Magne P, Magne M, Belser U. Natural and restorative oral esthetics. Part II: Esthetic treatment modalities. J Esthet Dent. 1993; 5:239-246
Magne P. Megabrasion: a conservative strategy for the anterior dentition. Pract Periodont Aesthet Dent. 1997; 9:389-395
Robinson S, Nixon PJ, Gahan MJ, Chan MF. Techniques for restoring worn anterior teeth with direct composite resin. Dent Update. 2008; 35:551-558
Magne P, Holz J. Stratification of composite restorations: systematic and durable replication of natural aesthetics. Pract Periodont Aesthet Dent. 1996; 8:61-68
Nalbandian S, Millar BJ. The effect of veneers on cosmetic improvement. Br Dent J. 2009; 207:(2)
Wakiaga J, Brunton P, Silikas N, Glenny AM. Direct versus indirect veneer restorations for intrinsic dental stains. Cochrane Database Syst Rev. 2004:(1)
Felippe LA, Monteiro S, Baratieri LN, Caldeira de Andrada MA, Ritter AV. Using opaquers under direct composite resin veneers: an illustrated review of the technique. J Esthet Rest Dent: official publication of the American Academy of Esthetic Dentistry. 2003; 15:327-336
Setien VJ, Roshan S, Nelson PW. Clinical management of discolored teeth. Gen Dent. 2008; 56:294-300
Plotino G, Buono L, Grande NM, Pameijer CH, Somma F. Nonvital tooth bleaching: a review of the literature and clinical procedures. J Endod. 2008; 34:(4)394-407
Christensen GJ. What is a veneer? Resolving the confusion. J Am Dent Assoc. 2004; 135:1574-1576
Jarad FD, Griffiths CE, Jaffri M, Adeyemi AA, Youngson CC. The effect of bleaching, varying the shade or thickness of composite veneers on final colour: an in vitro study. J Dent. 2008; 36:554-559
Miyagawa Y, Powers JM, O'Brien WJ. Optical properties of direct restorative materials. J Dent Res. 1981; 60:890-894
de Azevedo Cubas GB, Camacho GB, Demarco FF, Pereira-Cenci T. The effect of luting agents and ceramic thickness on the color variation of different ceramics against a chromatic background. Eur J Dent. 2011; 5:245-252
Wray A, Welbury R. UK National Clinical Guidelines in Paediatric Dentistry: Treatment of intrinsic discoloration in permanent anterior teeth in children and adolescents. Int J Paed Dent/the British Paedodontic Society [and] the International Association of Dentistry for Children. 2001; 11:309-315
Vanoorbeek S, Vandamme K, Lijnen I, Naert I. Computer-aided designed/computer-assisted manufactured composite resin versus ceramic single-tooth restorations: a 3-year clinical study. Int J Prosthodont. 2010; 23:223-230
Yesil Duymus Z, Orbak R, Dilsiz A. Abrasion resistance of veneering materials to tooth brushing. Dent Mater J. 2003; 22:460-466
Vichi A, Ferrari M, Davidson CL. Influence of ceramic and cement thickness on the masking of various types of opaque posts. J Prosthet Dent. 2000; 83:412-417
Van Meerbeek B, Yoshihara K, Yoshida Y, Mine A, De Munck J, Van Landuyt KL. State of the art of self-etch adhesives. Dent Mat: official publication of the Academy of Dental Materials. 2011; 27:17-28
Chu FC, Andersson B, Deng FL, Chow TW. Making porcelain veneers with the Procera AllCeram system: case studies. Dent Update. 2003; 30:454-460
Antonson SA, Anusavice KJ. Contrast ratio of veneering and core ceramics as a function of thickness. Int J Prosthodont. 2001; 14:316-320
Magne P, Magne M, Belser U. The esthetic width in fixed prosthodontics. J Prosthodont. 1999; 8:106-118
Sutton AF, McCord JF. Variations in tooth preparations for resin-bonded all-ceramic crowns in general dental practice. Br Dent J. 2001; 191:(12)677-681
Peumans M, De Munck J, Fieuws S, Lambrechts P, Vanherle G, Van Meerbeek B. A prospective ten-year clinical trial of porcelain veneers. J Adhes Dent. 2004; 6:65-76
Burke FJ, Lucarotti PS. Ten-year outcome of porcelain laminate veneers placed within the general dental services in England and Wales. J Dent. 2009; 37:(1)31-38
Burke FJT, Lucarotti PSK. Re-intervention on crowns: what comes next?. J Dent. 2009; 37:25-30
Saunders WP, Saunders EM. Prevalence of periradicular periodontitis associated with crowned teeth in an adult Scottish subpopulation. Br Dent J. 1998; 185:137-140
Spear F, Holloway J. Which all-ceramic system is optimal for anterior esthetics?. J Am Dent Assoc. 2008; 139:19S-24S
Felton DA, Kanoy BE, Bayne SC, Wirthman GP. Effect of in vivo crown margin discrepancies on periodontal health. J Prosthet Dent. 1991; 65:357-364
Karaagaclioglu L, Yilmaz B. Influence of cement shade and water storage on the final color of leucite-reinforced ceramics. Oper Dent. 2008; 33:386-391
Barath VS, Faber FJ, Westland S, Niedermeier W. Spectrophotometric analysis of all-ceramic materials and their interaction with luting agents and different backgrounds. Advs Dent Res. 2003; 17:55-60
Palacios RP, Johnson GH, Phillips KM, Raigrodski AJ. Retention of zirconium oxide ceramic crowns with three types of cement. J Prosthet Dent. 2006; 96:104-114
Baldissara P, Llukacej A, Ciocca L, Valandro FL, Scotti R. Translucency of zirconia copings made with different CAD/CAM systems. J Prosthet Dent. 2010; 104:6-12
Consultant/Senior Clinical Lecturer in Restorative Dentistry, Bristol University Dental Hospital and School, University Hospitals Bristol NHS Foundation Trust, Lower Maudlin Street, Bristol BS1 2LY, UK
This is the second article of a two part series covering the aetiology, prevention and broad range of management options for the single discoloured tooth. The article covers situations where masking and simulation techniques with direct composite are required. Direct composite, indirect composite and ceramic veneers are then considered, as well as full coverage crowns. The option of extraction of the affected tooth and its prosthodontic replacement will also be considered. Clinical cases are used to illustrate various scenarios.
Clinical Relevance: The single discoloured tooth is a commonly encountered clinical problem in general dental practice. A wide variety of management options exist and it is recommended that general dental practitioners consider adopting minimally invasive techniques in the first instance before moving on to more invasive therapies.
Article
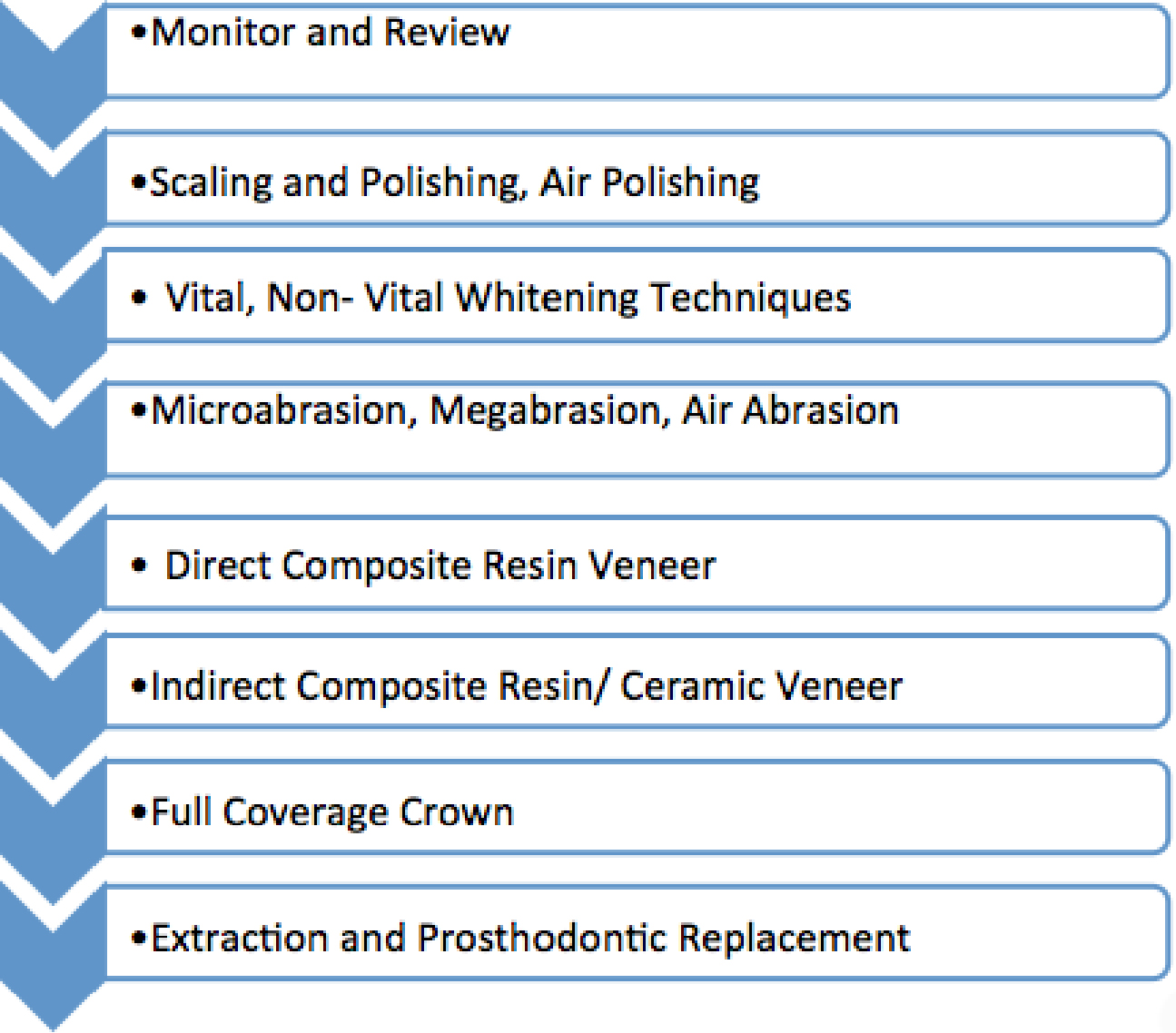
This is the second article of a two part series on management of the single discoloured tooth. It considers direct restorative options as well as indirect restorative options that involve teamwork with a suitable dental laboratory. It is assumed that the minimally invasive restorative techniques considered in part one have been exhausted, have not been successful or are judged to be unsuitable for the particular case. As described in part one, the logical approach suggested is a ‘crescendo’1 with less invasive techniques being considered first before moving towards techniques that are more destructive of tooth tissue. The overall hierarchy of treatment options is demonstrated in Figure 1. The aim of this article is to outline the final four restorative options in the hierarchy and consider their relative indications and contra-indications.
Figure 1. Hierarchy or ‘Crescendo’ of treatment options available for the single discoloured tooth.
Direct composite resin veneer
This is the direct application of a thin film of composite over the entire labial aspect of a tooth in order to modify the contour and/or shade. As for megabrasion,2 a preliminary single tooth bleaching treatment may be indicated to raise the value of the tooth shade so that a thinner layer of composite may be applied to mask the discoloration and reduce the likelihood of the tooth appearing over-contoured. For worn teeth or teeth with areas of hypoplastic or pitted discoloured enamel, the technique has the advantage of managing the deficient contours as well as the shade. It is particularly applicable for young patients with teeth which are minimally or unrestored since it preserves tooth tissue. Direct composite veneers can be placed with no or minimal tooth preparation in a single appointment, often with no local anaesthetic. The final labial contour is best placed in one increment to avoid voids3 and the interface between increments attracting stains and becoming visible. With experience and using a stratified technique4 composite veneers can be highly aesthetic. Nalbandian and Millar5 found, in a survey of patients who received maxillary anterior veneers, that the choice of material (direct composite resin versus porcelain) did not significantly affect the patient's perception of cosmetic improvement. A Cochrane review6 found that there is no reliable evidence to show a benefit of one type of veneer restoration (direct or indirect) over the other with regard to the longevity of the restoration.
There are two principal ways in which direct composite (whether used as a veneer over the entire labial surface or used selectively in isolated areas of the labial surface) can be used in managing the single discoloured tooth:
Masking; and
Simulation.
Masking
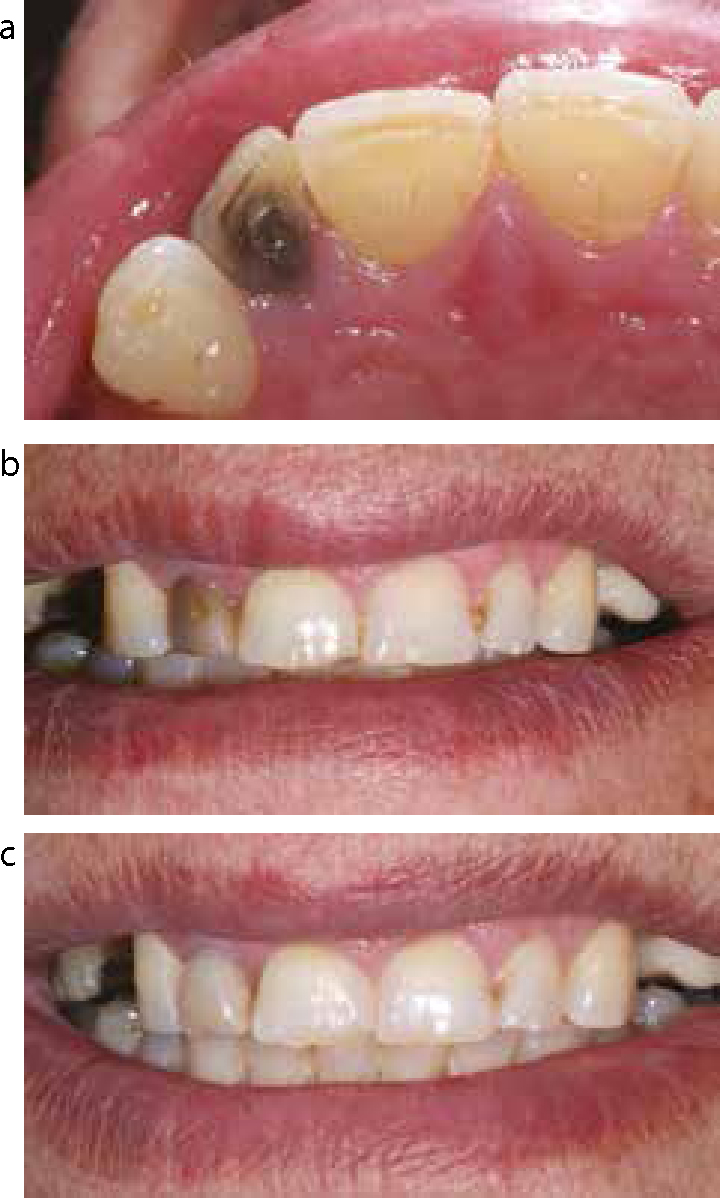
This is where one or several shades of composite resin are used to camouflage the underlying darkened tooth shade. For severe discolorations, a resin-based opaque layer placed over the discoloured areas of tooth may be required.7 This is then covered with dentine and enamel shades to match the adjacent teeth. Various stains and special effect composite shades giving fluorescence, translucency and opalescence to resin restorations provide opportunities to harmonize discoloured teeth with adjacent ones. When applying composite in the cervical region, placing a retraction cord improves the visibility and provides better isolation, making it easier to perform the procedure.8 A clinical case demonstrating masking of discoloration using a direct composite resin veneer is demonstrated in Figure 2. The upper right lateral incisor tooth was discoloured secondary to a root treatment and a corroded amalgam restoration in the palatal access cavity. The patient, over 70 years of age, declined any form of bleaching or tooth preparation and wanted a rapid solution in one visit. In any case, bleaching is known to be less effective in cases whereby the cause of discoloration is due to metallic compounds, as in the case of amalgam.9 The palatal amalgam access restoration was replaced with a high value composite shade. Owing to the severity of the discoloration, and the need for an opaque layer, as well as enamel and dentine shades, the result is slightly over contoured. Nevertheless, the patient was pleased with the simple and quick solution.
Figure 2.
(a) Palatal view of discoloured upper right lateral incisor with palatal amalgam restoration. (b) Anterior view of discoloured upper right lateral incisor. (c) View of direct composite veneer placed to mask the discoloration of the upper right lateral incisor. No tooth preparation was performed.
Figure 3 demonstrates a case of a young female patient with fluorosis and discoloration of the upper right lateral and central incisor teeth. The areas of dark discoloration were disguised with direct composite resin, including an opaque layer (masking) and some superficial opaque white flecks (simulation) to harmonize the teeth with the generalized mottled appearance.
Figure 3.
(a) Brown intrinsic staining (fluorosis) affecting the UR2 and UR1. (b) Direct composite selectively applied to the UR2 and UR1 masking the brown discoloration of fluorosis and mimicking the opaque mottling seen on the adjacent teeth.
Masking with a direct composite veneer may also prove useful in cases where a form of non-vital tooth whitening is considered desirable, however, access to the pulp chamber is unavailable owing to an existing indirect adhesive restoration such as a resin-bonded bridge or indirect palatal veneer.
Simulation
This is where one or several shades of composite resin are used to mimic the discoloration of a tooth in an adjacent tooth in order to improve overall aesthetics and symmetry. It is less commonly used since most patients wish to have the discoloration disguised (masking) rather than more areas of discoloration artificially created. Setien et al8 demonstrated a case where a patient with yellow discoloration cervically at the upper right central incisor and a midline diastema had the diastema closed and the yellow cervical discoloration mimicked in the upper left central incisor to improve the symmetry of the smile.
Indirect composite veneers
Just as direct composite veneers can be used to mask underlying tooth discoloration or simulate discoloration, indirect composite veneers can be used in a similar way. Christensen10 considered the difficulty in bonding laboratory-made, fully cured resin-based composite veneers to acid-etched tooth structure and the colour unpredictability and difficulty of colour correction at seating, as reasons for the lack of popularity of indirect composite veneers. The predictability of colour matching being the principal reason for placing the restoration, in the case of the single discoloured tooth, means that the applications for this technique are fewer than for direct composite.
The unpredictability of the colour of teeth restored with indirect composite veneers has been investigated in laboratory studies. A study by Jarad et al11 found that prior bleaching of the tooth to be veneered, and the veneer thickness, significantly affected the tooth colour, depending on the shade used. The light absorbing and internal reflecting properties of the composite alter the amount of background effect and overall shade.12 The more translucent a composite, the more effect the background (tooth) colour has. Thus, altering the absorbing and reflecting properties gives variation between shades.11 The shade, thickness and optical properties13 of the resin cement lute may also have an effect on the final colour of the veneer. With all of these variables affecting the final colour of the tooth, the result can be unpredictable. Colour matching is easier with direct composite, in so far as differing shades of composite can be trialled intra-orally on unetched enamel, cured and then removed prior to the bonding procedures in order to ensure a satisfactory colour match.
The advantages of composite veneers include the ability to be repaired intra-orally if required. Precise control of occlusal contacts, proximal contacts and surface morphology is easier with an indirect composite technique, especially if the discoloured tooth is moderately broken down, hypoplastic or microdontic.
In their clinical guideline, Wray and Welbury14 suggested the use of composite veneers to treat discoloration in children under the age of 16. The technique does potentially involve less tooth tissue removal than for ceramic veneers and the cervical contour of the veneer can be modified with direct composite as the gingival margin matures apically with growth. Other causes of localized discoloration considered to be potential indications for composite veneers include localized hypoplasia not responsive to microabrasion, discoloration due to loss of vitality not responsive to non-vital bleaching, and idiopathic hypoplasia.14
The restorative status of adjacent teeth can affect appropriate material choice. For example, if the discoloured tooth is adjacent to an acrylic or composite-based restoration, then matching the optical properties of the discoloured tooth to the adjacent tooth is easier when a composite restoration is used as opposed to a ceramic one. Figure 4 demonstrates the use of composite veneers in a patient with generalized discoloration of the teeth adjacent to an acrylic prosthesis.
Figure 4.
(a) Discoloured lower incisors in a patient with amelogenesis imperfecta. (b) Indirect composite veneers are used to mask the discoloured teeth which had been bleached already and give similar optical properties to the acrylic prosthesis replacing the lower canines.
Ceramic veneers
Ceramic veneers can be used in a similar way to indirect composite veneers to mask discoloration and create the illusion of the natural intensity of tooth shade. For mild discoloration of single teeth, they may be appropriate if bleaching procedures have proved ineffective. Nevertheless, it should be stressed that a direct composite veneer is a more conservative initial choice than an indirect veneer requiring tooth preparation.
Indications
Ceramic veneers have a higher resistance to wear15,16 than their composite counterparts. Ceramics are also considered to have a greater ability to mask discoloration than resins.17 For an aged tooth with mild discoloration and lots of character, a ceramic veneer may be a reasonable option. For aged and mildly discoloured teeth, areas of intense coloration, spots and craze lines can be incorporated into 0.5–1 mm ceramic veneers, facilitating their integration despite a low thickness. Ceramic veneers may also be appropriate when the teeth or pontics adjacent to the discoloured tooth have ceramic restorations. Using similar materials can help in integrating the appearance of the teeth. Also, if the discoloured tooth is lingually or palatally displaced in relation to the adjacent teeth, then the depth of tooth reduction can be reduced. Figure 5 demonstrates the integration of a minimal preparation ceramic veneer on a displaced tooth with an adjacent metal-ceramic prosthesis.
Figure 5.
(a) The upper left lateral incisor is palatally displaced and adjacent to the upper right central incisor, which is planned as a conventional metal-ceramic bridge abutment. (b) The ceramic veneer on the upper left lateral incisor tooth integrates well with the ceramic of the new bridge and corrects the displacement from the arch.
Limitations
For severe discolorations of single teeth the use of a ceramic veneer is more problematic and is unlikely to provide a satisfactory aesthetic result.18 In order to mask severe discolorations successfully, a thickness of up to 2 mm of glass-ceramic will be required.19 This is particularly destructive if tooth preparation up to 2 mm is required in order to avoid over contouring the veneer. Such tooth reduction would remove the entire layer of enamel in most areas of incisor teeth, particularly cervically, leaving a dentine surface for bonding procedures which is less predictable and more technique sensitive than a bond to enamel.20 If feldspathic porcelains are used, an opacious layer of ceramic is required to mask the underlying discoloration followed by dentine and enamel shades that will integrate with the adjacent teeth, adding to the required depth of preparation. For severely discoloured teeth, it has been suggested to construct veneers with high density alumina cores,21 which are known to exhibit a low transmittance of light,22 using a computer-assisted design/computer-assisted manufacture system. For such veneers, the high density alumina core cannot be etched, unlike feldspathic porcelain and glass ceramic veneers. Accordingly, the bond to the luting resin is less predictable.
For patients with a thin tissue biotype and high lip line, ceramic veneers on discoloured teeth are at risk of aesthetic failure due to gingival recession. In teeth discoloured due to pulp breakdown products, exposure of the tooth root will uncover the darkened roots that will contrast against the bright veneer and give a poor appearance. For patients with thin gingival tissues, failure to address the underlying tooth discoloration through bleaching can also mean a greyish hue can appear apical to the gingival margin. Another reason for this greying of the gingival margin and interdental papillae, in cases where opacious veneers, opacious luting resins or crowns with opaque cores have been used, is related to the lack of light transmission through the crown into the root and out into the surrounding tissues and the shadow created by the upper lip. This has been described as the ‘umbrella effect’.23
Shade communication
In order for the technician to choose the appropriate shade and translucency of ceramic for a veneer or translucent all-ceramic crown, the clinician must communicate to the technician the shade of the underlying veneer or crown preparation, as well as the desired final shade of the restoration. Digital photographs may be of help in this respect. Research of UK general practitioners’ prescriptions for all ceramic crowns has suggested that this is rarely communicated, with 93% of practitioners failing to provide any information on the shade of the prepared tooth stump.24 Ivoclar have created the IPS Natural Die Material shade guide (Ivoclar Vivadent AG, Liechtenstein) (Figure 6) and composite system that allows the clinician to record the shade of the prepared tooth (Figure 7) and communicate this to the laboratory. This aids the technician in finishing and staining the cervical portions of translucent restorations.
Figure 6.
The IPS Natural Die Material shade guide (Ivoclar Vivadent AG, Liechtenstein) that can be used to record the shade of discoloured tooth preparations.Figure 7.
The IPS Natural Die Material shade guide (Ivoclar Vivadent AG, Liechtenstein) being used to record the shade of prepared upper incisor teeth.
Knowing the shade of the tooth preparation and the desired restoration shade, in the case of the EmaxPress ceramic system (Ivoclar Vivadent AG, Liechtenstein), the technician can refer to documentation from the ceramic manufacturer and select the corresponding ceramic shade, opacity, translucency levels and the manufacturing technique. Indeed, it may be that the documentation suggests that the tooth is too severely discoloured for the ceramic to mask the discoloration using a veneer. Other techniques would then need to be considered, including a crown with an opaque layer.
Relative contra-indications
For young patients with highly translucent teeth adjacent to a severely discoloured one, creating a thin veneer with an opaque core/layer that will harmonize well with the adjacent teeth is extremely difficult to achieve. For teeth that are discolored owing to pulp breakdown products in the dentine, the paradox is that the more tooth reduction that is carried out to give a greater thickness of porcelain (to mask the tooth's discoloration), the greater the intensity of discoloration the tooth will have (since the tooth surface is closer to the source of discoloration-pulpal breakdown products).
Effect of luting cement on the overall shade
Opacious luting cements are unable to mask severe tooth discolorations when used with translucent restorations. When cementing the veneer, the thickness of the cement lute is nearly impossible to control accurately. Vichi et al,19 referring to the cement lute, suggested that this parameter can be controlled by the operator only to a certain extent; it cannot be considered as a procedure to correct colour. The authors went on to state that the availability of different cement shades allows only minor aesthetic corrections, which might be instrumentally detectable but are clinically not relevant.19
Survival rates
Porcelain veneers have a relatively good survival rate with a ten-year prospective clinical trial25 showing that, for a single operator, the percentage of veneers that were clinically acceptable without the need for intervention decreased from an average of 92% (95 CI: 90–94%) at 5 years to 64% (95 CI: 51–77%) at 10 years. Similarly, a study that used data from over 80,000 different adult patients treated in NHS general dental practices found that only 53% of veneers survived without re-intervention after 10 years.26 Porcelain fractures and large marginal defects, often associated with discoloration, are commonly reported as reasons for failure of veneers.25
When a veneer fails and is replaced, it has been shown that in circa 20% of cases a crown is the next restoration that the tooth will receive.27 Crowns are clearly more invasive and carry the risk of pulpal death28 and tooth fracture and move the tooth further down the restorative spiral towards extraction.
Full coverage crowns
Full coverage crowns are indicated for discoloured teeth where the teeth are heavily restored, including the use of posts. Crowns become appropriate when more conservative measures, have been unsuccessful in resolving the discoloration. There is a wide variety of materials that can be used for tooth-coloured crown construction, including metal-ceramic and all-ceramic systems (Figure 8).
Figure 8.
(a, b) A range of all-ceramic and metal-ceramic crowns photographed on a mirror to demonstrate their different translucencies. The crowns were made to the same shade decreasing in their translucency from left to right: an Emax lithium disilicate pressed crown, an Incise zirconia core crown, a porcelain fused to metal crown with a porcelain shoulder and a porcelain fused to metal crown with a metal collar.
These crowns will vary in their requirement for depth of tooth reduction, the ability to be etched and resin bonded to tooth structure, their strength, the level of suitable margin placement, the appropriate luting agents and their translucency.
For teeth affected by discoloration, there are principally two choices of crown material types:
Crowns made from a translucent shade of ceramic, such as the lithium disilicate material used in pressed glass-ceramic crowns (Emax, Ivoclar Vivadent, Lichtenstein), can be used to restore discoloured teeth. Such crowns have the advantages of the need for minimal (0.5–1.5 mm) tooth preparation and the ability to be etched and adhesively cemented to unretentive preparations, such as the crown forms found in obliquely fractured or severely worn teeth.
Such translucent crowns can work well for mildly discoloured teeth. However, for teeth with localized areas of more intense discoloration, it has been suggested to perform selective deeper (additional 0.3 mm) tooth preparation, followed by masking the most intensely discoloured regions, using an opaque shade of composite resin blended into the adjacent crown preparation,29 in conjunction with a translucent crown. Etchable, translucent glass-ceramics can be used with supra-gingival chamfered margins, where the cervical portion of the tooth is not unacceptably discoloured. This is advantageous for periodontal health, since it is known that a relationship exists between marginal discrepancy and periodontal tissue inflammation for sub-gingivally located crown margins.30
For more intensely discoloured teeth, translucent crowns are an unpredictable option for achieving an aesthetic crown that will harmonize with adjacent teeth. This is for the same reasons as have been discussed for ceramic veneers; the underlying discoloration will shine through the translucent ceramic. This shine-through of the discoloration is reduced most effectively by increasing the ceramic thickness up to 2 mm,19 which corresponds to aggressive tooth reduction. The use of varying shades of cement has little effect on the final colour at 1.5 mm and none at 2 mm thickness.19 A laboratory study examining 0.8 mm thickness specimens of IPS Empress ceramic found again that cement shade had no effect on the final colour of the restoration.31 Barath et al,32 referring to laboratory testing of Empress 2 (Ivoclar Vivadent AG, Schaan, Liechtenstein) and In-Ceram Alumina (Vita Zahnfabrik, Bad Säckingen, Germany), concluded that no method exists to predict the outcome of an all-ceramic restoration, based on consideration of the luting agent and the background colour.
Opaque crowns
Opaque crowns, whether made of a metal or an all-ceramic material, have the advantage of greater predictability in final colour of the restoration and are better suited to severely discoloured teeth.29 A case of zirconia opaque core all-ceramic crowns being used to mask discoloration of root-treated incisor teeth is demonstrated in Figure 9.
Figure 9.
(a) A patient with a high lip line complains of discoloured margins of the metal ceramic crowns on her upper right central incisor, upper left central incisor and upper left lateral incisor. She is also concerned by the slight black triangle between the upper central incisor teeth, the ‘false looking’ shade of her crowns and the uneven gingival zeniths. (b) The metal-ceramic crowns are removed to reveal proclined underlying teeth giving little depth of veneering porcelain to create a natural appearance. The discoloured upper right central incisor and the upper left lateral incisors are root treated. (c) Following soft tissue surgery to address the uneven gingival levels and a period of provisionalization, zirconium opaque core all-ceramic crowns are placed to address the concerns over the natural appearance of the teeth, and the black triangle.
The drawbacks of such crowns, compared to translucent crowns, include the need for equi-gingival or sub-gingival margins and the risk of periodontal inflammation and gingival recession and slightly deeper tooth preparations, to allow for the thickness of the opaque coping and the veneering ceramic. True resin bonding of such restorations is not possible owing to the inability of metal and highly sintered ceramics to be etched, although tribochemical treatments and adhesive resin-based cements can be used for cementation.33 Zirconia is a popular material choice for an all-ceramic crown core and is available in a range of shades, thicknesses and translucencies, depending on the coping manufacture system used. Although early zirconia copings were very opaque, more modern, thin copings have up to 70% of the translucency value of lithium disilicate glass-ceramic materials,34 and so careful selection of an appropriately opaque coping should be made for the severely discoloured tooth. Figure 10 demonstrates how crowns placed to mask underlying discoloration can face aesthetic failure owing to marginal discoloration and exposure of discoloured root following gingival recession.
Figure 10.
(a) Patient with a high smile line and thin tissue bio-type complains of a discoloured, root-treated upper right lateral incisor and also notes a black line has appeared over time at the margin of the crown on her upper left lateral incisor, which was also a discoloured tooth. (b) Given the treatment options available for the upper right lateral incisor tooth, the patient opts for inside-outside non-vital tooth whitening which produces an aesthetic result. Given the option of a new crown for the upper left lateral incisor, the patient elects to maintain the existing crown for the present time.
The decision to place a crown restoration should not be made lightly, since the negative sequelae of crowns are well known. A study considering the treatment instituted when re-intervention is necessary on a tooth which has previously been crowned, found that 19% of crowned teeth were extracted and/or replaced by a denture as the next intervention.27
Extraction and prosthodontic replacement
For some discoloured teeth, the overall consideration of the endodontic, periodontal and restorability status of the tooth in question may well mean that extraction of the tooth in question, and consideration of the replacement options, is a more economical, efficient and predictable treatment option. When teeth are extracted there are four standard replacement options:
Acceptance of the space;
Provision of a denture;
A conventional or resin-bonded bridge; or
An implant restoration.
Figure 11 demonstrates a case of a gentleman who attended complaining of discoloration of the upper right lateral incisor and intermittent tenderness on biting from the upper right central and lateral incisors. A peri-apical radiograph (Figure 11b) revealed an overprepared root canal system coronally and incomplete orthograde root canal treatment in the upper right lateral incisor. Large retrograde root canal fillings were present in both upper right incisors, with loss of the lamina dura and associated peri-radicular radiolucencies. The diagnosis of chronic peri-radicular periodontitis of the upper right central and lateral incisor was made. The discoloration was thought to be due to a combination of metallic discoloration from corrosion products of the amalgam palatal restoration and pulpal remnant breakdown products. The patient wanted a rapid solution that would relieve the tenderness and correct the discoloration. The poor prognosis of further endodontic intervention on the upper right central and lateral incisors was discussed, as was the limited restorability and lack of structural integrity of the two teeth. The poor prognosis of bleaching severely discoloured teeth with metallic discoloration was also discussed. Given the available options, the patient elected to have the upper right central and lateral incisors removed and replaced by an immediate partial denture. A fixed prosthodontic solution (Figure 11c) was provided following a period of healing.
Figure 11.
(a) Right frontal smile view of the upper anterior dentition and discoloured upper right lateral incisor tooth. (b) Peri-apical radiograph of the upper central incisors and the upper right lateral incisor. (c) Right frontal smile view of the upper anterior dentition following prosthodontic replacement of the upper right central and lateral incisor teeth.
Summary
A variety of treatment strategies may be appropriate for the management of the single discoloured tooth, depending on the diagnosis. In the second of this two part series, direct composite veneers and indirect restorative options have been discussed. The relative advantages and disadvantages of these approaches are outlined in Table 1. Dentists are advised, where possible, after a careful case assessment, to start with minimally invasive treatment strategies, as described in part one. Several management options may be required in combination to obtain satisfactory results in certain cases. Indirect restorative techniques can provide predictable ways of managing the single discoloured tooth, although they come with greater financial cost than direct techniques and greater biological cost in terms of reduction of tooth structure or even removal of the tooth.
Treatment Option
Advantages
Disadvantages
Monitor and review
Low cost, non-invasive option that avoids additional potentially unnecessary treatments.
Only suitable for discoloration that presents post-trauma. Patients must be compliant and temporarily accept the discoloration and accept a degree of uncertainty about its resolution.
Scaling and polishing, air polishing
Scaling and polishing: readily accessible, low cost, low morbidity option effective against extrinsic stains. Allows true assessment of underlying tooth shade and is necessary prior to further procedures such as whitening or adhesive restorations.
Will only treat extrinsic discolorations. Air polishing units not that widely available.
Vital, non-vital whitening techniques
Simple, minimally invasive approach. Rapid results. Preservation of tooth structure.
Patients must be consented and comfortable with a degree of uncertainty over the potential for relapse of discoloration.Ongoing issue over legality of procedures.
Microabrasion, air abrasion, megabrasion
Microabrasion: rapid results. Minimally invasive treatment for superficial internalized intrinsic stains.Air abrasion: rapid superficial intrinsic stain removal.Megabrasion: rapid, low cost. No special equipment required.
Microabrasion: optical characteristics of the tooth altered.Air abrasion: non-selective tooth tissue removal. Dedicated equipment required.Megabrasion: potentially more invasive than an additive masking procedure with direct composite.
Direct composite resin veneer
Low cost, rapid, readily available, repairable, requires minimal or no tooth preparation. Easy maintenance, biological consequences of restoration failure minimal.
Will attract stain more rapidly than ceramic indirect restorations.
Indirect composite resin/ceramic veneer
Ability to harmonize aesthetically with adjacent ceramic/acrylic work. Ability to disguise certain shape irregularities of the underlying discoloured tooth.
Cost of laboratory fee. Unpredictability of final shade when used over deeply discoloured preparations. Tooth preparation required.
Full coverage crown
Predictability of masking underlying discoloration when opaque core crown used.
Destruction of tooth tissue required and consequent detrimental effects on the longevity of the underlying tooth. Risk of aesthetic failure subsequent to gingival recession.
Extraction and prosthodontic replacement
Predictable solution. Removes uncertainty over prognosis for the tooth and correction of its discoloration.
Provisionalization of the space needs careful planning if the patient wants a fixed solution. Requires careful consideration of predictable tooth replacement options. Relatively high costs if dental implant or conventional bridgework planned.