
Abstract
This is the last in a series of three articles on X-ray dose reduction and covers aspects of quality assurance. The first outlined radiation physics and protection and the second the legislation relating to radiation safety.
From Volume 39, Issue 5, June 2012 | Pages 334-339
This is the last in a series of three articles on X-ray dose reduction and covers aspects of quality assurance. The first outlined radiation physics and protection and the second the legislation relating to radiation safety.

A radiograph can be justified when it delivers a net benefit to the patient, ie it helps with diagnosis and/or patient management. This cannot be said of poor quality radiographs, which may yield little or no diagnostic information, and may result in misleading radiographic appearances.
It has been acknowledged, both in the UK and worldwide, that dental radiographs have not always achieved high quality standards, and that this has had a detrimental effect on the quality of patient care.1,2,3 The Ionizing Radiations Regulations 1999 addressed this issue by introducing into the UK a mandatory duty to set up and maintain a quality assurance programme for dental radiographs in whatever setting these were taken.
Quality Assurance (QA) describes ‘that set of activities that are carried out to set standards and to monitor and improve performance so that the care provided will satisfy stated or implied needs.’4 It is a systematic process to check for and, where appropriate, correct errors in the production of dental radiographs to prevent or limit further unsatisfactory images. The aim of a quality control programme is to produce consistently high quality images whilst keeping doses as low as reasonably practicable and, when properly performed, carries benefits to both the patient and the practice because it:
Quality assurance involves all members of the dental team playing his/her part, each having a role by supporting the programme, thus helping to bring about an improvement in radiographic quality. A basic principle of a quality assurance programme is that all necessary procedures should be laid down in writing, clearly identifying:
A QA programme involves not only the implementation of quality control procedures, but also the mechanism to ensure these are monitored, evaluated and that necessary corrective action is taken. The programme can be broken down into the following sections:
Staff education and training is the bedrock of high quality radiography through essential theoretic knowledge coupled with expert practical training and assessment. Thorough training ensures that radiographic techniques are employed to a high standard so that operator errors, such as poor film or patient positioning, inadequate patient instruction, and incorrect choice of exposure factors are kept to a minimum. The IR(ME) R 2000 regulations require both practitioners and operators to be ‘adequately trained’. Undergraduate students should receive appropriate theoretical education and practical training in line with that documented by the British Society of Dental and Maxillofacial Radiology (BSDMFR),5 and subsequently undertake continuing education during the remainder of their practising life. For all dentists and dental care professionals involved in the radiographic process this should include at least 5 hours of verifiable CPD undertaken every 5 years at an appropriate course.
A register should be kept of all the staff involved in radiography which makes clear:
This information forms part of the QA log and fulfils a requirement of IRR 99 and IR(ME)R 2000.
Quality assurance applied to ‘working procedures’ is designed to ensure that all documentation related to legislation and patient protection is kept up-to-date. These documents are kept in the Radiation Protection File, along with operational procedures and a procedures log, to comply with IR(ME)R 2000. They should contain all the essential pieces of information relevant to the local X-ray installation for its safe use.
The other important component of the Radiation Protection File is the Local Rules (see article 2). Operational procedures include lists of instructions on how to carry out tasks that may have an effect on patient safety (eg correct preparation of processing chemicals, monitoring image quality). A procedures log keeps track of all written radiographic procedures recording if and when these are reviewed and/or updated.
The log book is an essential QA tool – use it to keep an inventory of X-ray equipment, its location and details of its maintenance.
Note that, on installation, the installer (an agent of the manufacturer) will give a written ‘Critical Examination’ report on the equipment, which you will need to keep, but an independent ‘Acceptance Test’ is also necessary – normally arranged through your Radiation Protection Advisor (RPA). This is an important preliminary safety check, and will confirm that the X-ray machine has sufficient filtration, is appropriately collimated, delivers accurately timed exposures and will test the radiation dose delivered for a typical radiograph, eg a lower molar periapical radiograph. The latter assessment will allow comparison with Diagnostic Reference Levels (DRLs – see article 2) and give baseline information against which results of subsequent routine tests can be compared. The ‘acceptance test’ will need to be repeated if an X-ray machine is altered or its permanent location is moved. Again, keep the results in your records.
Simple checks should be part of your daily routine for monitoring your X-ray equipment, such as lack of stability in the X-ray tube head support arm or failure of the audible and visible X-ray exposure warning signals.
The X-ray set should undergo a routine radiation safety test as well as servicing, as recommended by the manufacturer, and is usually undertaken annually. If the set develops a fault, for example the dental X-ray tube head does not stay in the desired position, or the panoramic set delivers distorted images, an appropriate engineer should be called to investigate and rectify the problem.
Modern dental radiography has embraced digital radiography along with other innovations in computerization and imaging in dentistry. Quality assurance applies equally to either film-based or digital systems.
Film is supplied with QA standards from the manufacturers. A QA programme in this regard might include adoption of these standards, which would recommend the long-term storage of film in a cool, dry environment (not, for example, in the loading bay of a processor), with stock control to ensure use before the expiry date and careful handling away from any light or X-ray sources. One should record the location of the film store, keep records of stock control and any specific requirements for film handling.
Follow manufacturer's advice on cleaning and maintenance of intensifying screens and cassettes. A QA programme may include a policy of how and when to clean intensifying screens which, if dirty or damaged, result in white spots or artefacts on the processed image (Figure 1). Periodically test for cassette light-tightness by placing an unexposed film in the cassette for several minutes before processing. No film fogging (blackening) should be observed.

An un-sharp image can result from poor film/screen contact due to worn cassette hinges or locks. This problem can be assessed by exposing a film and graph paper in the cassette and checking for sharpness of the grid lines on the image. Adopt a policy of numbering individual cassettes to assist in identification in case of errors or problems.
This may be undertaken manually in a darkroom but is now more commonly performed using an automatic processor. QA standards would be guided by the suppliers of processing chemicals and processor manufacturer's recommendations. The QA log includes:
To help keep the rollers clean, a blank film can be run through the automatic processor at the start of each day to pick up residues left on the transport mechanism.
Quality control tests should include a ‘coin test’, especially when suspecting light leakage within the daylight loader or darkroom to cause film fogging, resulting in a dark area on the film. It consists of placing three coins on an undeveloped film under safe light conditions in the processor's daylight hood and sequentially removing one coin every 20 seconds, then processing the resultant film. A circular image of the coin seen after removing the first coin indicates that there is less than 20 seconds before film fogging has occurred. If no coin images are seen on the processed film after 60 seconds, when all three coins have been removed, then the safe working time is at least 60 seconds.
Developer solution will lose efficiency imperceptibly, even when no films are processed, and thus the dentist may be unaware of loss of image contrast and density. To monitor film development, a ‘step-wedge’ test is necessary. This test is designed to monitor the quality of the developing solution for deterioration, and indicates when the solution must be replaced. The test can be simple, but more sophisticated versions of this principle are preferred which use densitometry and sensitometry.
The basis of this test is to acquire an excellent quality reference film, using freshly prepared processing solutions, against which subsequently processed films can be compared. It can be created by taking a radiograph using a standard exposure and tube position of a test object, such as a tongue spatula on which three or four stepped layers (different thicknesses) of lead foil have been mounted or, alternatively, imaging a radiographic aluminium step wedge.
This first film is processed in newly made processing solutions at the correct temperature and for the correct time. The chemistry is then used as normal, and films of the test object taken and processed daily thereafter. Careful observation should identify when subsequent films first become noticeably different in density from the reference film, and this indicates the need to change the chemicals.
Alternatively, commercially available pre-exposed film strips are processed on a daily basis and analysed with a film reader, which indicates when the developer solution requires changing (Figure 2). This method provides an accurate, uniform and quantifiable quality control test.6

Quality assurance is as important and applicable here as for conventional dental film-based imaging. Whilst eliminating chemical processing problems, new areas of error have been introduced. Quality assurance plays a part here in creating and maintaining uniformly good digital image quality.
Digital dental imaging is now acquired through one of two technologies:
For further reading on the formation and manipulation of dental digital images, 21st Century Imaging by Horner, Drage and Brettle is recommended.7
Potential sources of error for CCD/CMOS sensor systems include:
Potential sources of error for photo-stimulable phosphor (PSP) plate systems include:

Clinical decisions are often made by examining the images on a monitor, thus it is important to ensure that the viewing conditions are appropriate for accurate assessment. The monitor should be placed out of direct sunlight and in a darkened room with a light level of 50 to 100 lux (the lux is the SI unit of luminance). This level is similar to room light levels experienced indoors on an overcast day, whereas office lighting levels are typically around 300 to 500 lux. If it is not possible to move the monitor away from direct sunlight, consider making a hood to shield the screen.
In addition, as part of the quality assurance programme, the monitor should be checked for brightness, contrast, resolution and geometric distortion. The screen should be appropriately set up for optimal viewing by the manufacturer on installation. Subsequent deterioration of image quality can be assessed using a standard image (test card) made up of lines and various grey scales. One such test card has been devised by the Society of Motion Picture and Television Engineers (SMPTE), which can be downloaded from the internet.8 Another is the TG18-QC test image, also available on the web. These images can be used every 3 months or so to evaluate monitor resolution and contrast.
Quality assessment of images is central to a QA programme, and should incorporate a clearly defined mechanism for:
The key elements of image quality assessment are:
| Rating | Quality | Basis of decision |
|---|---|---|
| 1 | Excellent | No errors of exposure, positioning or processing |
| 2 | Diagnostically acceptable | Some errors of exposure, positioning or processing but which do not detract from the diagnostic utility of the radiograph |
| 3 | Unacceptable | Errors of exposure, processing or positioning which render radiograph diagnostically unacceptable |
| Rating | Percentage of radiographs taken |
|---|---|
| 1 | Not less than 70% |
| 2 | No greater than 20% |
| 3 | No greater than 10% |
Film reject analysis – analyse the reasons for Grade 3 or reject films, as this may help identify particular problem areas, and where improvements are most urgently needed. Earlier issues of this journal contain a good guide to film fault analysis and making quality improvements.10,11
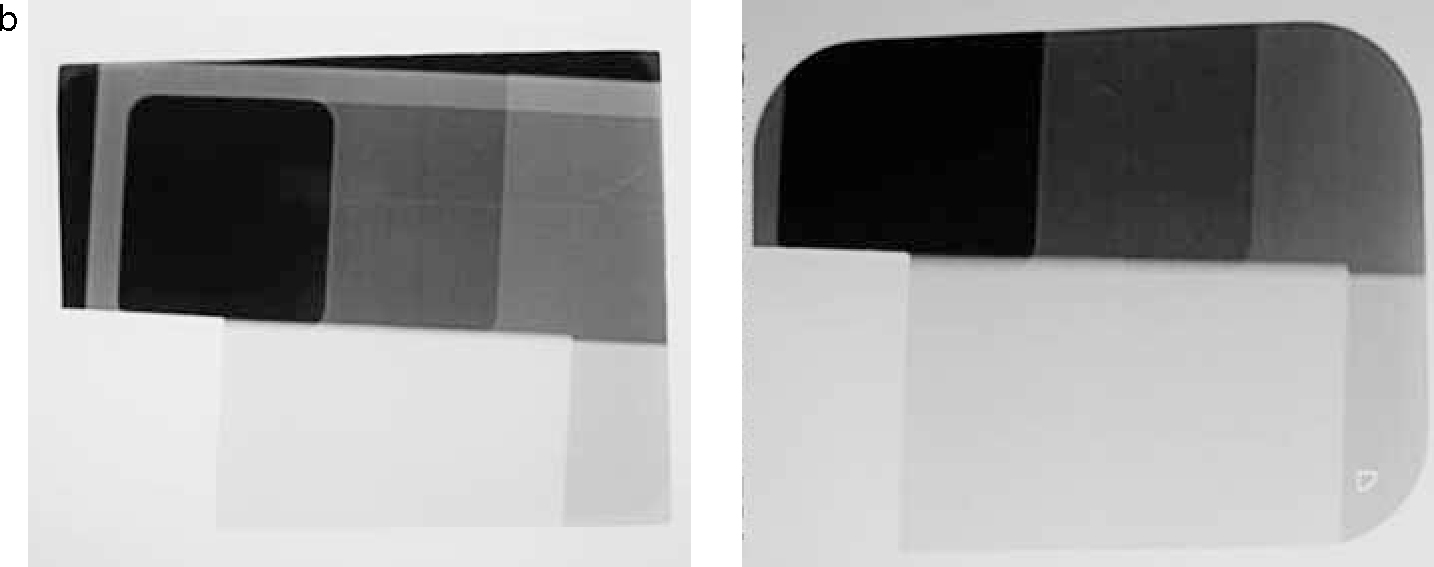
The company Leeds Test Objects have produced a step test object suitable for assessing intra-oral digital sensors. The principle is similar to that for film in that a grey scale image is produced using the stepped test object as shown in Figure 4a, but the exposure times are varied so that the operator, by observing the grey shades (Figure 4b), can select, for example, the exposure time that shows dental caries most clearly.

Audit is an excellent tool for bringing about an improvement in healthcare. Quality assurance in dental radiography lends itself very well to the audit process, since standards exist for quality targets in dental radiography which can be audited against (see above).9 By recording the total number of radiographs taken within a given time and calculating the percentage of films in each grade category, a ready comparison can be made with these published targets. The most important next step is to close the audit loop by looking for the cause of any problems identified in the comparison process, making changes to eliminate these problems and then re-auditing to see whether the instigated changes have had a beneficial effect.
Thus audit is the culmination of the process of Quality Assurance, and should ultimately help to confirm the benefit brought about by the instigation of such a programme.