Ruigómez A, Johansson S, Wallander MA, Rodríguez LA Incidence of chronic atrial fibrillation in general practice and its treatment pattern. J Clin Epidemiol. 2002; 55:(4)358-363
Kannel WB, Wolf PA, Benjamin EJ, Levy D Prevalence, incidence, prognosis, and predisposing conditions for atrial fibrillation: population-based estimates. Am J Cardiol. 1998; 82:(8A)2N-9N
Keeling D, Baglin T, Tait C, Watson H, Perry D, Baglin C Guidelines on oral anticoagulation with warfarin. Br J Haematol. 2011; 154:(3)311-324
Fitzmaurice DA, Murray ET, McCahon D, Holder R, Raftery JP, Hussain S Self management of oral anticoagulation: randomised trial. Br Med J. 2005; 331:(7524)
Camm AJ, Lip GY, De Caterina R, Savelieva I, Star D, Hohnloser SH 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: an update of the 2010 ESC Guidelines for the management of atrial fibrillation. ▪ Developed with the special contribution of the European Heart Rhythm Association.2012
TA249 Dabigatran etexilate for the prevention of stroke and systemic embolism in atrial fibrillation. http://guidance.nice.org.uk/ta249
Stangier J Clinical pharmacokinetics and pharmacodynamics of the oral direct thrombin inhibitor dabigatran etexilate. Clin Pharmacokinet. 2008; 47:(5)285-295
Uchino K, Hernandez AV Dabigatran association with higher risk of acute coronary events: meta-analysis of noninferiority randomized controlled trials. Arch Intern Med. 2012; 172:(5)397-402
Legrand M, Mateo J, Aribaud A, Ginisty S, Eftekhari P, Huy PT The use of dabigatran in elderly patients. Arch Intern Med. 2011; 171:(14)1285-1286
TA256 Rivaroxaban for the Prevention of Stroke and Systemic Embolism in People with Atrial Fibrillation. http://guidance.nice.org.uk/TA256
Garcia D, Libby E, Crowther MA The new oral anticoagulants. Blood. 2010; 115:(1)15-20
TA275 Apixaban for Preventing Stroke and Systemic Embolism in People with Nonvalvular Atrial Fibrillation. http://guidance.nice.org.uk/TA275
Raghavan N, Frost CE, Yu Z, He K, Zhang H, Humphreys WG Apixaban metabolism and pharmacokinetics after oral administration to humans. Drug Metab Dispos. 2009; 37:(1)74-81
van Ryn J, Litzenburger T, Waterman A, Canada K, Hauel N, Sarko C Dabigatran anticoagulant activity is neutralized by an antibody selective to dabigatran in in vitro and in vivo models. J Am Coll Cardiol. 2011; 57
Baglin T, Keeling D, Kitchen S Effects on routine coagulation screens and assessment of anticoagulant intensity in patients taking oral dabigatran or rivaroxaban: Guidance from the British Committee for Standards in Haematology. Br J Haematol. 2012; 159:(4)427-429 https://doi.org/10.1111/bjh.12052
As dental professionals, we should all be familiar with the most common oral anticoagulant, warfarin, and how to manage our patients that are taking it. However, several new oral anticoagulants which have recently been approved by the National Institute for Health and Care Excellence (NICE) are now being prescribed for patients in the United Kingdom. These new oral anticoagulants fall into two different categories: a direct thrombin inhibitor dabigatran etexilate (Pradaxa® Boehringer-Ingelheim, Bracknell, Berkshire) and activated Factor X inhibitors rivaroxaban (Xarelto® Bayer HealthCare, Newbury, Berkshire) and apixaban (Eliquis® Bristol-Myers Squibb, Uxbridge, Middlesex). These new drugs will have potential consequences for how dental practitioners manage patients requiring dental treatment, especially extractions and minor surgical procedures.
Clinical Relevance: It is important that dentists are aware of new anticoagulants which are being prescribed for patients to ensure that they receive safe and appropriate dental treatment. As healthcare professionals we should also be aware of how and when to report adverse drug reactions.
Article
Atrial fibrillation is the most common sustained cardiac arrhythmia in Europe and North America with about 46,000 new cases diagnosed in the UK every year.1 The prevalence of atrial fibrillation increases with advancing age, with a 0.5% incidence in 50–59 year-olds increasing to 9% in 80–89 year-olds.2 Given that the proportion of older people in the UK population is increasing, it is likely that the prevalence of this condition will increase significantly in the next 50 years, inevitably leading to more patients being prescribed anticoagulant drugs. This same group of older people are retaining their natural teeth longer and will potentially require extractions and minor oral surgical procedures, and so dental practitioners will need to be aware of the implications of these drugs.
For the last 50 years, warfarin has been the drug of choice for oral anticoagulation in atrial fibrillation3 and it is estimated that about 950,000 people are taking the drug in the UK.4 However, newer oral anticoagulants, such as dabigatran etexilate (Pradaxa®), rivaroxaban (Xarelto®) and apixaban (Eliquis®) may now offer an alternative to warfarin. The European Society of Cardiology has updated its Guidelines for the Management of Atrial Fibrillation5 to include these drugs and the NICE Clinical Guideline 36, ‘The Management of Atrial Fibrillation,’ is in the process of being updated taking these new oral anticoagulants into consideration. This update is due for publication in June 2014.
Dabigatran etexilate (Pradaxa®)
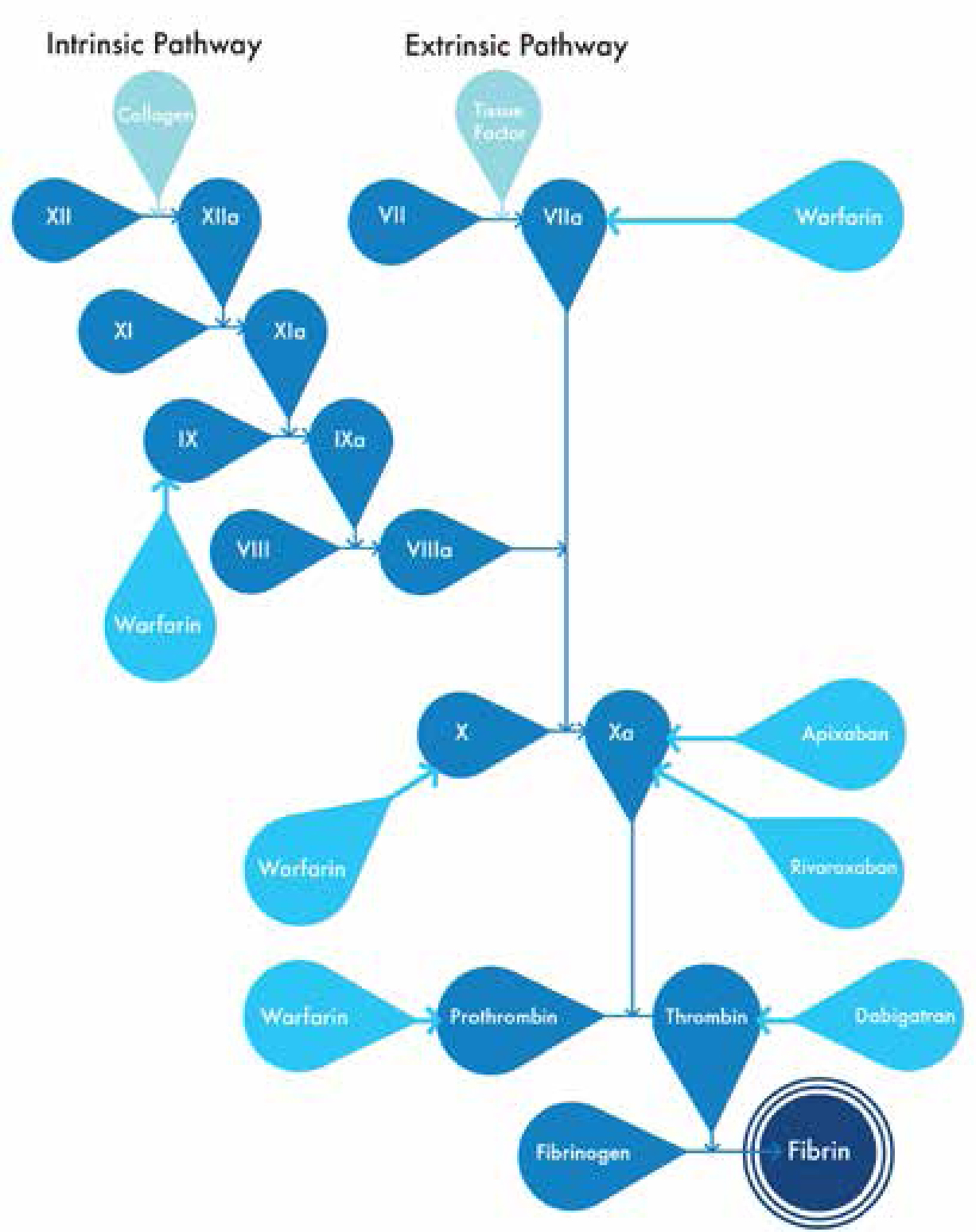
The publication by NICE of the Technology Appraisal 249 in March 20126 recommended dabigatran etexilate as a treatment option for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation and one or more associated risk factors, eg age 75 years or older, previous stroke, transient ischaemic attack or systemic embolism, symptomatic heart failure or 65 years old with diabetes mellitus, coronary artery disease or hypertension. Dabigatran etexilate is a pro-drug which is hydrolysed to the biologically active dabigatran. It is a direct thrombin inhibitor which binds to thrombin and directly blocks interactions with its substrates, therefore preventing the conversion of fibrinogen to fibrin (Figure 1). Dabigatran etexilate has a half-life of 12–17 hours before excretion, predominantly by the kidneys.7 The standard recommended dose in patients with atrial fibrillation is 150mg taken twice daily. Dabigatran etexilate has, so far, several known drug–drug interactions (Table 1) and no known drug–food interactions8 and provides predictable anticoagulation with no requirement for regular coagulation monitoring. However, the approval of dabigatran for use in atrial fibrillation is not without some controversy as there is no long-term data available for the drug and more interactions and adverse drug reactions may be identified as the drug is prescribed more widely. Dabigatran etexilate has also been linked with an increase in the incidence of myocardial infarction9 and a risk of overdose in people with impaired renal excretion.10
Figure 1. Clotting cascade.
Contra-indicated drugs:
Dabigatran etexilate
Rivaroxaban
Apixaban
Other anticoagulants
Other anticoagulants
Other anticoagulants
Azole antimycotics
Azole antimycotics
Azole antimycotics
Cyclosporin
HIV protease inhibitors
HIV protease inhibitors
Tacrolimus
Dronedarone
Anticoagulant effect increased with the following drugs:
Dabigatran etexilate
Rivaroxaban
Apixaban
Aspirin
Aspirin
Aspirin
NSAIDs
NSAIDs
NSAIDs
Clopidogrel
Clopidogrel
Clopidogrel
SSRI/SNRI
Dronedarone
Verapamil
Quinidine
Clarithromycin
Amiodarone
Ticagrelor
Anticoagulant effect decreased with the following drugs:
Dabigatran etexilate
Rivaroxaban
Apixaban
Phenytoin
Phenytoin
Phenytoin
Carbamazepine
Carbamazepine
Carbamazepine
Rifampicin
Rifampicin
Rifampicin
St John's Wort
St John's Wort
St John's Wort
Phenobarbital
Phenobarbital
Rivaroxaban (Xarelto®)
In May 2012, NICE published Technology Appraisal 25611 which recommended Rivaroxaban as a treatment option for the prevention of stroke and systemic embolism in adult patients with non-valvular atrial fibrillation and at least one other risk factor, eg age 75 years or older, congestive heart failure, hypertension, diabetes mellitus, prior stroke or transient ischaemic attack.
Rivaroxaban is a direct inhibitor of activated Factor X by reversibly binding to the active site of Factor X and preventing the catalysis of prothrombin to thrombin (Figure 1). The standard recommended dose for patients with atrial fibrillation is one 20mg tablet taken once daily. Rivaroxaban has a half-life of 5–9 hours in adults but this is prolonged to 12–13 hours in patients over 75 years old.12 Similarly to dabigatran etexilate, rivaroxaban has several known drug-drug interactions (Table 1) and no known drug-food interactions.13 This, combined with the once daily dosing, means that it may be an attractive treatment option for patients with atrial fibrillation. However, the lack of any long-term data is again problematic, with new interactions and adverse drug reactions possible in the future. There is also a risk of overdose in people with severe renal impairment and so caution is required with these patients.
Apixaban (Eliquis®)
Apixaban, like rivaroxaban, is an oral direct inhibitor of activated Factor X (Figure 1). In February 2013, NICE published Technology Appraisal TA27514 which recommended the use of apixaban for the prevention of stroke and systemic embolism in patients with non-valvular atrial fibrillation and one or more risk factors, eg prior stroke or transient ischaemic attack, age 75 years or older, hypertension, diabetes mellitus or symptomatic heart failure. The standard recommended dose for patients with a trial fibrillation is one 5 mg tablet taken twice daily. Orally administered apixaban has a mean half-life of 12 hours and is metabolized in the kidneys, liver and intestine.15 Apixaban has several known drug-drug interactions (Table 1) and no known drug-food interactions16 and, like the other new oral anticoagulants, routine monitoring is not required. However, again, no long-term data is available, especially with regard to drug interactions and adverse drug reactions. Caution is also advised in patients with severe hepatic or renal impairment.
Relevance for dental professionals
Of particular relevance to dental professionals is the fact that, although reversal agents are being developed,17 no antidote or reversal agents are currently available for these drugs and regular monitoring of coagulation does not take place. When faced with a patient requiring an extraction or surgical procedure, there are no specific evidence-based guidelines available to dentists to advise them as to how to proceed. Studies have also shown no definitive agreement on what laboratory blood test is most suitable for assessing the patient's level of coagulation18 and a simple INR measurement, with which we are all familiar, does not give an accurate indication of the patient's degree of anticoagulation.
The manufacturers of these new anticoagulants have not issued any specific guidance for patients who require dental extractions or dental surgical procedures. A Prescriber Guide for apixaban (Eliquis®) published by Bristol-Myers Squibb and Pfizer19 advises that, for invasive surgical procedures in general, where bleeding risk is minimal, in a non-critical location or easily controlled by mechanical haemostasis, the drug should be stopped 24 hours before the procedure. If bleeding is likely to be more significant, then the drug should be stopped 48 hours before the procedure. The Prescriber Guide issued by Bayer HealthCare20 advises a similar procedure for rivaroxaban (Xarelto®); when an invasive procedure is planned, the drug should be stopped 24 hours beforehand. Both drugs should be restarted as soon as possible after adequate haemostasis has been achieved. These prescriber guides, however, also advise that the decision on whether to stop the drugs to carry out a surgical procedure should be taken on a case-by-case basis, taking the risk of bleeding and systemic embolism into account.
Boehringer Ingelheim, the manufacturer of Pradaxa® (dabigatran etexilate) advises that, for a minor surgical procedure in patients with renal function of greater than 80 ml/min creatinine clearance, the drug should be stopped for 24 hours before surgery.21 This time will need to be extended to 1–2 days for patients with creatinine clearance of between 50–80 ml/min and extended again to 2–3 days for patients with creatinine clearance of between 30–50 ml/min. Again, the drug should be restarted as soon as adequate haemostasis has been achieved. They also advise that the decision to stop the drug to perform an elective surgical procedure should again be taken on a case-by-case basis considering the risk of bleeding in conjunction with the risk of systemic embolism.
Practical dental advice for dabigatran etexilate (Pradaxa®) has been published by the Thrombosis Guidelines Group.22 This group, however, are Belgian-based and the guidelines are not UK guidelines. This document advises that dental surgical procedures should be carried out 12 hours after the last dosing of dabigatran and should be completed with minimal trauma and post–operative suturing. It is also recommended to prescribe 5% tranexamic acid mouthwash to use 4 times a day for 5 days after surgery. This advice, however, poses some difficulties for general dental practitioners as tranexamic acid mouthwash is not on the Dental Practitioners' Formulary and is difficult to source in community pharmacies.
NICE Clinical Knowledge Summaries23 have also issued recommendations for the management of patients taking a new oral anticoagulant who require invasive procedures. They advise that the decision to stop the anticoagulant temporarily should be considered relative to the bleeding risk of the procedure and the risk of a thrombo-embolic event occurring. In this guidance, extraction of up to 3 teeth, periodontal surgery and implant placement are all classified under ‘no clinically important bleeding risk’ and the guidance for management of these patients is similar for all three of the new oral anticoagulants. For procedures with ‘no clinical important bleeding risk’, the procedure should be carried out just before the next dose of the drug is due or 18-24 hours after the last dose (this may mean missing a dose of dabigatran (Pradaxa®) or apixaban (Eliquis®) due to their twice daily dosing). The drugs should be restarted 6 hours after the procedure. The guidance also recommends 5% tranexamic acid mouthwash to be used four times a day for 5 days post-operatively which, as mentioned before, may present a significant problem for general dental practitioners.
In addition to the difficulties that dentists will face when treating patients taking these drugs, it is important that dentists are also vigilant for any adverse drug reactions associated with these new anticoagulants. The Medicines and Healthcare Products Regulatory Agency (MHRA) encourage healthcare professionals and patients to report any suspected side-effect to medicines via the Yellow Card Scheme,24 which is run in conjunction with the Commission on Human Medicines. Adverse drug reactions can be reported via the paper Yellow Card form found in the BNF (British National Formulary) or on their website at www.yellowcard.mhra.gov.uk. Information gathered from Yellow Card reports is investigated in order to identify any new side-effects or complications associated with this medicine.
Conclusion
In summary, these new oral anticoagulants may provide a viable alternative to warfarin and therefore become more widely prescribed for the treatment of atrial fibrillation. Until good quality research is conducted and evidence-based guidelines are published for dentists treating these patients, the onus is on each individual practitioner to recognize these drugs, the potential complications that may occur, report any adverse reactions and exercise caution when carrying out extractions or surgical procedures on these patients (Table 2).
What Can Dentists Do?
Be aware that there are new oral anticoagulants available for the prevention of stroke and systemic embolism in patients with atrial fibrillation.
Recognize the medicines by both their brand name and generic name.
Consider the potential for drug interaction when prescribing for patients taking these anticoagulants.
Refer to their pharmacist for advice about over the counter analgesics.
Liaise with the medical practitioner who manages the patients anticoagulation if planning any dental procedures where bleeding may occur. If dabigatran is to be stopped, the renal function must be established.
Report any adverse drug reactions via the Yellow Card Scheme.