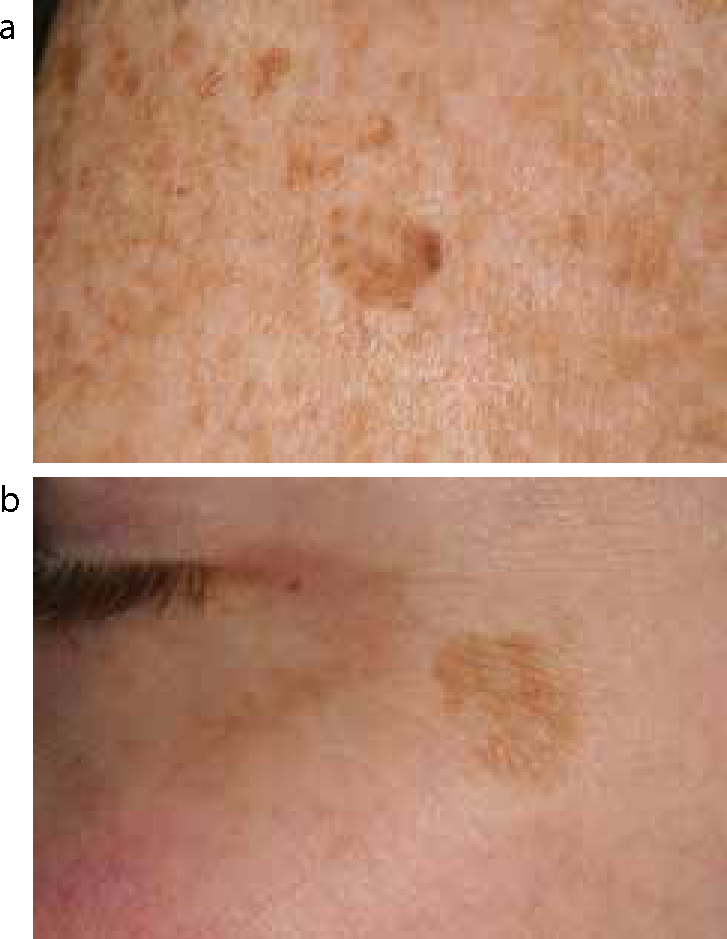
(a–c) Three examples of seborrhoeic keratoses. Seborrhoeic keratoses have a myriad of appearances. Note the warty surface in (b), the apparent crusting in (c) and the range of colours between the examples. All of these lesions are easily palpable.Figure 15.
(a, b) These lesions, usually referred to as ‘liver spots’ by patients, are often called solar lentigines, but in many ways they are just flat seborrhoeic keratoses (yes, dermatological terminology is confusing!). They are a marker of solar exposure, and most common on the backs of the hands, face and arms. The differential is usually with a melanoma.
These lesions are usually multiple, most common on the cheeks and forehead, and comprise enlarged clusters of sebaceous glands. They are easily confused with small BCCs, although they tend to look more yellow than BCCs. They do not require treatment.
Figure 16. Sebaceous hyperplasia. There is one large lesion centrally, and smaller one above. They are harmless, but often confused with BCCs.
These may of course not present any difficulty for the dentist, but are commonly misdiagnosed as BCCs by general medical practitioners.
Figure 17. Dental sinus. GPs do not tend to look in the mouth. This lesion was referred as a skin cancer, but the clinical signs are not right for this, and an oral examination confirmed the root of the problem.
Figure 18. These multiple areas of pigmentation are melanotic mucosal macules. The multitude of lesions argues against any concern re melanoma.
These are focal areas seen on the lips (and genitalia) with hyperpigmentation of the basal layer, that are frequently multiple. They are commonly confused with melanomas, but can usually be distinguished clinically.
Figure 19. Blue nevus (see also Figure 4). Admittedly, this picture does not capture the ‘blueness’ well. Blue nevi occur at all ages but if they are recent in origin, the differential is a nodular melanoma.
These can be viewed as a type of melanocytic nevus, that is situated deep in the skin, meaning that the ‘brown’ melanin pigment appears blue, due to light-scattering (the same physics that explains why the sky is blue rather than white). Their main differential is a nodular melanoma. If the lesion is recent in onset, and solitary, and the patient old, distinguishing this benign lesion from a nodular melanoma may be impossible clinically.
Figure 20. Pyogenic granuloma. These are most common on the hands and around the mouth. They look as if they bleed easily, and indeed they do! Curettage and cautery usually suffices therapeutically. The differential diagnosis is with an amelanotic melanoma.
These are comprised of granulation tissue, and are thought to be an aberrant response to wounding, and are common around the mouth and the hands. They sometimes resemble a piece of raw liver or redcurrant jam. They easily bleed on pressure. The differential is an amelanotic melanoma. If there is diagnostic doubt, they should be excised; therapeutically, curettage and cautery usually suffices.
Conclusion
Diagnosing skin cancer is a signal to noise problem – the number of benign mimics of skin cancer greatly outweighs the number of cancers, even though skin cancer is the most common cancer in most European populations. Diagnosis relies on recognizing morphological patterns, with a role for biopsy and histopathology in a small proportion of instances. The range of appearances even within a particular lesion type is large, making the field difficult for generalists. Nevertheless, even short exposure to tuition, or image banks can greatly increase the expertise of relative novices. Early diagnosis, particularly of pigmented lesions, dramatically improves prognosis, and since the highest density of cancers is on the face and head, dentists are in a good position to advise and counsel patients.