Eccles JD. Tooth surface loss from abrasion, attrition and erosion. Dent Update. 1982; 9:373-381
Burke FM, McKenna G. Toothwear and the older patient. Dent Update. 2011; 38:165-168
Summary Report and Thematic Series (NS).: The Health and Social Care Information Centre; 2009
Kelly M, Steel J, White D Adult Dental Health Survey – Oral Health in the United Kingdom 1998.: A publication of the Government Statistical Service; 2000
Nunn J, Morris J, Pine C, Pitts NB, Bradnock G, Steele J. The condition of teeth in the UK in 1998 and implications for the future. Br Dent J. 2000; 189:(12)639-644
Sjögren U, Hägglund B, Sundqvist G, Wing K. Factors affecting the long-term results of endodontic treatment. J Endod. 1990; 16:498-504
Ng YL, Mann V, Rahbaran S, Lewsey J, Gulabivala K. Outcome of primary root canal treatment: systematic review of the literature – Part 1. Effects of study characteristics on probability of success. Int Endod J. 2007; 40:921-939
Ng YL, Mann V, Gulabivala K. A prospective study of the factors affecting outcomes of nonsurgical root canal treatment: Part 1: periapical health. Int Endod J. 2011; 44:583-609
Grieve AR, McAndrew R. A radiographic study of post-retained crowns in patients attending a dental hospital. Br Dent J. 1993; 174:197-201
Qualtrough JE, Whitworth JM, Dummer PMH. Preclinical endodontology: an international comparison. Int Endod J. 1999; 32:406-414
Jenkins SM, Haye S, Dummer PMH. A study of endodontic treatment carried out in dental practice within the UK. Int Endod J. 2001; 34:16-22
Goodacre CJ. Designing tooth preparations for optimal success. Dent Clin N Am. 2004; 48:359-385
Hemmings KW, King PA, Setchell DJ. Resistance to torsional forces of various post and core designs. J Pros Dent. 1991; 66:325-329
Poyser N, Briggs PFA, Chana HS, Kelleher MGD, Porter RWJ, Patel MM. The evaluation of direct composite restorations for the worn mandibular anterior dentition – clinical performance and patient satisfaction. J Oral Rehab. 2007; 34:(5)361-376
Chana H, Kelleher M, Briggs P, Hooper R. Clinical evaluation of resin-bonded gold alloy veneers. J Prosthet Dent. 2000; 83:294-300
Alani A, Bishop K. Contemporary issues in the provision of restorative dentistry. Br Dent J. 2012; 213:(4)163-170
Gulamali AB, Hemmings KW, Tredwin CJ, Petrie A. Survival analysis of composite Dahl restorations provided to manage localised anterior tooth wear (ten year follow-up) 2011. Br Dent J. 2011; E9
Alani A, Bishop K, Djemal S. The influence of specialty training, experience, discussion and reflection on decision making in modern restorative treatment planning. Br Dent J. 2011; 210:(4)
Balto HAG, Al-Madi EM. A comparison of retreatment decisions among general dental practitioners and endodontists. J Dent Educ. 2004; 68:872-879
Cosyn J, De Bruyn H. Interclinician disparity in periodontal decision making: need for consensus statements on surgical treatment. J Periodont Res. 2007; 42:311-317
Ibbetson RJ, Hemmings KW, Ward VJ. Variations in planning fixed bridgework – a group of dentists at a case-based postgraduate course. Br Dent J. 1999; 187:159-163
Maidment Y, Durey K, Ibbetson R. Decisions about restorative dental treatment among dentists attending a postgraduate continuing professional development course. Br Dent J. 2010; 209:455-445
Pagonis TC, Fong CD, Gunnar Hasselgren G. Retreatment decisions – a comparison between general practitioners and endodontic postgraduates. J Endod. 2000; 26:240-241
Zadik Y, Levin L. Clinical decision making in restorative dentistry, endodontics, and antibiotic prescription. J Dent Educ. 2008; 72:81-86
Berry DC, Poole DFG. Attrition: possible mechanisms of compensation. J Oral Rehab. 1976; 3:201-206
Posselt U. Studies in the mobility of the human mandible. Acta Odont Scand. 1952; 10
Pameijer JHN, Parkins BJ.Amsterdam: Dental Center for Postgraduate Courses; 1985
Dawson PE.St Louis, Missouri: Mosby; 2007
Christensen J. Effect of occlusion-raising procedures on the chewing system. Dent Pract Dent Rec. 1970; 20:233-238
Dahl BL, Krogstad O, Karlsen K. An alternative treatment of cases with advanced localised attrition. J Oral Rehab. 1975; 2:209-214
Lindauer SJ, Gay T, Rendell J. Effect of jaw opening on masticatory muscle EMG-force characteristics. J Dent Restor. 1993; 72:51-55
Dahl BL, Krogstad O. The effect of a partial bite-raising splint on the occlusal face height. An X-ray cephalometric study in human adults. Acta Odont Scand. 1982; 40:17-24
Dahl BL, Krogstad O. The effect of a partial bite-raising splint on the inclination of upper and lower front teeth. Acta Odont Scand. 1983; 41:311-314
Dahl BL, Krogstad O. Long-term observations of an increased face height obtained by a combined orthodontic/prosthetic approach. J Oral Rehab. 1985; 12:173-176
Gough MB, Setchell DJ. A retrospective study of 50 treatments using an appliance to produce localised occlusal space by relative axial tooth movement. Br Dent J. 1999; 187:134-139
Hemmings KW, Darbar UR, Vaughan S. Toothwear treated with direct composite restorations at an increased vertical dimension: results at 30 months. J Prosthet Dent. 2000; 83:287-293
Redman CDJ, Hemmings KW, Good JA. The survival and clinical performance of resin-based composite restorations used to treat localised anterior toothwear. Br Dent J. 2003; 194:566-572
Satterthwaite JD. Indirect restorations on teeth with reduced crown height. Dent Update. 2006; 33:210-216
Smales RJ, Berekally TL. Long-term survival of direct and indirect restorations placed for the treatment of advanced tooth wear. Eur J Prosthodont Rest Dent. 2007; 15:2-6
Saunders WP, Saunders EM. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:137-140
Toothwear is now common, especially in younger patients, with high demand for the restoration of the damaged teeth which is likely to increase further over time. Fixed prosthodontic options range from direct composite resin to conventional tooth preparation and cemented indirect restorations. This paper summarizes the views of a variety of clinicians on a plan delivered to a patient with toothwear in secondary care and explores the possible reasons for the variation in decision-making in the treatment of toothwear.
Clinical Relevance: With levels of toothwear increasing, the clinician needs to be aware of the different treatment modalities which are appropriate.
Article
Toothwear is often defined as the chemical and/or mechanical loss of tooth surface that does not involve bacteria.1 Premature wear of the dentition is now considered pathological and preventable.2
The 2011 Adult Dental Health Survey confirmed an increased prevalence of toothwear,3,4 compared to the findings of the 1998 Adult Dental Health Survey5 (Table 1). Although only the anterior teeth were examined for wear:
77% of dentate adults had some form of toothwear;
15% had moderate toothwear (wear that has exposed a large area of dentine on any surface); and
2% had severe toothwear (wear that has exposed the pulp or secondary dentine).
Age groups
Percentage of dentate adults with:
Any wear
Some moderate wear
Some severe wear
1998
2009
1998
2009
1998
2009
All
34
77
3
15
0
2
16–24 yrs
12
52
0
4
0
0
25–34 yrs
24
69
1
7
0
0
35–44 yrs
29
77
2
10
0
0
45–54 yrs
41
84
4
16
0
2
55–64 yrs
49
89
5
20
0
3
65–74 yrs
58
92
9
29
0
4
75–84 yrs
95
44
2
6
85 yrs +
94
34
6
When the extremes of age were considered, 52% of 16–24 year-olds had some form of wear compared with 95% of 75–84 year-olds. The exact prevalence is difficult to ascertain owing to varied assessment criteria and variations between different population groups.
Variations in treatment planning for toothwear cases in the UK
The 2011 Pan Dental Conference was held in Liverpool on the 11th and 12th November 2011. The society felt that it would be appropriate to explore the differences in treatment planning for toothwear by using a case as the thread for an interactive expert panel discussion in front of an audience of conference delegates. A previously treated wear case was presented and discussed during the Interactive Treatment Planning Session as part of the ‘Are we doing the right thing?’ educational programme on the British Society of Prosthodontics (BSSPD) agenda. All identifying details of the patient were removed and both the patient and the treating clinicians gave permission to the society for the case to be used for educational purposes.
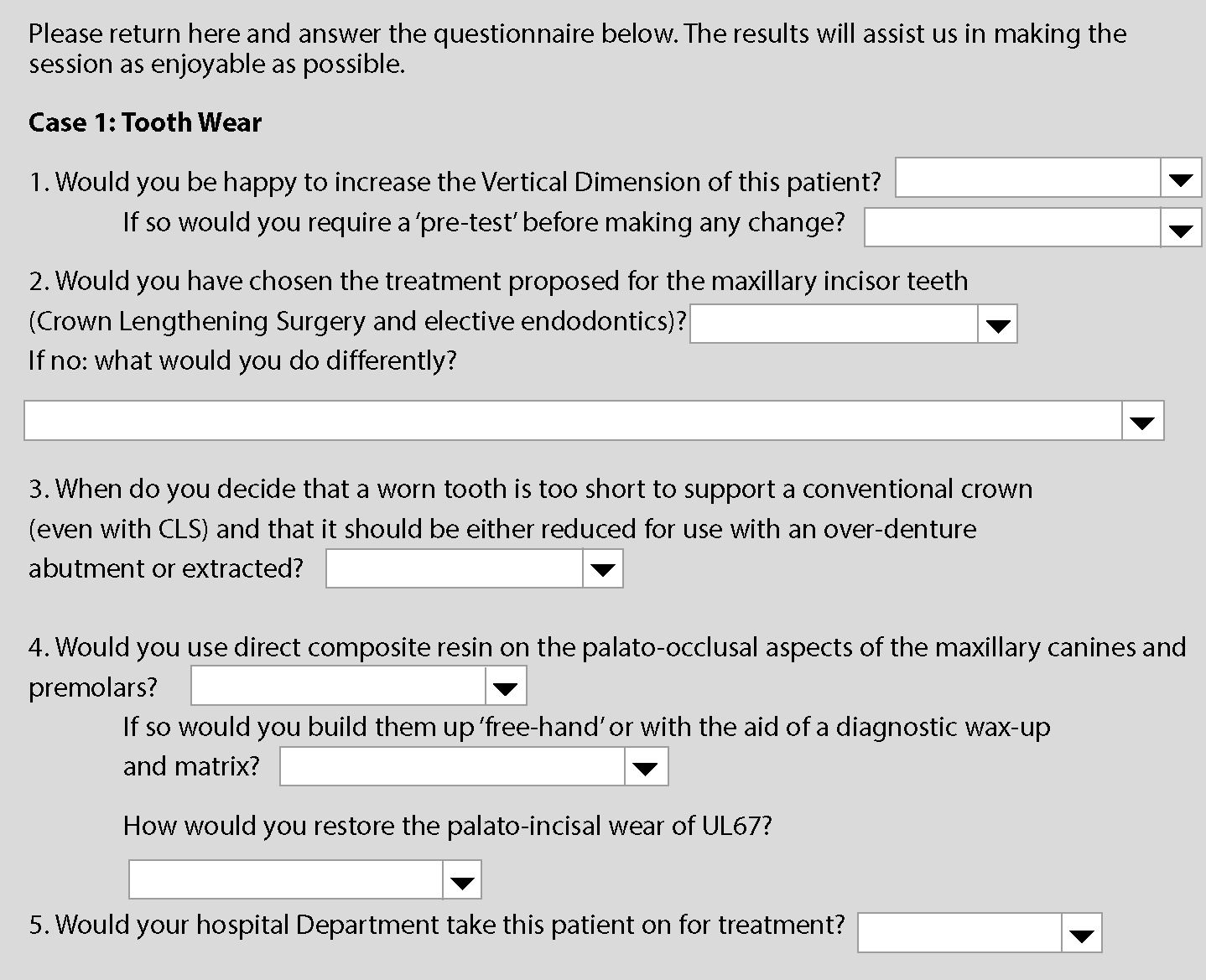
Prior to conference, the clinical details were also uploaded onto the Pan Dental Society Website (www.pandental.co.uk). The case was accompanied by a case summary together with pre-and post-treatment photographs. Five main questions were posted which people were encouraged to answer online (Table 2). Fifty-two dentists completed the web-based questionnaire (45 were hospital or other NHS salaried dentists, 3 were UK-based general dental practitioners and 4 were general dental practitioners working outside the UK). The results of each completed web-based questionnaire were emailed to one of the authors (PB) who organized the Pan Dental interactive session. These same questions were put to each of the expert panel members during the interactive session.
Question
Answers
Yes
No
Would you be happy to increase the vertical dimension of this patient?
95%
5%
If you are happy to increase the vertical dimension, would you require a ‘pre-test’ before making any change?
20%
80%
Would you have chosen the treatment proposed for the maxillary incisor teeth (crown lengthening surgery and elective endodontics)?
50%
50%
Would you use direct composite resin on the palato–occlusal aspects of the maxillary canines and premolars?
88%
12%
Would your hospital department take this patient on for treatment?
42%
58%
Peter Briggs (who collated the results of the web-based questions) chaired the well-attended session. The invited panel included six well-known UK Consultants/Specialists in the field of Prosthodontics: Derrick Setchell (London), Lloyd Searson (London), Craig Barclay (Manchester), Ken Hemmings (London), Paul King (Bristol) and Nick Lewis (London). Each panel member was asked to give his or her view and comment on the treatment that had been carried out. The discussion was also opened up to include the attending course delegates.
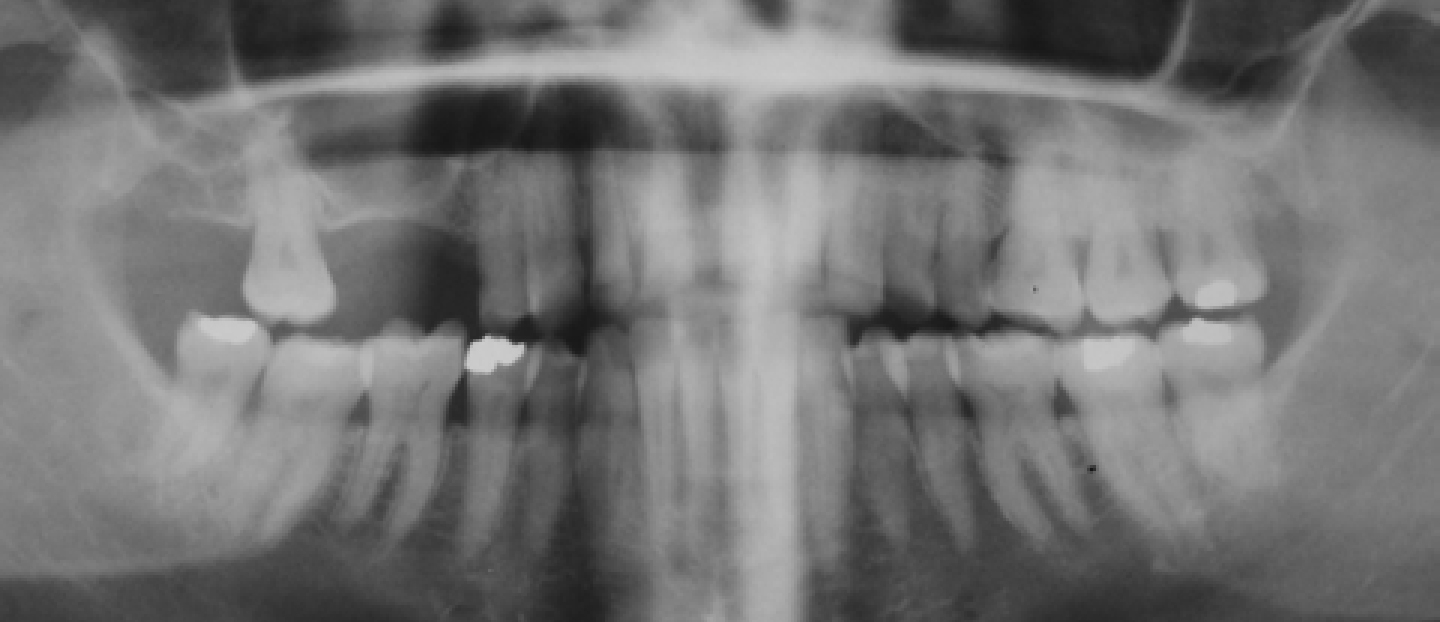
Figure 1. Extra-oral view showing the smile line.Figure 2. Labial view with teeth in occlusion.Figure 3. Maxillary occlusal view.Figure 4. Mandibular occlusal view.Figure 5. Pre-operative dental panoramic tomogram.
A 41-year-old female presented with marked erosion of the maxillary teeth with a history of mental illness that had involved vomiting and ‘picking at’ her teeth. Following a long period of treatment, the patient was in recovery and rebuilding her life. She was no longer vomiting or ‘picking at’ her teeth. Her complaints were the poor appearance of the upper anterior teeth (shape of teeth and the spacing between the teeth) and some sensitivity localized around the UL6. She was less concerned about the space left by the loss of two teeth in the upper right quadrant. She preferred not to wear a denture owing to her strong gag reflex and she was not struggling to eat on the right side.
She smoked 20 cigarettes per day and had done so for 25 years. She was a regular dental attender and her dental practitioner had referred her to a dental hospital for possible treatment. There was no evidence of periodontal pockets greater than 3 mm, although there were some areas of recession.
The expert panel members were asked to respond to pre-set questions on the management of the patient. The same questions were asked online and the results sent to PB by email. Fifty-two completed web-based questionnaires were received prior to the conference. These results were made known and discussed with the panel and the audience. They were collated and displayed in simple percentages (Table 2).
What follows is a summary of the discussion that took place on the treatment plan used to treat this wear patient from both the expert panel members and the audience of BSSPD delegates at the Pan Dental Conference in 2011.
Question 1 – Would you be happy to increase the vertical dimension of this patient? If so, would you require a ‘pre-test’ before making change?
None of the expert panel expressed worries about increasing the occlusal vertical dimension (OVD) by the space necessary for the satisfactory aesthetics of the final restorations. The increase should be dictated by a combination of the ideal post-operative tooth length required and inter-occlusal space required for the palatal contour of the teeth. There were no concerns regarding the amount by which the OVD is increased.
The panel members were generally happy to use the Dahl concept and composite to achieve this or, if indicated, the use of a diagnostic wax-up upon casts mounted on a semi-adjustable articulator to fabricate conventional provisional crown restorations. As most of the occlusal aspects of the maxillary teeth were restored in this case, the vertical dimension of the overall occlusion was increased by a combination of direct composites on UR7, UR4, UR3, UL3, UL4 and UL5, and porcelain fused to metal crowns (PFMs) on the UR2, UR1, UL1 and UL2. The shared common view was that it was unlikely that the patient would need a ‘trial’ period of adjusting to the increased vertical dimension. The panel would reserve this for patients with a history of temporo-mandibular joint or muscle problems or those with a high level of occlusal awareness.
The vast majority of the dentists that completed the questionnaire (95%) reported that they were comfortable to increase the OVD of this patient. Most (80%) would not consider a trial increase of vertical dimension necessary but 20% would want to ‘test’ a trial appliance, eg a removable occlusal splint, before making a ‘fixed’ change to overall vertical dimension.
Question 2 – Would you have chosen the treatment plan proposed for the maxillary incisors, ie crown lengthening and elective root canal therapy of UR2, UR1, UL1 and UL2? (If ‘no’ what would you do differently?) (Figures 7–13).
Figure 7. Pre-operative palato-incisal view UR3, UR2, UR1, UL1, UL2 and UL3.Figure 8. Immediately after surgical crown lengthening UR3, UR2, UR1, UL1, UL2, UL3 and UL4.Figure 9.
(a, b) Six weeks after surgical crown lengthening surgery healing.Figure 10. Preparation of UR2, UR1, UL1 and UL2 for cast gold post and cores.Figure 11. Plastic post impression posts UR2, UR1, UL1 and UL2. aFigure 12. Cemented cast post and cores UR2, UR1, UL1 and UL2.Figure 13. Post–operative views: (a) extra-oral view of porcelain-fused to metal crowns (with butt fitted labial margins) UR2, UR1, UL1 and UL2, direct composite resin free-hand build-ups UR4, UR3, UL3, UL4 and UL5; (b) labial view with teeth in occlusion; (c) palatal view.
The view from panel members was unanimous. They did not share the view that elective devitalization and root canal therapy, to allow subsequent restoration with cast posts and cores of UR2, UR1, UL1 and UL2 was necessary to restore the maxillary incisors predictably. All panel members supported the need for the crown lengthening surgery (CLS) of UR2, UR1, UL1 and UL2; followed by either conventional PFM crowns (with metal on palatal surfaces being the ideal choice) or adhesive all-ceramic dentine-bonded crowns for UR2, UR1, UL1 and UL2. They expressed that ‘in their hands’ enough retention would be achieved with this procedure without the need for post cores. Some voiced the view that the adhesive ceramic restorations were more predictable on the grounds of the likely intrinsic erosive aetiology (evidenced by the history of the patient and the fact that the mandibular dentition displayed little wear).
Most experts felt that direct composite restorations would not be very predictable for UR2, UR1, UL1 and UL2 owing to their severe wear and lack of enamel on the palatal and palato-gingival areas. However, some felt that there was little to be lost by giving direct composite ‘a go’ and that such restorations could provide the first part of a two-stage approach.
The expert panel was generally happy to suggest PFM crowns for UR2, UR1, UL1 and UL2, in combination with an increase in overall vertical dimension and with the use of palatal metal as the long-term treatment modality for this patient.
Members of the audience and the web survey results disagreed with the expert panel on this issue. Half of the dentists who completed the web-based questionnaire agreed with the treatment carried out and would both root treat and crown lengthen UR2, UR1, UL1 and UL2. A good proportion of dentists in the audience felt that adequate retention and resistance form for UR2, UR1, UL1 and UL2 (single crowns) could only be achieved by the use of both crown-lengthening in conjunction with the post and cores in this particular case. It was expressed that retention challenges are different for worn teeth supporting single crowns when compared to bridges. It was suggested by some that this is an important area for future clinical research.
This marked difference in view of the web and audience survey to the generally united view of the expert panel may be a reflection of personal differences in experience and training. Those who have worked within different UK dental hospitals will often come across with strong and, at times, inflexibly held views on treatment planning. The wise clinician will enthusiastically embrace the practice, the different philosophies available, consider the available evidence and make up his/her own mind about which works best.
In an ideal world, there was agreement that good standard elective endodontics can be expected to be successful.6,7,8 Similarly, post crowns placed within single teeth with good ferrules, when done well, will likewise be expected to last well. Unfortunately, there is UK evidence that dentists commonly experience technical problems with posts, such as iatrogenic deviation and around 50% of such teeth are associated with radiographic evidence of peri-apical periodontitis.9 There is also evidence to suggest that, in the UK, we struggle to achieve technically gold standard root fillings, even for single-rooted teeth.10,11 This may also support the general view of the panel of experts that it might be most sensible initially to avoid the additional risk to the long-term outcome of the UR2, UR1, UL1 and UL2.
Comment was also made that one could always consider the post-core option at the first failure cycle of the restorations provided with CLS alone, especially considering that the first failure cycle of post crowns is often complicated by root fracture, rendering the tooth unrestorable.
Question 3 – When do you decide that a worn tooth is too short to support a conventional crown (even with CLS) and that it should be either reduced for use with an over-denture abutment or extracted? (Figures 7 and 11).
The general view from the experts was that 3 mm of crown height (axial wall of the tooth preparation) is usually enough to retain a single crown.12 However, several commented that many worn teeth display uneven wear and that, as a result, each tooth needs to be assessed on an individual basis. The panel also commented that a short tooth in a parafunctional patient represented a greater challenge to future crown retention than a tooth damaged by erosion, highlighting the importance of accurate diagnosis prior to treatment planning.
There were marked differences in the opinions of those in the web-based survey, with 66% willing to use teeth shorter than 3 mm for the support of fixed indirect restorations. The web-based answers varied considerably: 7% of dentists indicated that anything below 5 mm would not retain a crown; 27% felt the cut-off was 3 mm; 33% felt it should be 2 mm and, surprisingly, 33% considered only heights below 1 mm as too short for a crown rather than an over-denture abutment.
The reasons for this may well relate to the fact that 50% of the surveyed dentists would also consider elective root treatment and the use of post-core restorations (in combination with crown lengthening), where a minimum cervical collar/ferrule of 2 mm is required.13 This approach may allow for very short teeth to be built up with fixed restorations, but it is likely in some patients to prove unpredictable, particularly in the presence of parafunction. With such an approach, additional tooth height is achieved from direct or indirect core material rather than from natural tooth tissue. Our discussion clearly established the need for clinical studies in this area to address the minimum height of tooth required to retain a direct and indirect restoration, especially as adhesive techniques may mean reduced need for conventional preparations aimed at increasing retention and resistance form.
Question 4 – Would you use direct composite resin on the palato–occlusal aspects of the maxillary canines and premolars? If ‘yes’ would you build them up ‘free-hand’ or with the aid of a diagnostic wax-up and matrix? (Figures 9, 10 and 12).
The general view of the panel supported the preference for the ‘free-hand’ direct composite approach to the build-up of the canine and premolar teeth. They were also keen to optimize the properties of composite by placing the restorations in some bulk, in combination with an increase in vertical dimension, as mentioned earlier and supported by the literature.14
The view was that direct composite was likely to perform well for these teeth owing to the presence of enamel and their moderate, rather than severe, level of wear. The personal choice of most panel members was free-hand application, with the added benefit of avoiding unnecessary resource allocation/making a cost saving. It was felt that familiarity with laboratory-based procedures during training makes clinicians more comfortable with building things up free-hand. There was some comment that present dental training involves less exposure to laboratory skills.
Only 35% of the web-respondents agreed with the panel's view and were happy to apply the composite by hand, with the majority (65%) preferring the use of a pre-formed matrix constructed from a pre-op wax-up. Some audience members made a valid point; a pre-formed matrix allows for a more convenient method of forming the palatal/lingual shapes of toothwear build-ups with direct composite resin and hence more careful control of the desired occlusal scheme.
Question 5 – How would you restore the palato-incisal wear of UL6 and UL7? (Figure 3)
In this case, the UL6 and UL7 were not restored as the use of fluoride applications and better oral hygiene improved the symptoms. The panel was split between the use of conventional and adhesive cast metal indirect restorations and composite resin.
Again, it was felt that there was little to lose (other than time and some cost) in using direct composite restorations first and then moving on to indirect restorations if they prove unpredictable. Of web-questioned dentists, 42% would use adhesive gold, 21% direct composite and 37% conventional ceramic +/- metal crowns. The panel favoured cast metal on the grounds of robustness and relatively conservative tooth preparation. Comment was made that, if PFM restorations were to be used, then metal and not ceramic should be used on the occlusal surface. There was clearly much support from both the panel of experts and the audience for adhesive cast gold to restore UL6 and UL7, with some evidence that they will improve the pulpal sensitivity present.15
Question 6 – Would your hospital department take on this patient for treatment?
This question was aimed at the dilemma of secondary care providing treatment for toothwear patients. Of the web-responders, 42% would accept (or expect acceptance) of this patient for treatment within a secondary care environment; 58% would refer back (or expect return) to the referring practitioner with a treatment plan. There was concern from the panel and audience that the NHS can no longer absorb such treatment loads, as there are other more important priorities, such as cancer, trauma, developmental disorders and severe medical compromise. In this respect, what the Restorative Dentistry Team of an acute NHS hospital trust can provide is going to be very different from a dental teaching school with greater treatment capacity by under-and postgraduate students.16
There was discussion about improving the availability of specialist prosthodontists to the NHS (within Managed Clinical Networks). It was agreed that toothwear patients are time-consuming and expensive to treat within secondary care environments. As a result, 21st century dental practitioners will need to have the skillsets to treat such patients within their practices. Toothwear and the restoration of compromised dentitions will remain a big part of UK dentistry for the foreseeable future.
The point was also made that there needs to be an incentive within any future NHS General Dental Services contract to allow such patients to be managed within primary care. For instance, a specialist in primary or secondary care could provide the crown-lengthening surgical aspect of care for this patient and the referring general dental practitioner could undertake the remainder of the treatment.
In addition, the trend is towards adhesive technology and the broad acceptance across the UK that the Dahl concept is safe and allows many wear patients to be treated in a simpler and cheaper manner.17
Discussion of decision-making in the prosthodontic management of toothwear
This BSSPD interactive session demonstrated that decision-making in the practical management of toothwear is subjective and individual. We did not attempt to explore the issue of whether or not the treatment should have been done or whether it would have been more appropriate to watch and monitor the patient (and offer further prevention and monitoring).
The decision to embark on treatment is multi-faceted. Treatment can often be patient-driven (cosmetic, functional and/or symptomatic) or clinician-driven (relieve symptoms, preventive and/or protective with a secondary intention of restoring aesthetics). The patient's perspective is extremely important as it falls upon the patient to comply with preventive measures and maintenance of restorations. Ascertaining the drive behind the patient's demand for treatment will help to understand the patient's motivation towards dental maintenance and care. Non-compliance may lead to further tooth loss and/or early failure of restorations and the patient needs to be informed of this. It could be argued that all aetiological factors should be understood and controlled before restorative intervention can be supported, however, the protection of vulnerable tooth tissue may take precedence, particularly where the toothwear has a high rate of progression and there are concerns regarding the future viability of the remaining tooth structure.
The wide variation in a clinician's decision-making was larger than expected and may be due to the variation in training, experience, and reluctance to consider newer approaches. A reluctance to use new techniques may also be due to the lack of training and practise with the new techniques and a general comfort with using techniques ‘known’ to the clinicians. In other areas of dentistry, variance in clinical decision-making is well documented, with some highlighting a lack of knowledge as a reason for the variation.18,19,20,21,22,23,24
Dento-alveolar compensation with a loss of restorative space (ie short teeth with dento-alveolar overeruption) is often seen in toothwear cases. Often, a reduction in OVD is not seen. The loss of OVD is only present if the toothwear progresses at a rate exceeding the rate of dento-alveolar growth and hence compensation.25 The OVD can potentially be ‘opened’ 20–25 mm in dentate patients, as this is the space created anteriorly when the condyles are purely rotating about the condylar axis and in centric relation.26,27,28 The stability of the lower face height is determined by the facial musculature.29,30,31 Therefore, the increase in OVD, and hence an increase in lower face height created by using the Dahl concept, is not maintained with time. Lower face height returns to that determined by the musculature following intrusion of the restored teeth and extrusion of the unrestored teeth. The panel expressed the feeling that diagnostic splints are not needed for the purpose of training a patient to tolerate an increased occlusal vertical dimension.
There was much discussion on the role and merits of traditional techniques that can be used to increase retention and resistance form. However, these methods are not a universal solution and are associated with biological costs. Partial bite raising appliances on upper teeth have been used to create localized interocclusal space by a combination of extrusion (60%) of the teeth rendered free of contact and intrusion (40%) of the teeth in contact with the ‘Dahl’ appliance.30,32,33,34 These removable ‘bite raising appliances’ were later cemented to improve compliance. They have now been replaced with composite resin restorations (considered definitive restorations in the medium term) with reasonable success rates.14,35,36,37 The teeth that are built up are unlikely to be overloaded owing to the proprioceptive feedback mechanism. The Dahl concept successfully creates space, with no pulpal symptoms, periodontal symptoms and temporomandibular joint dysfunction in the majority (96%) of cases.35,36
All experts agreed that, where possible, contemporary techniques, utilizing adhesive dentistry and the Dahl concept, have an increasing place in the management of such cases as that discussed in this paper.37,38. The recommendation of the expert panel was to carry out crown lengthening for the upper anterior teeth and provide PFMs for the upper incisors (without endodontic treatment and posts), composite build-ups for the canines and premolars and metal adhesive crowns for the UL6 and UL7, in this particular case.
The main role of additive techniques is to create time, where the dentition is satisfactorily protected and restored without the risk of destructive complications that are associated with failure of conventional restorations.39 This approach allows the lifetime of conventional restorations to start later. Furthermore, there is better protection of the pulp with more conservative approaches. It is known that 19% of teeth prepared for full crowns will develop apical areas.40 Often, the cost of repair and maintenance of these restorations, which are prone to staining, especially in smokers, is small in comparison to the biological cost of the alternatives.
The point was made that the clinicians’ confidence in these techniques grows with constant practise and experience of using these techniques. With the right clinical skills and knowledge, it is now possible to get around 7 years of survival service from direct composite Dahl restorations and around 5 years from replacement restorations that have failed.17
Conclusion
This BSSPD interactive survey highlighted differences in opinion regarding the management of toothwear around the UK. A marked difference of opinion was noted between the expert panel and those of the audience/web survey participants. Decision-making should be based on available evidence and up to date with progressive thinking. Such teaching and learning tools, exemplified by this Treatment Planning Session, as part of the educational programme organized by the BSSPD, may be the future for debating and establishing more consistency in treatment planning in restorative dentistry.